影响正畸用微螺钉种植体成功率的风险因素分析
2017-08-07郭建斌邹耿森郑辉蒋剑晖黄文秀
郭建斌, 邹耿森, 郑辉, 蒋剑晖, 黄文秀, 吴 东, 陈 江
影响正畸用微螺钉种植体成功率的风险因素分析
郭建斌, 邹耿森, 郑辉, 蒋剑晖, 黄文秀, 吴 东, 陈 江
目的 探讨并分析影响微螺钉种植体成功率的风险因素。 方法 选择固定矫治患者167例,总计植入微螺钉种植体360颗。应用Logistic回归分析对15个临床变量(性别、年龄、垂直骨面型、矢状骨面型、口腔卫生、上下颌骨、左右侧、区域、附着龈宽度、品牌、长度、直径、医生、植入和加载方式)进行回归分析。 结果 360颗微螺钉种植体有34颗发生松脱失败,成功率90.56%。成功率与患者的年龄、口腔卫生、垂直骨面型、植入部位(上下颌骨)、左右侧和附着龈宽度有相关性(P<0.05),与患者的性别、矢状骨面型、唇腭侧位置、医生、植入方式、加载方式、品牌、直径和长度无相关性。 结论 为了获得更高的微螺钉种植体成功率,医生应对患者加强口腔卫生宣教,并针对不同的风险因素采取相应的措施予以规避。
骨螺丝; 牙; 牙种植体; 正畸支抗; 正畸学,矫正; 因素分析,统计学
支抗在口腔正畸治疗中有重要的意义。骨性正畸支抗一直是医生关注的热点,目前包括修复种植体、腭部种植体、颧骨结扎、微型钛板、微螺钉种植体等,其中微螺钉种植体应用最普遍。它具有操作简单、体积小、异物感低、不依赖患者配合、应用灵活、矫治时间短等优点,受到了广泛认可。然而在临床应用中,微螺钉种植体会出现松动、松脱的现象,进而影响治疗效果。尽管有学者对影响微螺钉种植体的风险因素,诸如性别、年龄、骨面型、植入位点、长度、直径、植入方式、加载方式和强度、角度、临床用途等做了荟萃分析[1-2],但因微螺钉种植体品牌、规格及研究方法不同,各风险因素不易控制,对照不严格,尚未得出一致的结论,部分风险因素仍需要更多的证据来支持。例如,成功率的报道不一,从59.4%到100%不等[3];而Reint等回顾了70个风险因素,每个风险因素均存在不一致的结论,尤以种植位点和种植体相关因素较为混乱[4]。为此,本研究选用了15个临床医生关心且易于控制、容易对照的临床变量,应用Logistic回归分析进行分析,报告如下。
1 对象与方法
1.1 对象 选择2013年2月—2016年6月就诊的采用微螺钉种植体矫治的错牙合畸形患者167例,男性71例,女性96例,年龄(17.56±9.39)岁(8~27岁);共有微螺钉种植体360颗,男性142颗,女性218颗。纳入标准:采用固定矫治方案的错牙合畸形患者,无正畸、正颌治疗史,排除吸烟、牙周炎及影响骨代谢的全身系统性疾病,如糖尿病。
1.2 方法
1.2.1 临床变量的选择 将可能影响微螺钉种植体的15个临床变量分为4组:(1)患者相关,包括性别(男;女)、年龄(<12岁;12~18岁;>18岁)、垂直骨面型(低角;均角;高角)、矢状骨面型(Ⅰ类;Ⅱ类;Ⅲ类);(2)植入位点相关,包括口腔卫生(良好;一般;差)、颌骨(上颌;下颌)、左右侧、区域(唇颊侧;腭侧;舌侧)、附着龈宽度(≤4 mm;>4 mm);(3)微螺钉种植体相关,包括品牌(A;B)、长度(8 mm;10 mm;12 mm)、直径(1.4~1.5 mm;1.8~2.0 mm);(4)临床操作相关,包括医生(1;2)、植入方式(自攻;助攻)、加载方式(即刻;>2周)。微螺钉种植体成功标准如下:(1)局部无肿胀;(2)无松动度或松动度≤0.5 mm,能承载加力;(3)在治疗过程中能完成支抗任务[5]。口腔卫生评定参照正畸菌斑指数(ortho-plaque index, OPI)[6]。
1.2.2 临床操作 微螺钉种植体的植入分别由2名医生完成,其中1名具有>20年的口腔颌面外科经验,完成236颗;另1名具有>10年的口腔颌面外科经验,完成124颗。术前拍摄全景片明确植入部位解剖情况。阿替卡因局部浸润麻醉后,自攻组使用手柄直接植入;助攻组在生理盐水冷却下,用先锋钻穿通皮质骨后,再用手柄将微螺钉种植体植入。植入后微螺钉种植体稳定且冠部暴露于口腔而未被软组织覆盖。
1.2.3 微螺钉种植体 共2个系统:Bio-Ray系统(台湾亚太医疗公司),直径分别为1.5和2.0 mm,长度分别为8,10和12 mm;OSSTEM系统(韩国奥齿泰公司),直径分别为1.4和1.8 mm,长度分别为8和10 mm。
1.3 统计学处理 将所有原始数据录入计算机建立数据库,采用SPSS 19.0软件进行Logistic回归分析,以P<0.05为差别有统计学意义。
2 结 果
360颗微螺钉种植体中,发生松脱失败34颗,余326颗(90.56%)成功。成功率与患者年龄、口腔卫生、垂直骨面型、上下颌骨、左右侧和附着龈宽度相关(P<0.05,表1)。年龄更大的患者成功率更高(P=0.03);高角患者的成功率低于均角和低角患者(P=0.02);口腔卫生状况良好的患者成功率显著高于卫生差的患者(P<0.01);上颌骨的成功率显著高于下颌骨(P<0.01);左侧成功率显著高于右侧(P=0.04);附着龈宽度>4 mm的患者成功率显著高于≤4 mm的患者(P=0.03)。其他9个变量与微螺钉种植体成功率不相关。
3 讨 论
本研究将影响微螺钉种植体成功率的风险因素分为4组:患者相关、植入位点相关、微螺钉种植体相关和临床操作相关,结果显示,总体成功率与国内外相关研究基本一致[7-9]。年龄、垂直骨面型、口腔卫生、位点(上下颌骨及左右侧)和附着龈宽度是影响微螺钉种植体成功率的可能风险因素,而性别、矢状骨面型、唇腭侧位置、医生、植入方式、加载方式、品牌、直径和长度与微螺钉种植体成功率无关。
年龄和微螺钉种植体的成功率之间存在着明显的相关性,<12岁的患者失败的风险大为增加,这一现象可能与青少年患者尚缺乏足够成熟的骨质及骨量有关,尤其是其皮质骨厚度远低于成年人[10-11]。高角面型是影响微螺钉种植体成功率的高风险因素,与Miyawaki的研究一致[12]。原因可能是高角患者的骨密度和皮质骨厚度较低,初期稳定性和后期骨结合均被减弱,导致微螺钉种植体的成功率下降[13]。
菌斑及微生物是牙周炎及种植体周围炎发生的始动因素。口腔卫生差的患者,口中存在的菌斑及食物残渣等在微螺钉种植体周围堆积,细菌繁殖生长,使微螺钉种植体颈部周围的软硬组织发生炎症,导致种植体的松动、脱落[14]。此外,右侧具有更高的失败率也可能与口腔卫生相关。因为大多数人是右利手,右侧口腔卫生的护理相对不易[15]。由于种植体周围炎发生隐匿,进展快,预后不佳,提示临床医生在植入种植体后要加强术后护理和口腔卫生宣教,避免微螺钉种植体周围炎症的发生[16]。
表1 微螺钉种植体的成功率及Logistic回归分析结果
Tab 1 Success rate and statistical analysis for miniscrew implants
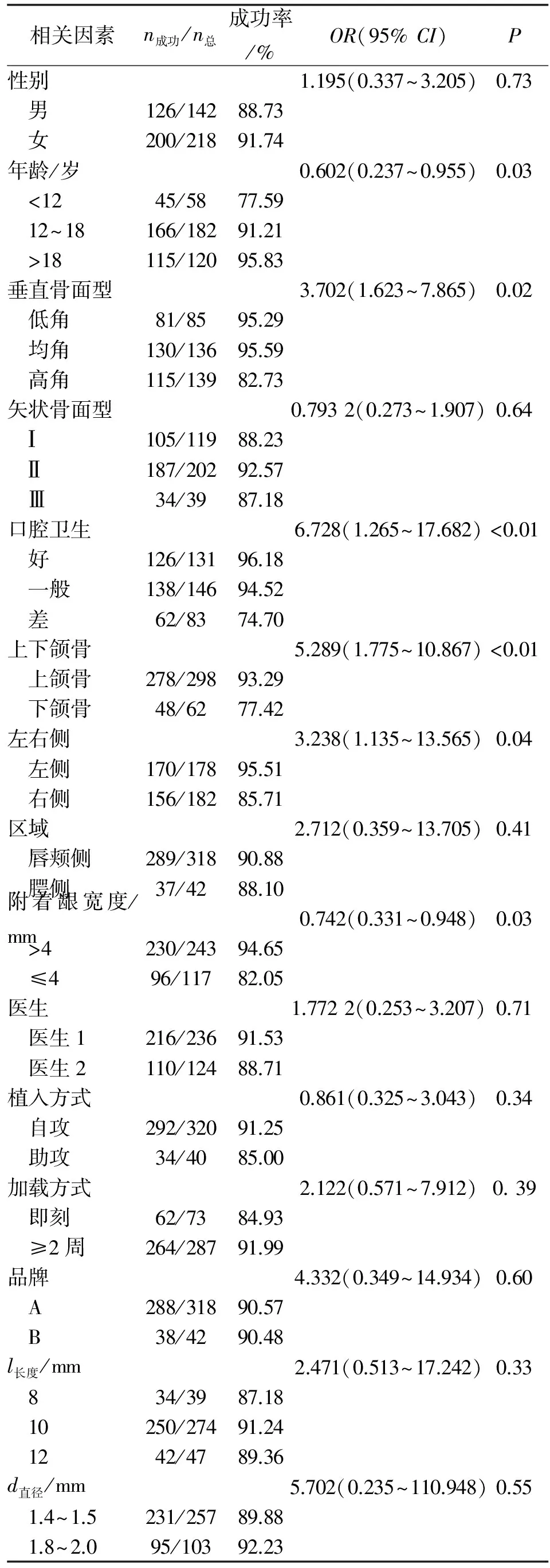
相关因素n成功/n总成功率/%OR(95%CI)P性别1.195(0.337~3.205)0.73 男126/14288.73 女200/21891.74年龄/岁0.602(0.237~0.955)0.03 <1245/5877.59 12~18166/18291.21 >18115/12095.83垂直骨面型3.702(1.623~7.865)0.02 低角81/8595.29 均角130/13695.59 高角115/13982.73矢状骨面型0.7932(0.273~1.907)0.64 Ⅰ105/11988.23 Ⅱ187/20292.57 Ⅲ34/3987.18口腔卫生6.728(1.265~17.682)<0.01 好126/13196.18 一般138/14694.52 差62/8374.70上下颌骨5.289(1.775~10.867)<0.01 上颌骨278/29893.29 下颌骨48/6277.42左右侧3.238(1.135~13.565)0.04 左侧170/17895.51 右侧156/18285.71区域2.712(0.359~13.705)0.41 唇颊侧289/31890.88 腭侧37/4288.10附着龈宽度/mm0.742(0.331~0.948)0.03 >4230/24394.65 ≤496/11782.05医生1.7722(0.253~3.207)0.71 医生1216/23691.53 医生2110/12488.71植入方式0.861(0.325~3.043)0.34 自攻292/32091.25 助攻34/4085.00加载方式2.122(0.571~7.912)0.39 即刻62/7384.93 ≥2周264/28791.99品牌4.332(0.349~14.934)0.60 A288/31890.57 B38/4290.48l长度/mm2.471(0.513~17.242)0.33 834/3987.18 10250/27491.24 1242/4789.36d直径/mm5.702(0.235~110.948)0.55 1.4~1.5231/25789.88 1.8~2.095/10392.23
下颌骨相对于上颌骨而言具有较厚的皮质骨厚度及更高的骨密度,从理论上讲,下颌应有更高的成功率,文献[17]也证实了这一点。但近年来,不少学者提出了不同观点,如Chen等认为,上下颌骨间成功率无显著性差异[18-19];本研究则显示,上颌骨的成功率高于下颌骨,与Hong的研究一致[20]。下颌骨失败率更高的原因可能有:(1)下颌骨皮质骨较厚,植入时多需要先锋钻预备,存在冷却不充分和骨灼伤的可能;(2)下颌骨的血运和营养供给不如上颌骨,随着愈合时间的延长,在上颌骨植入的微螺钉种植体可能会有更好的骨结合,从而获得更好的后期稳定性;(3)下颌骨的骨密度高可能会造成更高的植入扭矩,带来更多的骨微损伤,造成松脱;(4)下颌骨的附着龈宽度远低于上颌骨,下前庭沟浅,植入位点多位于牙槽黏膜附近,而牙槽黏膜不易抵抗外界刺激;(5)下颌的微螺钉种植体在咀嚼时容易受到食物冲击的影响[20-22]。
附着龈的存在对维持牙周健康有重要意义,且有利于菌斑控制。研究表明,微螺钉种植体的成功率与附着龈宽度相关,与口腔种植体的研究一致[23]。当微种植体支抗植入位点处于膜龈联合部时,游离的牙槽黏膜易包绕微螺钉种植体的头部,口腔卫生措施不易到位,菌斑堆积,导致种植体黏膜炎及周围炎,导致微种植体支抗的松脱。
种植体长度对成功率的影响有着不同的观点。一般而言,长的种植体容易获得更好的成功率,Yi和Chen等的研究也支持这一观点,8 mm的成功率(90.2%)显著高于6 mm(72.2%)[18, 24]。Kuroda等的研究则表明,种植体长度与成功率不相关[21]。不同研究的结论不同,可能与所用的微螺钉种植体的长度范围及植入部位的差异有关。Gracco等认为,微螺钉种植体的最佳长度为9 mm,此时其应力值分布最小,对颌骨解剖结构的损伤最小[25]。此外,不同的植入部位有着不同的皮质骨厚度,一定程度上影响了成功率[26]。临床上应根据不同的植入部位的解剖条件(皮质骨厚度,黏膜厚度,邻近牙根或上颌窦的位置)和植入角度选择合适的长度。
直径对微螺钉种植体的成功率没有影响。Miyawaki等发现,1.0 mm直径的微螺钉种植体的成功率显著低于1.5和2.3 mm[12]。究其原因,可能是1.0 mm的直径容易对骨组织产生较大的应力性损害,建议微螺钉种植体的直径应>1.3 mm[27-28]。由于本研究所采用的微螺钉种植体直径均>1.3 mm,故未发现直径对成功率的影响。
随着微螺钉种植体的应用及基础研究的不断深入,相关的正畸技术将会日益完善成熟。在临床实践过程中,为了获得更高的成功率,医生要注意对患者加强口腔卫生宣教和监督,植入位点尽可能位于附着龈区域,选用合适的尺寸,在下颌骨或其他皮质骨相对较厚的区域应使用先锋钻预备,避免骨灼伤。
[1] Papadopoulos M A, Papageorgiou S N, Zogakis I P. Clinical effectiveness of orthodontic miniscrew implants: a meta-analysis[J].JDentRes, 2011,90(8):969-976.
[2] Papageorgiou S N, Zogakis I P, Papadopoulos M A. Failure rates and associated risk factors of orthodontic miniscrew implants: a meta-analysis[J].AmJOrthodDentofacialOrthop, 2012,142(5):577-595.
[3] Crismani A G, Bertl M H, Celar A G,etal. Miniscrews in orthodontic treatment: review and analysis of published clinical trials[J].AmJOrthodDentofacialOrthop, 2010, 137(1): 108-113.
[4] Reynders R, Ronchi L, Bipat S. Mini-implants in orthodontics: a systematic review of the literature[J].AmJOrthodDentofacialOrthop, 2009,135(5):564-565.
[5] Cheng S J, Tseng I Y, Lee J J,etal. A prospective study of the risk factors associated with failure of mini-implants used for orthodontic anchorage[J].IntJOralMaxillofacImplants, 2004,19(1):100-106.
[6] Atassi F, Awartani F. Oral hygiene status among orthodontic patients[J].JContempDentPract, 2010,11(4):25-32.
[7] Lim H J, Choi Y J, Evans C A,etal. Predictors of initial stability of orthodontic miniscrew implants[J].EurJOrthod, 2011,33(5):528-532.
[8] Wu T Y, Kuang S H, Wu C H. Factors associated with the stability of mini-implants for orthodontic anchorage: a study of 414 samples in Taiwan[J].JOralMaxillofacSurg, 2009,67(8):1595-1599.
[9] 曹小青, 张 莉, 刘龙坤. 正畸用微种植钉种植成功的多因素分析[J]. 口腔医学研究, 2016,32(1):79-82.
[10] Stagi S, Cavalli L, Iurato C,etal. Bone metabolism in children and adolescents: main characteristics of the determinants of peak bone mass[J].ClinCasesMinerBoneMetab, 2013,10(3):172-179.
[11] Wang Z, Zhao Z, Xue J,etal. Pullout strength of miniscrews placed in anterior mandibles of adult and adolescent dogs: a microcomputed tomographic analysis[J].AmJOrthodDentofacialOrthop, 2010,137(1):100-107.
[12] Miyawaki S, Koyama I, Inoue M,etal. Factors associated with the stability of titanium screws placed in the posterior region for orthodontic anchorage[J].AmJOrthodDentofacialOrthop, 2003,124(4):373-378.
[13] Baek S H, Kim B M, Kyung S H,etal. Success rate and risk factors associated with mini-implants reinstalled in the maxilla[J].AngleOrthod, 2008,78(5):895-901.
[14] Antoszewska J, Raftowicz-Wojcik K, Kawala B,etal. Biological factors involved in implant-anchored orthodontics and in prosthetic-implant therapy: a literature review[J].ArchImmunolTherExp(Warsz), 2010,58(5):379-383.
[15] Park H S, Jeong S H, Kwon O W. Factors affecting the clinical success of screw implants used as orthodontic anchorage [J].AmJOrthodDentofacialOrthop, 2006,130(1):18-25.
[16] Jepsen S, Berglundh T, Genco R,etal. Primary prevention of peri-implantitis: managing peri-implant mucositis[J].JClinPeriodontol, 2015,42(Suppl 16):152-157.
[17] Chen Y J, Chang H H, Huang C Y,etal. A retrospective analysis of the failure rate of three different orthodontic skeletal anchorage systems[J].ClinOralImplantsRes, 2007,18(6):768-775.
[18] Yi L S, Mimi Y, Ming T C,etal. A study of success rate of miniscrew implants as temporary anchorage devices in singapore[J].IntJDent, 2015,2015:294-290.
[19] Chen Y J, Chang H H, Lin H. Y,etal. Stability of miniplates and miniscrews used for orthodontic anchorage: experience with 492 temporary anchorage devices[J].ClinOralImplantsRes, 2008,19(11):1188-1196.
[20] Hong S B, Kusnoto B, Kim E J,etal. Prognostic factors associated with the success rates of posterior orthodontic miniscrew implants: A subgroup meta-analysis[J].KoreanJOrthod, 2016,46(2):111-126.
[21] Kuroda S, Sugawara Y, Deguchi T,etal. Clinical use of miniscrew implants as orthodontic anchorage: success rates and postoperative discomfort[J].AmJOrthodDentofacialOrthop, 2007,131(1):9-15.
[22] Motoyoshi M, Hirabayashi M, Uemura M,etal. Recommended placement torque when tightening an orthodontic mini-implant[J].ClinOralImplantsRes, 2006,17(1):109-114.
[23] Bassetti M, Kaufmann R, Salvi G E,etal. Soft tissue grafting to improve the attached mucosa at dental implants: A review of the literature and proposal of a decision tree[J].QuintessenceInt, 2015,46(6):499-510.
[24] Chen C H, Chang C S, Hsieh C H,etal, The use of microimplants in orthodontic anchorage[J].JOralMaxillofacSurg, 2006,64(8):1209-1213.
[25] Gracco A, Cirignaco A, Cozzani M,etal. Numerical/experimental analysis of the stress field around miniscrews for orthodontic anchorage[J].EurJOrthod, 2009,31(1):12-20.
[26] Sawada K, Nakahara K, Matsunaga S,etal. Evaluation of cortical bone thickness and root proximity at maxillary interradicular sites for mini-implant placement[J].ClinOralImplantsRes, 2013,24(Suppl A100):1-7.
[27] Sivamurthy G, S Sundari. Stress distribution patterns at mini-implant site during retraction and intrusion-a three-dimensional finite element study[J].ProgOrthod, 2016,17(1):1-4.
[28] 鲁颖娟, 常少海, 伍 虹, 等. 不同力作用下微种植体长度和直径的双变量优化分析[J]. 华西口腔医学杂志, 2014,32(1):85-90.
(编辑:何佳凤)
Risk Factors Associated with the Success Rates of Orthodontic Miniscrew Implants
GUO Jianbin, ZOU Gengsen, ZHENG Hui, JIANG Jianhui, HUANG Wenxiu, WU Dong, CHEN Jiang
Department of Implantology, School and Hospital of Stomatology,Fujian Medical University, Fuzhou 350002, China
Objective To investigate and analyze the risk factors associated with the success rate of miniscrew implants. Methods 167 patients(71 male patients and 96 female patients, the average age was 17.56±9.39) with a total of 360 miniscrew implants were involved in this study, and 15 clinical variables(gender, age, vertical/sagittal skeletal facial pattern, oral hygiene, the implant site, left and right side, location, and attached gingiva, brands, length, diameter, surgeons, drilling/loading patterns) were investigated by logistic regression analysis. Results 34 miniscrew implants failed and the success rate was 90.56%. The success rate was correlated with age, oral hygiene, vertical skeletal facial pattern, the implant site (upper and lower jaw), left and right side, and attached gingiva width (P<0.05). No evidence was found in this study that gender, sagittal skeletal facial pattern, buccal/lingual sites, surgeons, drilling/loading patterns, brands, length or diameter was associated with the success rate. Conclusion To minimize failure, clinicians should strengthen the oral hygiene instruction and take appropriate measures for different risk factors.
bone screws; tooth; dental implants; orthodontic anchorage procedures; orthodontics, corrective; factor analysis, statistical
2016-10-06
福建省自然科学基金(2013J05112);福建省重点专科资助项目(20121589);福建省大学生创新创业训练计划(201510392105)
福建医科大学 附属口腔医院种植科,福州 350002
郭建斌,男,主治医师,医学博士
陈 江. Email: dentistjiang@sina.com
R687.32; R783.5
A
1672-4194(2017)02-0126-04