多层螺旋CT灌注成像在早期急性坏死性胰腺炎的临床应用
2016-06-20毛景松沈阳市第五人民医院放射科辽宁沈阳110023
毛景松沈阳市第五人民医院放射科,辽宁沈阳 110023
多层螺旋CT灌注成像在早期急性坏死性胰腺炎的临床应用
毛景松
沈阳市第五人民医院放射科,辽宁沈阳110023
[摘要]目的探讨CT灌注成像在早期急性坏死性胰腺炎中的应用。方法45例胰腺炎患者被分成轻型胰腺炎(n=26)及坏死性胰腺炎(n=19)两组,给予胰腺灌注扫描,比较两组CT灌注参数BF、BV、MTT、PS并进行统计学分析;3周后,胰腺炎患者予常规增强CT扫描,判断灌注扫描对怀疑胰腺坏死的敏感性及特异性。结果坏死性胰腺炎患者的BF和BV水平显著低于轻型胰腺炎组,差异具有统计学意义(P<0.05);MTT和PS水平两组比较,差异无统计学意义(P>0.05)。45例胰腺炎患者,CT灌注怀疑19例胰腺坏死,3周后复查CT增强检查,19例胰腺坏死中的17例出现阳性,2例出现假阳性,灌注排除坏死的患者中未出现胰腺坏死病例,敏感性为100.0%,特异性为93.3%。结论CT灌注成像对早期急性坏死性胰腺炎有较高的敏感性。
[关键词]急性胰腺炎;计算机断层;灌注;胰腺坏死
急性胰腺炎(AP)是常见的急腹症之一,急性胰腺炎患者中大部分为轻症胰腺炎(MAP)患者,预后较好,而急性坏死性胰腺炎(ANP)患者症状重,常常是致命的,其死亡率高达32%。急性胰腺炎,特别是坏死性胰腺炎的早期治疗对提高生存率是必要的。然而由于没有方法评估其严重程度,早期治疗常被延误。现在国内外的专家多用CT灌注成像评估胰腺疾病,本研究主要回顾我院2013年5月~2015年6月收治的45例急性胰腺炎患者,用CT灌注扫描评估其严重程度及胰腺坏死的形成。现报道如下。
1 资料与方法
1.1临床资料
选择2013年5月~2015年6月我院收治的45例胰腺炎患者,纳入标准:临床症状体征及实验室检查结果符合急性胰腺炎的诊断标准;经两名影像医师独立阅片,影像支持胰腺炎的诊断。排除标准:合并有心血管、肝肾、造血系统等严重原发病者;由于外伤、手术、肿瘤所致的急性胰腺炎患者;碘剂严重过敏者。按照全国胰腺疾病学组制订的《中国急性胰腺炎诊治指南(草案)》的诊断标准分为轻型胰腺炎(MAP)26例(A组)和坏死性胰腺炎(ANP)19例(B组)。A组男18例,女8例,年龄(46.3±8.6)岁;B组男15例,女4例,年龄(45.6±6.9)岁,两组的性别、年龄之间比较差异无统计学意义(P>0.05),具有可比性。
1.2方法
多层螺旋CT灌注成像:两组患者入院3 d内,采取GE hispeed 16层螺旋CT进行动态灌注扫描。所有病例均取仰卧位,常规腹部CT平扫,层厚、层间距、螺距分别为5、5、1.375 mm,选择胰腺显示最完整的层面作为灌注扫描层面,管电压、管电流分别为100 kV、80 mA,应用非离子对比剂欧乃派克(350 g/L)100 mL,高压注射速率为4.5 mL/s,注射50 mL,延迟8 s开始扫描,嘱患者扫描前屏住呼吸,扫描时长约30 s。灌注扫描结束后,再注射欧乃派克50 mL,进行常规胰腺增强扫描。最后在CT工作站上通过利用ADW4.3软件的Perfusion3,进行图像分析和数据处理,得到胰腺CT灌注参数:血流速度(blood flow,BF)、血容量(blood volume,BV)、平均通过时间(mean to time,MTT)、表面通透性(permeability surface,PS)。
1.3胰腺坏死的诊断
在BF灌注图像上,颜色缺失或BF值明显低于胰腺组织,为CT灌注怀疑胰腺坏死;3周后,予常规胰腺增强检查,根据增强CT影像表现,双期持续存在的胰腺实质无强化的不规则形低密度区,与周围强化的胰腺组织形成明显的密度差,明确胰腺坏死[16]。
1.4统计学处理
2 结果
2.1两组胰腺炎灌注参数比较
B组患者BF和BV水平显著低于A组,差异具有统计学意义(P<0.05);MTT和PS水平比较,差异无统计学意义(P>0.05),见表1。
2.2CT灌注成像诊断胰腺坏死的敏感性及特异性
45例胰腺炎患者中,CT灌注怀疑19例胰腺坏死(BF灌注图像明显低于正常组织),见封三图7。3周后复查CT增强检查,19例怀疑胰腺坏死中的17例出现阳性,2例出现假阳性,灌注排除坏死的患者中未出现胰腺坏死,敏感性为100.0%,特异性为93.3%。
3 讨论
急性胰腺炎的诊断依据:①临床症状;②生化;③CT影像诊断[1,2]。急性胰腺炎是内科中较为严重的疾病。全世界急性胰腺炎的死亡率2.1%~9.2%,坏死性胰腺炎的发病率在胰腺炎中占10%~15%,死亡率占23%[3]。急性坏死性胰腺炎早期不易发现,有报道称多层螺旋增强CT对比兰森评分系统,急性生理学及慢性健康评分系统预测坏死性胰腺炎较准确[4],但由于增强CT在预测急性坏死性胰腺炎早期的低敏感性,急性胰腺炎临床指导建议3 d后行增强CT扫描[5]。CT灌注扫描可用于3 d内检查,且对坏死性胰腺炎的敏感性及特异性分别为100.0%及95.3%[6],与本研究结果相近。CT灌注技术在一定程度上能反映器官组织的血流动力学状态和功能情况[7,8],可以反映组织器官的微血管变化,表现其灌注量的增加,参数反映了与血管生成相一致的微观生理改变。胰腺是一个血供较丰富的器官,测量胰腺的血流灌注对于胰腺疾病的诊断有重要的作用[9-12]。本研究显示,急性胰腺炎的发展的早期轻型胰腺炎与坏死性胰腺炎比较,CT灌注参数BF、BV显著下降,两者差异有统计学意义(P<0.05)。
表1 A B两组胰腺炎的灌注参数比较(±s)
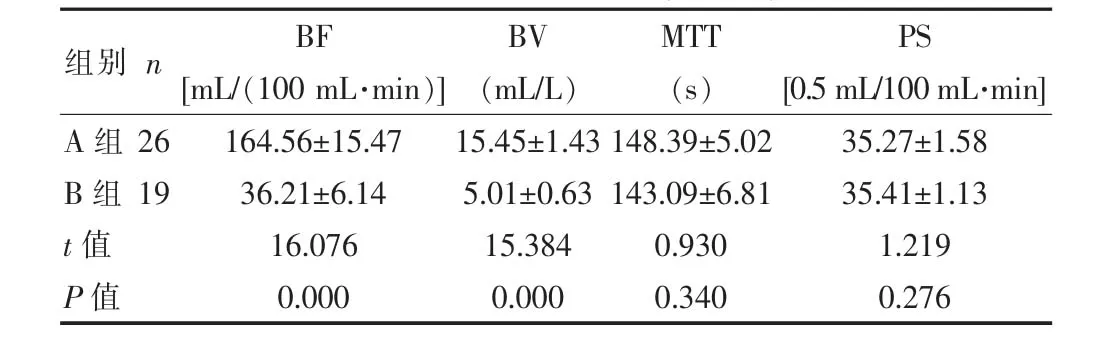
表1 A B两组胰腺炎的灌注参数比较(±s)
164.56±15.47 36.21±6.14 16.076 0.000 15.45±1.43 5.01±0.63 15.384 0.000 148.39±5.02 143.09±6.81 0.930 0.340 35.27±1.58 35.41±1.13 1.219 0.276 BF [mL/(100 mL·min)] BV (mL/L)MTT (s)PS [0.5 mL/100 mL·min] A组B组t值P值26 19组别n
胰腺坏死是因供应胰腺的血管痉挛引起的[13,14],血管造影是目前唯一诊断血管痉挛的检查方法,但血管造影在不稳定及急诊病例中进行比较困难,因此应用CT灌注扫描诊断胰腺组织的缺血。Yoshihisa等[15]认为,CT灌注扫描在诊断胰腺坏死方面优于血管造影,同时CT灌注怀疑胰腺坏死的患者中坏死发病率较高,相反,阴性可以排除胰腺坏死的可能。国外也有学者认为BF值的下降超过19.3%,提示胰腺组织坏死[16]。本研究中,在胰腺灌注高度怀疑坏死的患者中,3周后复查,7例患者出现胰腺坏死,1例患者没有出现坏死,在灌注排除胰腺坏死的患者中,没有出现一例坏死病例,与相关研究结果相一致。
综上所述,急性坏死性胰腺炎的早期诊断对疗效非常重要,然而,现在的方法预测早期坏死性胰腺炎是较困难的[17,18],CT灌注对诊断早期坏死性胰腺炎有很大帮助。早期诊断有助于临床医师加强对病情的判断与早期对坏死性胰腺炎进行干预,减少并发症发生率,提高患者生存率[5]。
[参考文献]
[1] Peter A,Banks Martin,L Freeman,et al. Practice guidelines in acute pancreatitis[J]. Gastroenterol,2006,10(1):2379-2400.
[2] Seiki Kiriyama,Toshifumi Gabata,Tadahiro Takada,et al. New diagnostic criteria of acute pancreatitis[J]. Hepatobiliary Pancreat Sci,2010,5(17):24-36 .
[3] M Sekimoto,T Takada,Y Kawarada,et al. JPN Guidelines for the manangement of acute pancreatitis:Epidemiology,etiology,natural history,and outcome predictors in acute pancreatitis[J].Journalof Hepato-Biliary-Pancreatic Surgery,2006,1(13):10-24.
[4] TK Leung,CM Lee,SY Lin,et al. Balthazar computed tomography severity index is superior to Ranson criteria and APACHEⅡscoring system in predicting acute pancreatitis outcome[J]. World Journal of Gastroenterology,2005,38 (11):6049-6052.
[5] M Piascik,G Rydzewska,J Milewski,et al. The results of severe acute pancreatitis treatment with continuous regional arterial infusion of protease inhibitor and antibiotic:A randomized controlled study[J]. Pancreas,2010,6(12):863-867.
[6] Li HO,Sun C,Xu ZD,et al. Low-dose whole organ CT perfusion of the pancreas:Preliminary study[J]. Abdom Imaging,2014,39(1):40-47.
[7]张根山,祖茂衡,袁刚,等. CT灌注成像及血管内皮生长因子检测对肝癌灌注栓塞血供评价的研究[J].当代医学,2012,27(18):74-76.
[8]侯斐,刘瑞霞,阴赪宏.急性胰腺炎微循环障碍的发生机制及其治疗进展[J].临床肝胆病杂志,2014,30(8):815-818.
[9]马晓璇,石惠平,郭薇,等.全器官CT灌注成像评价胰腺癌微循环的价值[J].中国医学影像学杂志,2013,6(21):439-443.
[10]蒋洪涛,陈柱,肖恩华. CT灌注成像原理及其在急性胰腺炎中的临床应用[J].中国CT和MRI杂志,2014,7(12):109-111.
[11]刘倩倩,黄小华,董国礼,等.多层螺旋CT灌注成像在胰腺癌诊断中的应用价值[J].中华临床医师杂志(电子版),2014,8(14):2613-2618.
[12] D'Onofrio M,Gallotti A,Mantovani W,et al. Perfusion CT can predict tumoral grading of pancreatic adenocarcinoma[J]. European Journal of Radiology,2013,82(2):227-233.
[13] Takeda K,Mikami Y,Fukuyama S,et al. Pancreatic ischemia associated with vasospasm in the early phase of human acute necrotizing pancreatitis[J]. Pancreas,2005,30 (2):40-49.
[14] Inoue K,Hirota M,Beppu T,et al. Angiographic features in acute pancreatitis:The severity of abdominal vessel ischemic change reflects the severity of acute pancreatitis[J]. JOP,2003,4(10):207-213.
[15] Yoshihisa Tsuji. Perfusion CT is superior to angiography in predicting pancreatic necrosis in patients with severe acute pancreatits[J]. Gastroenterol,2010,5(45):1155-1162.
[16] Yoshihisa Tsuji,Naoki Takahashi,Chiba Tsutomu,et al. Pancreatic perfusion CT in early stage of severe acute pancreatitis[J]. International Journal of Inammation,2012,10(11):1-5.
[17] Bollen TL,Van Santvoort HC,MG Besselink,et al. The Atlanta Classication of acute pancreatitis revisited[J]. British Journal of Surgery,2008,95(1):16-21.
[18] Chauhan S,Forsmark CE. The diculty in predicting outcome in acute pancreatitis[J]. American Journal of Gastroenterology,2010,2(10):443-445.
Clinical application of multi-slice CT perfusion imaging in early stage of acute necrotizing pancreatitis
MAO Jingsong
Department of Radiology, the Fifth People's Hospital of Shenyang City,Shenyang 110023,China
[Abstract]Objective To investigate the perfusion changes associated with acute necrotizong pancreatitis(ANP) at an early age using the multi-slice computed tomograohy (CT) perfusion imaging. Methods A total of 45 patients with acute pancreatitis underwent CT perfusion imaging were divided into two groups, 26 patients with mild AP (MAP) and 19 pa tients with ANP. The CT perfusion parameters including blood flow(BF), blood volume (BV), mean transit time (MTT) and permeability-surface area product (PS) were compared, and the correlation between the parameters was analyzed in statistic. After three weeks, all the patients underwent conventional contrast-enhanced CT scan, to judge the sensitivity and specificity of perfusion image in the patients with pancreatic necrosis. Results The levels of BF and BV for the ANP group were significantly lower than those for MAP group(P<0.05); The levels of PS and MTT were not statistically significant (P>0.05). 19 patients were diagnosed with ANP by using CT perfusion, of which, 17 patients were confirmed by conventional contrast-enhanced CT scan after 3 weeks. All the patients who had no perfusion defects detected in the perfusion CT image were diagnosed with mild AP 3 weeks later. The sensibility and specificity of diagnosing the early ANP by using the perfusion CT was 100.0% and 93.3%, separately. Conclusion Perfusion CT was more sensitive in diagnosing ANP at an early stage.
[Key words]Acute pancreatitis; Multi-slice spiral CT; Perfusion; Pancreatic necrosis
[中图分类号]R576;R816.5
[文献标识码]B
[文章编号]1673-9701(2016)03-0107-03
收稿日期:(2015-07-31)
