非布司他与别嘌醇在降尿酸治疗中的有效性和安全性对比研究
2016-06-21吴晓丹四川省医学科学院四川省人民医院风湿免疫科四川成都610072
周 乔,苏 江,吴晓丹,周 彬(四川省医学科学院·四川省人民医院风湿免疫科,四川 成都 610072)
非布司他与别嘌醇在降尿酸治疗中的有效性和安全性对比研究
周 乔,苏 江,吴晓丹,周 彬
(四川省医学科学院·四川省人民医院风湿免疫科,四川 成都 610072)
目的 对比非布司他与别嘌醇在痛风治疗中降尿酸的有效性和安全性。方法 2011年11月至2014年12月我院风湿免疫科就诊的90例痛风患者,分为非布司他40 mg组,非布司他80 mg组和别嘌醇组各30例,比较降尿酸的效果和不良事件发生情况。结果 各组患者的尿酸水平在治疗1月后与基线比较均明显降低(P< 0.05),非布司他80 mg组与别嘌醇组比较,尿酸水平在第1、2、3、6月明显降低;与非布司他40 mg组比较,尿酸水平在第1、5、6月明显降低(P< 0.05)。非布司他40 mg组与别嘌醇组比较,各时点尿酸水平差异均无统计学意义(P> 0.05)。两非布司他组的肝功损害、高脂血症和痛风发作的发生率高于别嘌醇组(P< 0.05)。结论 在各器官功能正常的患者中,非布司他治疗有效性和安全性更易被接受。
痛风;非布司他;别嘌醇;降尿酸治疗
近年由于促尿酸升高的一些合并症的增加[1]和生活方式改变等[2],痛风的患病率日益增长。高尿酸血症是指血清尿酸水平大于6.8或7.0 mg/dl[3,4]。组织内单尿酸钠晶体沉积是痛风发作和形成痛风石的主要原因,因此降尿酸治疗(ULT)在痛风患者的管理中尤为重要。目前的降尿酸药物主要有抑制尿酸生成剂和促尿酸排泄剂。抑制尿酸生成剂主要为黄嘌呤氧化酶抑制剂,包括别嘌醇和非布司他。前者在携带HLA-B * 5801等位基因的人群中可能导致严重的超敏反应,如剥脱性皮炎等,在中国汉族和泰国人群中由于携带该基因的人群占比较高(约8%),故其不良事件风险相对高于欧美人群[5]。非布司他是一种新的黄嘌呤氧化酶抑制剂,于2013年获得授权在我国使用,目前制剂为40 mg片剂。为了比较这两种药物的疗效和安全性,我们收集了2011年11月至2014年12月的痛风患者的临床和实验室数据,现报道如下。
1 资料与方法
1.1 一般资料 2011年11月至2014年12月在我院进行降尿酸治疗的90例患者。纳入标准:年龄18~70岁;诊断符合1985年Holmes标准[6];血尿酸≥8.0 mg/dl (476 μmol/L);体重指数≤30 kg/m2;有至少6个月的随访数据。排除标准:继发性高尿酸血症(如肾脏、血液系统疾病);血肌酐≥133 μmol/L;转氨酶(ALT或AST)>2倍正常上限;白细胞<4.0×109/L或血红蛋白<100 g/L或血小板<100×109/L;停用降尿酸药物不到1周;合用糖皮质激素、免疫抑制剂、他汀类、噻嗪类利尿剂、氯沙坦、茶碱类药物;慢性结缔组织病,有重度、进展性和/或未控制的肾脏、肝脏、血液系统、消化道、内分泌、肺部、心脏、神经系统等疾病或肿瘤;有酗酒或药物滥用史;有慢性感染、近期严重或危及生命的感染病史。90例患者分为非布司他40 mg组,非布司他80 mg组和别嘌醇组各30例,三组基线资料比较差异均无统计学意义(P> 0.05),见表1。

表1 三组基线资料比较
1.2 方法 在患者开始降尿酸及每个月随访时检测血常规、血生化指标。如果治疗中出现急性痛风发作可使用非甾体类抗炎药(NSAIDs)或秋水仙碱。
1.3 统计学方法 采用SPSS 22.0统计学软件进行数据分析。计量资料以均数±标准差表示,组间比较采用重复测量数据的方差分析及LDS-t检验;计数资料比较采用卡方检验。P< 0.05为差异有统计学意义。
2 结果
2.1 降尿酸疗效 各组患者的尿酸水平在治疗1月后与基线比较均明显降低(P< 0.05),并在后续治疗中维持于该水平。非布司他80 mg组与别嘌醇组比较,尿酸水平在第1、2、3、6月明显降低;与非布司他40 mg组比较,尿酸水平在第1、5、6月明显降低(P< 0.05)。非布司他40 mg组与别嘌醇组比较,各时点尿酸水平差异均无统计学意义(P> 0.05)。见表2。
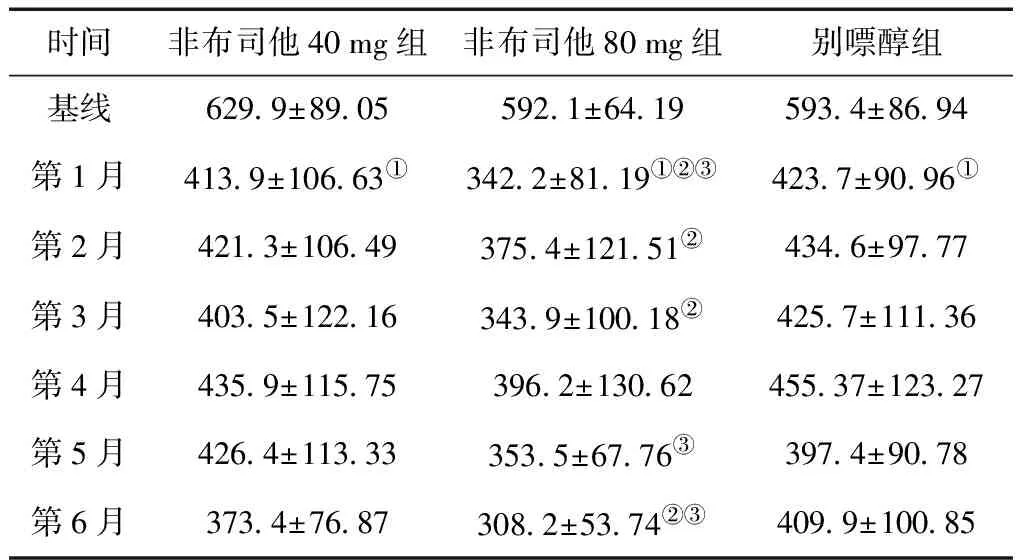
表2 各组患者治疗随访期间的血尿酸值 (μmol/L)
①与基线比较,P< 0.05;②与别嘌醇组比较,P< 0.05;③与非布司他40 mg组比较,P< 0.05
2.2 不良事件 共40例患者出现了88例次不良事件。其中,非布司他40 mg组26例次,非布司他80 mg 组37例次,别嘌醇组25例次。常见不良事件为痛风发作(26例次)、肝功异常(22例次)和高脂血症(11例次)。痛风发作患者使用NSAIDs或秋水仙碱缓解疼痛,大多数患者可继续进行降尿酸治疗,仅2例因重度疼痛中止治疗。三组间发生率比较,差异无统计学意义(P> 0.05)。将非布司他40 mg组与80 mg组作为整体的肝功损害发病率与别嘌醇组比较,差异有统计学意义(P= 0.046),但两非布司他组之间差异无统计学意义。两非布司他组中共有5例因中到重度肝功损害且经2周治疗仍未恢复,从而中断原有的降尿酸治疗,但在保肝治疗后均已恢复,并在后续选择了其它降尿酸方案。非布司他40 mg 组和80 mg 组的高脂血症发生率与别嘌醇组比较,差异均有统计学意义(P< 0.05)。别嘌醇组过敏的发生率最高,与其它两组比较,差异均有统计学意义(P< 0.05)。见表4。

表4 三组不良事件及停药原因 [n(%)]
3 讨论
痛风是最常见的炎性关节炎疾病之一,尽管治疗容易,但仍有大量患者未得到恰当的治疗。欧洲抗风湿病联盟(EULAR)和ACR推荐降尿酸的目标值为低于6.0 mg/dL(360 μmol/L)[7,8]。本研究中,仅非布司他80 mg组患者在第1月末的血尿酸值达到了该水平,并维持了半年。我们认为非布司他80 mg qd的降尿酸效果优于别嘌醇。而与非布司他40 mg组比较,降尿酸效果较难评价,需要更进一步的大样本和多中心前瞻性研究来进行评判。
不良事件方面,非布司他组更易出现肝功损害和高脂血症。我们推测肝功损害可能存在剂量依赖性,但需要更进一步研究明确。而皮疹等过敏事件则更多见于别嘌醇组。痛风发作是降尿酸治疗中不可避免的不良事件,其原因主要是由于体内尿酸晶体的快速溶解,尤其是在治疗初期。指南推荐所有患者在降尿酸治疗初期可采用秋水仙碱或低剂量NSAIDs对此进行预防[9~13]。本研究中,使用降尿酸治疗的患者大多在前两周出现痛风的发作。
本研究不足之处是我们仅纳入了肝肾功能正常、无显著合并症(如高血压、糖尿病、其它风湿病)以及无其它伴随用药的患者。这类患者根据临床有效性和安全性评估,我们推荐使用非布司他40 mg qd降尿酸。然而,患者病情有复杂之处,具体使用方案还需进行个体化评估,并规律监测相关指标。
[1] Brook RA,Forsythe A,Smeeding JE,et al.Chronic gout:epidemiology,disease progression,treatment and disease burden[J].Curr Med Res Opin,2010,26:2813-2821.
[2] Doherty M.New insights into the epidemiology of gout[J].Rheumatology (Oxford),2009,48(Suppl 2):2-8.
[3] Baker JF,Schumacher HR.Update on gout and hyperuricemia[J].Int J Clin Pract,2010,64:371-377.
[4] Neogi T.Clinical Practice:Gout[J].N Engl J Med,2011,364:443-452.
[5] Lonjou C,Borot N,Sekula P,et al.A European study of HLA-B in Stevens-Johnson syndrome and toxic epidermal necrolysis related to five high-risk drugs[J].Pharmacogenet Genomics,2008,18:99-107.
[6] German DC,Holmes EW.Hyperuricemia and gout[J].Med Clin North Am,1986,70:419-436.
[7] Hamburger M,Baraf HS,Adamson TC,et al.2011 recommendations for the diagnosis and management of gout and hyperuricemia[J].Phys Sportsmed,2011,39:98-123.
[8] Khanna D,Fitzgerald JD,Khanna PP,et al.2012 American College of Rheumatology guidelines for management of gout.Part 1:systematic non-pharmacologic and pharmacologic therapeutic approaches to hyperuricemia[J].Arthritis Care & Research,2012,64:1431-1446.
[9] Becker MA,Schumacher HR,Wortmann RL,et al. Febuxostat compared with allopurinol in patients with hyperuricemia and gout[J].N Engl J Med,2005,353:2450-2461.
[10]Sundy JS,Baraf HS,Yood RA,et al.Efficacy and tolerability of pegloticase for the treatment of chronic gout in patients refractory to conventional treatment:two randomized controlled trials[J].JAMA,2011,306:711-720.
[11] Becker MA,Schumacher HR,Espinoza LR,et al.The urate-lowering efficacy and safety of febuxostat in the treatment of the hyperuricemia of gout:the CONFIRMS trial[J].Arthritis Res Ther,2010,12:R63.
[12] Wortmann RL,Macdonald PA,Hunt B,et al.Effect of prophylaxis on gout flares after the initiation of urate lowering therapy:analysis of data from three phase III trials[J].Clin Ther,2010,32:2386-2397.
[13] Khanna D,Khanna PP,Fitzgerald JD,et al.2012 American College of Rheumatology guidelines for management of gout.Part 2:therapy and antiinflammatory prophylaxis of acute gouty arthritis[J].Arthritis Care & Research,2012,64:1447-1461.
Comparison of clinical effect and safety between febuxostat and allopurinol in reducing uric acid treatment
ZHOUQiao,SUJiang,WUXiao-dan,ZHOUBin
(DepartmentofRheumatology,SichuanAcademyofMedicalScience&SichuanProvincialPeople’sHospital,Chengdu610072,China)
Objective To evaluate and compare the efficacy and safety of two xanthine oxidase inhibitor:febuxostat and allopurinol in Chinese gout patients.Methods Ninety gout patients treated in our department form November 2011 to December 2014 were selected and divided into three groups:febuxostat 40 mg qd,febuxostat 80 mg qd and allopurinol 0.1 g tid,30 patients in each group. The effect of reducing uric acid and adverse events were compared.Results The levels of serum UA in all three groups were reduced when compared to basic line after one month of treatment (P< 0.05). In the febuxostat 80 mg qd group,serum uric acid levels were significantly decreased in the 1 st,2 nd,3rd and 6th month and in 1st,5th and 6th month after treatment when compared to the allopurinol group and the febuxostat 40 mg qd group,respectively (P< 0.05). There was no significant difference in serum uric acid between febuxostat 40 mg qd group and allopurinol group at different time points (P> 0.05). However,the incidence of abnormal liver function,hyperlipidemia and gout flare was also higher in febuxostat groups when compared to the allopurinol group (P< 0.05).Conclusion Febuxostat 40 mg qd has a better efficacy and acceptable safety concerns than the other dose and allopurinol in gout patients with normal organ function.
Gout;Febuxostat;Allopurinol;Urate lowering therapy
R593.2
A
1672-6170(2016)06-0068-03
2016-01-09;
2016-06-24)