代谢综合征与相应血常规指标的关联性研究
2016-05-30陶丽新刘相佟李海彬闫傲霜郭秀花
杨 昆 陶丽新 曹 凯 刘相佟 李海彬 闫傲霜 郭秀花*
(1.首都医科大学公共卫生学院流行病与卫生统计学系,北京100069; 2.北京市临床流行病学重点实验室,北京 100069;3.北京市科学技术委员会, 北京 100195)
代谢综合征与相应血常规指标的关联性研究
杨昆1,2陶丽新1,2曹凯1,2刘相佟1,2李海彬1,2闫傲霜3*郭秀花1,2*
(1.首都医科大学公共卫生学院流行病与卫生统计学系,北京100069; 2.北京市临床流行病学重点实验室,北京 100069;3.北京市科学技术委员会, 北京 100195)
【摘要】目的 探讨北京市成年人群代谢综合征(metabolic syndrome,MetS)的发生与血常规指标的关联性。方法选取来自北京3所医院的体检者作为研究对象,调查并追踪记录男女人群血常规指标及MetS各组分的检出情况,采用广义估计方程探讨代谢综合征的发生与血常规指标的关联性。结果2007至2012年间参加3次以上体检并符合研究要求的对象共7 489人,共有378人发生MetS。与MetS发生相关联的血常规指标,以最低的四分位数作参照,对男性而言,红细胞比容(hematocrit value, HCT)和白细胞计数(white blood cell, WBC) 的第四分位发生MetS的RR值分别为1.861 3(95%CI:1.325 6~2.613 5)和 2.598 4(95%CI:1.805 5~3.739 5);对女性而言,红细胞计数(red blood cell, RBC)、WBC和淋巴细胞的第四分位发生MetS的RR值分别为3.146 3(95%CI:1.836 3~5.391 0)、1.897 1(95%CI:1.089 9~3.302 2)和2.200 8(95%CI:1.221 9~3.964 0)。结论北京市成年人群体检中HCT、WBC、RBC和淋巴细胞等血常规指标与MetS的发生具有关联性,可作为MetS发生的预测指标。
【关键词】代谢综合征;血常规指标;广义估计方程;队列研究
代谢综合征(metabolic syndrome,MetS)是以糖代谢异常(糖尿病或糖调节受损)、高血压、血脂异常、中心性肥胖等多种主要疾病或危险因素在个体聚集为特征的一组临床症候群[1]。近年来,随着人们对MetS的深入研究,已经明确MetS的发生与遗传和环境因素有关,但是其具体的病因和发病机制目前尚不十分清楚[2]。国内外学者[3-5]发现非酒精性脂肪肝、慢性炎性反应以及血液凝集状态与MetS的发生密切相关。而影响血液凝集状态和代表机体炎性反应的红细胞计数(red blood cell, RBC)、红细胞比容(hematocrit value, HCT)、血红蛋白(hemoglobin, HGB)、血小板(blood platelet, PLT)等血常规指标都有可能成为预测和诊断MetS的新指标。因此本研究利用广义线性模型探讨MetS与相关的血常规指标的关联性,为MetS的早期诊断和预防提供理论支持。
1研究对象与方法
1.1研究对象
通过首都医科大学附属北京同仁医院、北京电力医院和北京小汤山医院体检中心,获得体检人群的电子数据。个人体检记录以病历号为唯一标识,将历年的数据信息合并、整理。以2007年作为基线,保留了至少参加过3次的体检者信息。调查对象均知情同意。在2007至2012年间,基线时参加体检者共计8 750人。排除有冠状动脉粥样硬化性心脏病(以下简称冠心病)、心绞痛、心肌梗死、脑卒中等严重合并症者474人,排除患有MetS及代谢组分异常者787人,最终符合要求的研究对象有7 489人,其中男性为3 389人(45.25%)。
1.2研究方法和内容
1.2.1调查内容
一般人口学特征、身高、体质量、血压。
血常规检查:受检者体检前日的晚12点后禁食,早晨空腹抽取静脉血,采用全自动血细胞分析仪检测血常规指标,包括:RBC、HCT、HGB、PLT、平均红细胞体积(mean corpuscular volume, MCV)、平均红细胞血红蛋白量(mean corpuscular hemoglobin, MCH)、平均红细胞血红蛋白浓度(mean corpuscular hemoglobin concentration, MCHC)、血小板分布宽度(platelet distribution width, PDW)、红细胞分布宽度(red blood cell volume distribution width, RDW)、白细胞计数(white blood cell, WBC)、平均血小板体积(mean platelet volume,MPV)、淋巴细胞和中性粒细胞。
血生化检查:受检者体检前日的晚12点后禁食,早晨空腹抽取静脉血,测定空腹血糖、三酰甘油(triglyceride,TG)和高密度脂蛋白胆固醇(high density lipoprotein cholesterol, HDL-C)。所有检查均使用统一试剂和方法,血糖检测采用葡萄糖氧化酶法测定,TG采用酶法测定,HDL-C采用直接法测定。由首都医科大学附属北京同仁医院、北京电力医院和北京小汤山医院检验中心完成。
1.2.2诊断标准
本次研究采用国际糖尿病联盟(International Diabetes Federation,IDF)和美国心脏协会(American Heart Association, AHA)/国立心肺和血液研究所(National Heart, Lung and Blood Institute, NHLBI)就MS的定义于2009年发表的新的联合声明[1]。
具体标准如下:(1)腹型肥胖:根据腰围诊断。不同国家地区和人种有各自特定的数值;(2)高TG血症:TG≥1.7 mmol/L,或已经进行针对此项血脂异常的治疗;(3)低HDL-C血症:男性<1.0 mm/L,女性<1.30 mm/L,或已经进行针对此项血脂异常的治疗;(4)血压升高:收缩压≥130 mmHg(1 mmHg=0.133 kPa)和(或)舒张压≥85 mmHg,或已经诊断高血压并开始治疗;(5)空腹血糖≥5.6 mmol/L,或已经诊断为2型糖尿病并开始治疗。
1.3统计学方法
本研究采用SPSS 21.0进行分析。采用Shapiro-Wilk 方法检验分组资料的正态性。计量资料采用Studentt检验或者秩和检验。按照四分位数间距,将指标测量值由低到高分为4类(Q1~Q4)。运用广义估计方程(generalized estimation equation,GEE)分析代谢综合征与血常规指标的关系。以P<0.05为差异有统计学意义。
2结果
2.1一般情况
研究对象在2007和2012年5个代谢组分的情况详见表1。除年龄外,不同性别各组分数值差异均具有统计学意义。
2.2 相关分析
利用单变量GEE筛选与MetS相关的指标,对于男性,除了MCV、MCH、MCHC和PDW外其他指标均有统计学意义。对于女性,除了RDW、MCH、MCHC、PDW外其他指标均有统计学意义,详见表2。将这些指标放入到多变量GEE模型中进行分析,探讨影响MetS发生的危险因素,详见图1。

表1 研究对象2007年和2012年代谢指标情况
△1 mmHg=0.133 kPa; BMI:body mass index; SBP:systolic blood pressure; DBP:diastolic blood pressure; FPG:fasting plasma glucose; TG:triglyceride; HDL-C:high density lipoprotein cholesterol.
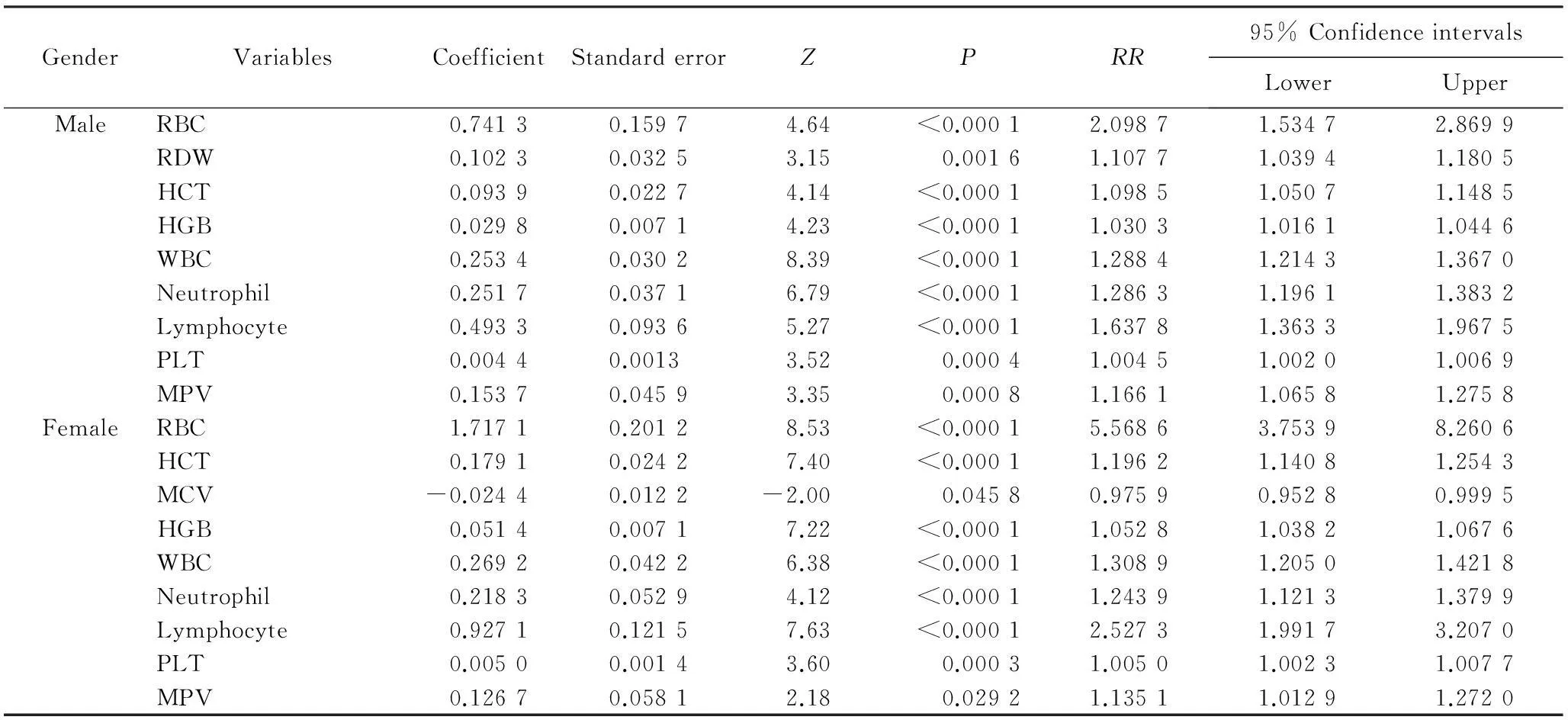
表2 单变量GEE筛选与MetS发生相关的血常规指标
GEE:generalized estimation equation;Mets:metabolic syndrome; RBC:red blood cell; RDW:red cell distribution width; HCT:hematocrit; HGB:hemoglobin; WBC:white blood cell; PLT:platelet; MPV:mean platelet volume; MCV:mean corpuscular volume.
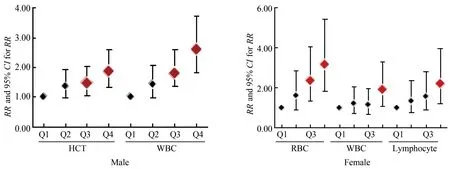
图1 多变量GEE筛选与影响MetS发生的血常规指标
◆P<0.05; GEE:generalized estimation equation;HCT:hematocrit value; WBC:white blood cell; RBC:red blood cell.
校正了其他指标后,对于男性组,得到影响MetS发生的血常规指标为HCT和WBC。与最低的HCT四分位数Q1相比,Q3的RR值以及95%CI为 1.458 8 (1.049 9,2.026 9),Q4的RR值以及95%CI为1.861 3(1.325 6~2.613 5)。与最低的WBC四分位数Q1相比,Q3的RR值以及95%CI为1.796 7(1.236 5~2.610 7),Q4的RR值以及95%CI为2.598 4 (1.805 5~3.739 5)。对于女性组,影响MetS发生的血常规指标为RBC、WBC和淋巴细胞。与RBC最低的四分位数Q1相比,Q3的RR值以及95%CI为2.338 0(1.357 3~4.027 3),Q4的RR值以及95%CI为3.146 3(1.836 3~5.391 0)。与WBC最低的四分位数Q1相比,Q4的RR值以及95%CI为1.897 1(1.089 9~3.302 2)。与淋巴细胞最低四分位数Q1相比,Q4的RR值以及95%CI为2.200 8(1.221 9~3.964 0)。
3讨论
近年来,随着人们对MetS的深入研究,发现代谢综合征不仅与糖尿病和心脑血管疾病[6]有关,而且与肝脏疾病[3]、慢性肾病[7]、血管纤维化等疾病有关。MetS的发生包括遗传和环境因素,其主要的发病机制可能与胰岛素抵抗、炎性反应和高黏血症[4-5,8]有关。
炎性反应可能是代谢综合征和动脉粥样硬化等心脑血管疾病的主要原因。有研究[4,9-10]发现代谢综合征与一系列慢性、低度炎性反应有关。以往研究[11]发现WBC与胰岛素抵抗以及高胰岛素血症有相关性,而胰岛素抵抗被认为是MetS发生的主要原因。一项2005~2010年美国的全国健康和营养调查发现WBC是肥胖的危险因素[12]。许多不同大型人群研究也发现总的白细胞数量以及不同的白细胞数量与MetS以及其各个组分具有相关性[13-14]。本研究发现WBC与男性、女性人群MetS发生均有关,与其他地区研究所得结论相符。WBC在临床实践中是常规检测项目,对疾病早筛查和诊疗更加实用。
一些横断面研究在印度人群[11]、以色列人群[15]、韩国人群[16]和日本人群[17]中发现RBC与MetS相关。但是本研究只是发现RBC数量与女性的血压升高相关,这可能与不同国家和地区和地区人群的特异性有关,有关不同国家和地区不同种族人群RBC数量与MetS及其组分的相关性可以做进一步研究。
HCT升高可能会增加血液黏度和血流外周阻力,并进一步促进胰岛素抵抗。有研究[4,11]证实HCT与胰岛素抵抗[11]和糖尿病[4]的发生有相关性,而胰岛素抵抗是代谢综合征的主要原因。一项泰国人群[18]和两项日本人群[19-20]中的横断面研究发现HCT与MetS具有相关性。本研究证实HCT指标与北京市成年男性人群MetS的发生有相关性。
淋巴细胞中T细胞、B细胞能够增加MetS发生的风险[21]。炎性反应状态下,T淋巴细胞被激活渗透血管壁后,可与浸润的脂肪细胞结合,具有免疫活性的淋巴细胞通过自身表面抗原与相应的受体进行特异性的结合,同时表达和分泌细胞因子,参与动脉粥样硬化的发生和发展,进而导致血管损伤。本研究证实女性MetS的发生与血液指标淋巴细胞具有相关性,表明淋巴细胞可以提供方便和有用的标记来做代谢综合征的进一步风险评估。
目前,医院体检主要测量血常规指标,影响血液凝集状态的RBC、HCT、HGB、PLT等血常规指标都有可能成为预测和诊断MetS的新指标。因此探讨与MetS相关的血液指标,不仅可以很好地预防一些慢性疾病的发生,为MetS的早期诊断和预防提供理论支持,对于有效地降低心脑血管疾病的发生率和病死率也具有重要意义。
4参考文献
[1] Alberti K, Eckel R H, Grundy S M, et al. Harmonizing the metabolic syndrome: a joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity[J]. Circulation, 2009, 120(16): 1640-1645.
[2] Ong G, Davis W A, Davis T M. Serum uric acid does not predict cardiovascular or all-cause mortality in type 2 diabetes: the Fremantle Diabetes Study[J]. Diabetologia,2010, 53(7):1288-1294.
[3] 张永媛. 基于队列设计纵向监测与概率图模型的非酒精性脂肪肝与代谢综合征双向因果推断研究[D].济南: 山东大学,2013.
[4] Fernández-Bergés D, Consuegra-Sánchez L, Peafiel J, et al. Metabolic and inflammatory profiles of biomarkers in obesity, metabolic syndrome, and diabetes in a mediterranean population. DARIOS Inflammatory Study[J]. Rev Esp Cardiol (Engl Ed), 2014, 67(8):624-631.
[5] Karbek B, Bozkurt N C, Topaloglu O, et al. Relationship of vaspin and apelin levels with insulin resistance and atherosclerosis in metabolic syndrome[J]. Minerva Endocrinol, 2014, 39(2): 99-105.
[6] Mottillo S, Filion K B, Genest J, et al. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis[J]. J Am Coll Cardiol, 2010, 56(14): 1113-1132.
[7] Singh A K, Kari J A. Metabolic syndrome and chronic kidney disease[J]. Current opinion in nephrology and hypertension, 2013, 22(2): 198-203.
[8] Lasselin J, Capuron L. Chronic low-grade inflammation in metabolic disorders: relevance for behavioral symptoms[J]. Neuroimmunomodulation, 2014, 21(2-3): 95-101.
[9] 段力园, 刘晨曦,赵静,等. 胰岛素抵抗状态下脂代谢和炎性反应相互关系研究进展[J]. 解放军医药杂志,2014,26(9):101-106.
[10] 李娟, 郭广亚,周莉.某社区居民代谢综合征影响因素分析[J]. 中国煤炭工业医学杂志,2014,17(12):2018-2020.
[11] Barazzoni R, Gortan Cappellari G G, Semolic A, et al. The association between hematological parameters and insulin resistance is modified by body mass index-results from the North-East Italy MoMa population study[J]. PLoS One, 2014, 9(7): e101590.
[12] Vuong J, Qiu Y, La M, et al. Reference intervals of complete blood count constituents are highly correlated to waist circumference: Should obese patients have their own “normal values?”[J]. Am J Hematol, 2014,89(7):671-677.
[13] Odagiri K, Uehara A, Mizuta I, et al. Longitudinal study on white blood cell count and the incidence of metabolic syndrome[J]. Intern Med,2011, 50(21):2491-2498.
[14] Babio N, Ibarrola-Jurado N, Bulló M, et al. White blood cell counts as risk markers of developing metabolic syndrome and its components in the PREDIMED study[J]. PLoS One, 2013, 8(3): e58354.
[15] Mardi T, Toker S, Melamed S, et al. Increased erythropoiesis and subclinical inflammation as part of the metabolic syndrome[J]. Diabetes Res Clin Pract,2005, 69(3):249-255.
[16] Kim J A, Choi Y S, Hong J I, et al. Association of metabolic syndrome with white blood cell subtype and red blood cells[J]. Endocr J,2006, 53(1):133-139.
[17] Kotani K, Sakane N, Kurozawa Y. Increased red blood cells in patients with metabolic syndrome[J]. Endocr J,2006, 53(5):711-712.
[18] Lohsoonthorn V, Jiamjarasrungsi W, Williams M A. Association of hematological parameters with clustered components of metabolic syndrome among professional and office workers in bangkok, thailand[J]. Diabetes & Metab Syndr, 2007, 1(3):143-149.
[19] Kawamoto R, Tabara Y, Kohara K, et al. Hematological parameters are associated with metabolic syndrome in Japanese community-dwelling persons[J]. Endocrine, 2013, 43(2):334-341.
[20] Sugimori H, Tomoda F, Koike T, et al. Blood rheology and platelet function in untreated early-stage essential hypertensives complicated with metabolic syndrome[J]. Int J Hyperten, 2012, 2012:109830.
[21] Phillips AC, Carroll D, Gale CR, et al. Lymphocyte sub-population cell counts are associated with the metabolic syndrome and its components in the Vietnam Experience Study. Atherosclerosis 2010, 213(1):294-298.
编辑陈瑞芳
Relationships between metabolic syndrome and its related blood indexes
Yang Kun1,2, Tao Lixin1,2, Cao Kai1,2, Liu Xiangtong1,2, Li Haibin1,2, Yan Aoshuang3*, Guo Xiuhua1,2*
(1.DepartmentofEpidemiologyandHealthStatistics,SchoolofPublicHealth,CapitalMedicalUniversity,Beijing100069,China;2.BeijingMunicipalKeyLaboratoryofClinicalEpidemiology,Beijing100069,China;3.BeijingMunicipalScienceandTechnologyCommission,Beijing100195,China)
【Abstract】ObjectiveTo evaluate the relationships between metabolic syndromes (MetS) and its related blood indexes in Beijing adults’ population.MethodsSubjects from Beijing three hospitals were enrolled and blood indexes record were tracked. The detection rates of MetS and its accompanying blood indexes were investigated. Generalized estimation equation model was used to estimate the relationships between MetS and its related blood indexes. Results7 489 subjects, who attended the health check-up from 2007 to 2012, were incorporated into the final analysis. During the 5 year follow-up, 378 cases of MetS were developed. The related blood routine indexes with MetS were hematocrit value (HCT) and white blood cell (WBC) for males. Compared with Q1, the lower quartile of HCT and WBC,the RRs of Q4 were 1.861 3 (95% CI: 1.325 6-2.613 5) and 2.598 4(95% CI: 1.805 5-3.739-5), respectively. Red blood cell (RBC), WBC and lymphocyte were corresponding factors for females. Compared with Q1, the lower quartile of RBC, WBC and lymphocyte,the RRs were 3.146 3 (95% CI: 1.836 3-5.391 0), 1.897 1 (95% CI: 1.089 9-3.302 2) and 2.200 8 (95% CI: 1.221 9-3.964 0), respectively.ConclusionMetS has a certain association with its related blood routine parameters, such as HCT, WBC, RBC and Lymphocyte applied by health check-up data in Beijing adults, and such parameters may be used as the predictors of MetS.
【Key words】metabolic syndrome; blood routine parameters; generalized estimation equation; longitudinal cohort study
(收稿日期:2015-10-21)
【中图分类号】R 589
[doi:10.3969/j.issn.1006-7795.2016.02.018]
*Corresponding author, E-mail:guoxiuh@ccmu.edu.cn
基金项目:国家自然科学基金(81373099,81001281,81530087,81502886),北京市自然科学基金(7131002),北京市优秀人才青年骨干个人项目(2014000020124G150)。This study was supported by National Natural Science Foundation of China (81373099,81001281,81530087,81502886), Natural Science Foundation of Beijing (7131002), Young Core Personal Project & Beijing Outstanding Talent Training Project (2014000020124G150).
网络出版时间:2016-04-1221∶03网络出版地址:http://www.cnki.net/kcms/detail/11.3662.r.20160412.2103.010.html
· 基础研究 ·
