肝移植术后血清降钙素原同肺部感染关系探讨
2016-03-23谭青海
谭青海,谷 晔
肝移植术后血清降钙素原同肺部感染关系探讨
谭青海,谷晔
【摘要】目的探讨血清降钙素原(procalcitonin,PCT)在肝移植术后并发肺部感染诊断中的临床意义。方法检测165例肝移植患者术后血清PCT水平,观察其在并发肺部感染与否患者中的差异,以及不同病因与PCT值的关系。结果 肝移植术后感染组PCT水平显著高于非感染组(t=2.05,P=0.047)。在165例肝移植患者中,前三位病因分别为肝恶性肿瘤、肝炎后肝硬化与酒精性肝硬化。比较前三个病因中感染组与非感染组PCT水平:肝恶性肿瘤、酒精性肝硬化患者术后感染组与非感染组PCT水平比较,差异无统计学意义;肝炎后肝硬化患者术后感染组PCT水平显著高于非感染组(t=2.40,P=0.034)。结论血清PCT监测有助于肝移植术后感染的早期诊断,肝恶性肿瘤与酒精性肝硬化患者需要动态监测PCT值并结合炎性反应指标判断感染。
【关键词】肝移植;降钙素原;感染
【中国图书分类号】R617
作者单位: 100039北京,武警总医院呼吸内科
肝移植手术是治疗终末期肝病的有效方法,而感染是影响手术成功与否的关键因素之一[1]。患者病情重,加之手术和大量免疫抑制药、激素、抗排异药的使用,造成其免疫力低下,抗感染能力下降,所以早期诊断患者术后是否合并感染尤为重要。PCT由细菌毒素和炎性因子诱导产生,研究认为其有助于肝移植术后感染的早期诊断及鉴别诊断,并可作为判断预后的指标[2]。本研究对165例肝移植患者进行术后6 h内血清PCT检测,探讨血清PCT在肝移植术后并发感染诊断中的临床意义,同时观察不同病因导致的肝脏疾病与术后PCT水平的关系。
1 资料与方法
1.1一般资料2014-01至2015-11在武警某部三甲医院呼吸内科行同种异体肝脏移植术后并发肺部感染患者85例,男64例,女21例,年龄1~72岁,平均(49.36±13.44)岁;非感染患者80例,男66例,女14例,年龄1~65岁,平均(47.36±12.34)岁。组间一般资料年龄、性别比较,差异均无统计学意义。
1.2诊断标准肺部感染患者早期常见症状有发热、咳嗽、肺部啰音或术后早期呼吸机辅助呼吸导致血氧饱和度低;对比术前,术后床旁胸部X线片显示不同程度的片状、斑片浸润性阴影或间质性改变,伴或不伴胸腔积液。在上述临床诊断基础上,符合下列条件之一者,即可确诊为细菌性肺炎:(1)经筛选的痰标本,连续2次分离出相同病原菌;(2)经纤维支气管镜或人工气道,防污染样本毛刷采样或支气管肺泡灌洗分离致病菌≥108 cfu/ml;(3)痰定量培养病原菌浓度≥109 cfu/ml。
1.3检测方法患者签署知情同意书,肝移植术后6 h内采集静脉血5 ml,真空静置,在采血后30 min内4000 r/min离心10 min。PCT检测采用免疫层析法(全血型),用武汉明德生物科技股份有限公司生产的免疫定量分析仪检测,试剂盒也为该公司提供。标本检测严格按照试剂盒说明书进行。
1.4统计学处理采用SPSS 17.0软件进行统计分析,计数资料以频数表示,组间比较采用χ2检验;计量资料以±s描述,组间比较采用两独立样本t检验,以P<0.05为差异有统计学意义。
2 结 果
2.1肝移植患者术后感染组与非感染组PCT水平比较肝移植患者术后感染组与非感染组PCT水平分别为(32.86±18.03)、(18.12±17.73)ng/ml,两组比较差异有统计学意义(t=2.050,P=0.047)。
2.2不同病因对PCT值的影响在165例肝移植患者中,不同病因感染与非感染患者频数分布见表1,其中排名前3位病因为肝恶性肿瘤、肝炎后肝硬化与酒精性肝硬化。比较前3个病因中感染组与非感染组PCT水平(表2):肝恶性肿瘤、酒精性肝硬化患者术后感染与非感染组PCT水平比较,差异无统计学意义;而肝炎后肝硬化患者术后感染与非感染组PCT水平比较,差异有统计学意义(t=2.403,P=0.034)。
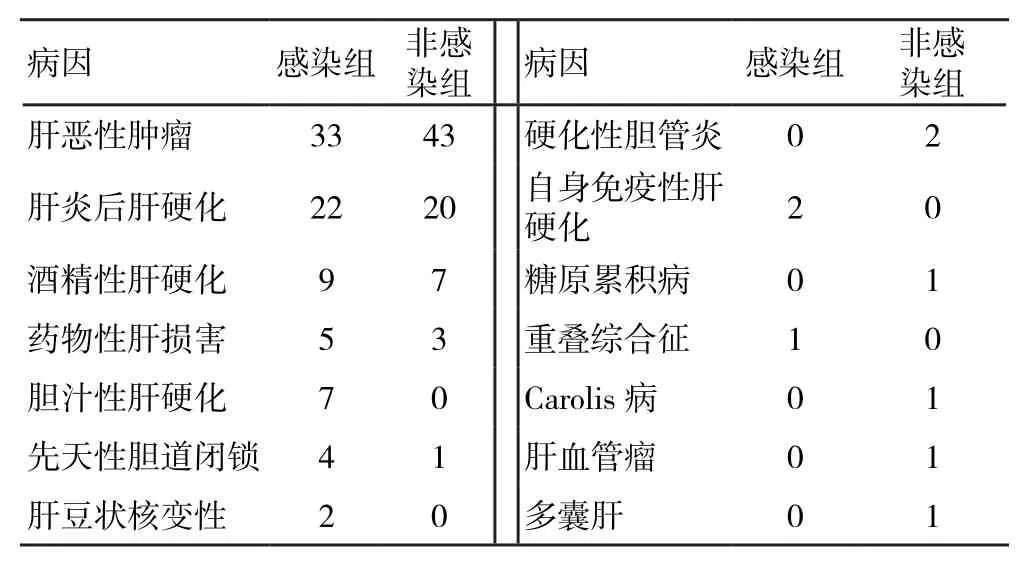
表1 不同病因感染与非感染组频数分布

表2 不同病因肝移植患者感染组与非感染组PCT水平比较
3 讨 论
PCT是一种蛋白质,可反映全身炎性反应的活跃程度,正常健康人血清PCT水平极低,几乎不能被检测到,但重症感染患者血清PCT水平可成倍升高[3]。影响PCT水平的因素包括被感染器官的大小和类型、细菌种类、炎性反应程度和免疫反应状况。严重细菌、真菌、寄生虫感染,以及脓毒症和多脏器功能衰竭,PCT在血浆中的浓度会升高;自身免疫反应、过敏和病毒感染时PCT水平不会升高;局部有限的细菌感染、轻微的感染和慢性炎性反应也不会导致其升高。感染时PCT的主要来源是实质组织细胞。肝移植手术创伤大,同时存在肝短暂缺血引发的再灌注损伤,肠黏膜也会因为缺血导致屏障功能障碍,肠道内毒素移位,白细胞介素-6等炎性介质释放增多,均可引起术后PCT水平升高[4]。但肝移植受者的PCT水平只在移植后早期短暂升高,随后迅速下降[5]。而肝移植术后如出现感染并发症,PCT水平会持续或者再次升高[6-7],支持本研究结果肝移植术后感染组PCT水平显著高于非感染组。同时,有研究报道血清PCT水平还可以作为评价肝移植预后的指标[8-10]。
目前关于PCT对肝硬化诊断价值的研究较少,Connert等[11]发现失代偿期肝硬化感染组与非感染组血清PCT水平有明显差异,当以PCT≥0.58 ng/ml为诊断感染阈值时,其敏感度为92%,特异性为78%;而Bota等[12]研究表明在肝硬化患者中,PCT水平在感染组与非感染组无显著差异。本研究将肝硬化进一步细分肝炎后肝硬化和酒精性肝硬化,结果显示肝炎后肝硬化患者感染与非感染组PCT水平比较,差异有统计学意义,而在酒精性肝硬化中两组无差异,但本研究中纳入酒精性肝硬化病例数较少,因此还需要下一步增加病例数进行分析。对于肿瘤是否影响PCT对感染的判断,近年来研究较多,但是否存在实体肿瘤细胞产生PCT,目前还不明确[13]。Hangai等[14]研究甲状腺恶性肿瘤及血液系统恶性肿瘤发现,在非感染患者中PCT水平也较正常人升高;Shomali等[15]也证实在肿瘤性发热和血液感染发热患者中PCT水平无显著差异。这些均表明肿瘤会影响PCT水平,本研究发现在肝恶性肿瘤患者感染组与非感染组PCT水平无显著差异,证实了上述结论。
本研究也存在一定的局限性,手术时间长短、供体是否存在感染,以及其他慢性肝脏疾病、手术过程中激素等免疫抑制药的使用,这些因素都可能影响术后PCT值[16,17], 另外,由于资料是回顾性临床病例资料,PCT值是孤立值,使用免疫层析法快速检测同双抗夹心免疫化学发光法比较偏差较大[18],也可能造成PCT出现偏大值。未来还需进行更深入、广泛的因素研究,以提高研究的解释力。
可以肯定的是,肝移植患者术后早期监测感染至关重要,所以要动态监测PCT值,联合C反应蛋白、白细胞介素-8等炎性反应指标,合理调整抗生素使用,减少耐药性细菌产生,特别是对重症患者及肝恶性肿瘤与酒精性肝硬化患者。
【参考文献】
[ 1 ]Perrakis A, Yedibela S, Schellerer V, et al. Procalcitonin in the setting of complicated postoperative course after liver transplantation [J]. Transplant Proc, 2010, 42(10): 4187-4190.
[ 2 ]Chen J,Wang Y,Shen Z,et al. Early diagnostic value of plasma PCT and BG assay for CRBSI after OLT [J]. Transplant Proc, 2011, 43(5): 1777-1779.
[ 3 ]Kaido T, Oguwa K, Fujimoto Y, et al. Perioperative changes of procalcitonin levels in patients undergoing liver transplantation [J]. Transpl Infect Dis, 2014, 16(5): 790-796.
[ 4 ]Jensen J U, Lundgren J D. Procalcitonin in liver transplant patients-yet another stone turned [J]. Crit Care, 2008, 12 (1): 1-2.
[ 5 ]Elefsiniotis I S, Skounakis M, Vezali E, et al. Clinical significance of serum procalcitonin levels inpatients with acute or chronic liver disease [J]. Eur J Gastroenterol Hepatol, 2006, 18(5): 525-530.
[ 6 ]Busuttil R W, TanakaK. The utility of marginal donors in liver transplantation [J]. Liver Transpl, 2003, 9(7): 651-663.
[ 7 ]Eyraud D,Ben Ayed S,Tanguy M L,et al. Procalcitonin in liver transplantation: are high levels due to donors or recipients? [J]. Crit Care, 2008, 12(4): 321.
[ 8 ]Wilson D J, Fischer A, Das K, et al. Donors with cardiac arrest: improvedorgan recovery but no preconditioning benefit in liver allograft [J]. Transplantation, 2003, 75 (10): 1683-1687.
[ 9 ]Van den Broek M A,Olde Damink S W,Winkens B,et al. Procalcitonin as a prognostic marker for infectious complications in liver transplant recipients in an intensive care unit [J]. Liver Transpl, 2010, 16(3): 402-410.
[10]曾兰兰,石玉玲,廖 扬,等. 动态监测降钙素原对肝移植患者感染预后判断的意义[J]. 生物技术通讯, 2010, 21(1): 77-79.
[11]Connert S, Stremmel W, Elsing C. Procalcitonin is a valid marker of infection in decompensated cirrhosis [J]. Z Gastroenterod, 2003, 41(2): 165-170.
[12]Bota D P, Van Nuffelen M, Zakarish A N, et al. Serum levels of C-reactive protein and procalcitonin in critically ill patients with cirrhosis of the liver [J]. J lab Clin Med, 2005, 146(6): 347-351.
[13]Thorn R M, Reynolds D M, Greenman J. Multivariate analysis of bacterial volatile compound profiles for discrimination between selected species and strains in vitro [J]. J Microbiol Methods, 2011, 84(2): 258-264.
[14]Hangai S, Nannya Y, Kurokawa M. Role of procalcitonin and C-reactive protein for discrimination between tumor fever and infection in patients with hematological diseases [J]. Leuk Lymphoma, 2015, 56(4): 910-914.
[15]Shomali W, Hachem R, Chaftari A M, et al. Can procalcitonin distinguish infectious fever from tumorrelated fever in nonneutropenic cancer patients? [J]. Cancer, 2012, 118(23): 5823-5829.
[16]Korczowskki B. Serum procalcitonin concentration in children with liver disease [J]. Pediatr Infect Dis J, 2006, 25(3): 268-269.
[17]Zazula R, Prucha M,Tyll T, et al. Induction of procalconin in liver transpant patients treated with anti-thymocyte globulin [J]. Crit Care, 2007, 11(6): 131-136.
[18]Kretzschmar M, Kruger A, Schirrmeister W. Procalcitonin following elective partial liver resection-origin from the liver? [J]. Acta Anaesthesiol Scand, 2001, 45(9): 1162-1167.
(2015-12-16 收稿2016-01-27 修回)
(责任编辑张亚丽)
Exploration on correlation between procalcitonin level in patients after liver transplantation operation and lung infection
TAN Qinghai and GU Ye. Department of Internal Respiratory, General Hospital of Chinese People’s Armed Police Forces, Beijing 100039, China
【Abstract】ObjectiveTo investigate the clinical diagnosis value of plasma procalcitonin(PCT) on lungs infection in patients after liver transplantation operation.MethodsLevel of plasma PCT in 165 patients who underwent liver transplantation were detected, then differences of PCT level were compared in patients with infection or not, and the relationship bewtween different etiology and PCT values were observed.ResultsLevel of plasma PCT in the post-operative infection group was significantly higher than that in the noninfection group(t=2.05,P=0.047). Among 165 patients with liver transplantation, the top three etiologies were liver cancer, liver cirrhosis and alcoholic cirrhosis. PCT level of infection group and non-infection group with the top three etiologies were compared: differences of PCT level in patients with liver cancer or alcoholic cirrhosis were not statistically significant between infection group and non-infection group; PCT level of the infection group in patients with cirrhosis after hepatitis was higher than that in the non-infection group (t=2.40, P=0.034). ConclusionsDetection of plasma PCT level is beneficial for early diagnosis of infection after liver transplantation. For patients with liver cancer and alcoholic cirrhosis, dynamically monitor of PCT combined with inflammatory biomarkers are needed.
【Keywords】liver transplantation;procalcitonin;infection
Corresponding author:GU Ye, E-mail: yezicookie@126.com
通讯作者:谷晔,E-mail: yezicookie@126.com
作者简介:谭青海,硕士研究生在读,E-mail: 983582874@qq.com
DOI:10.13919/j.issn.2095-6274.2016.02.008