Hyperbaric oxygen therapy decreases mortality due to Fournier’s gangrene:a retrospective comparative study
2021-03-03OmarresMarleyRibeiroFeitosaJosJoaquimRibeirodaRochaJulianaMamedeMirandaLucianaEgydiodosSantosArturCuryresHugoParradeCamargoRogrioSerafimParra
Omar Féres,Marley Ribeiro Feitosa,José Joaquim Ribeiro da Rocha,Juliana Mamede Miranda,Luciana Egydio dos Santos,Artur Cury Féres,Hugo Parra de Camargo,Rogério Serafim Parra*
Department of Surgery and Anatomy,Ribeirão Preto Medical School,University of São Paulo,Ribeirão Preto,Brazil
Abstract There is no consensus about the role of adjunctive hyperbaric oxygen therapy (HBOT) in the management of Fournier’s gangrene.The aim of this study was to compare the evolution of patients with Fournier’s gangrene treated with all classical measures with and without adjuvant HBOT.A retrospective comparative study regarding the evolution of patients treated for Fournier’s gangrene was conducted in two periods.In period I,from 1990 to 2002,patients received standard treatments for Fournier’s gangrene,which consisted of surgical debridement,antibiotic therapy and intensive care.In period II,from 2012 to 2019,adjunctive HBOT was added to the classical management strategy.All patients were assigned into four groups according to the anatomical severity classification and the area affected after the first debridement.This classification ensured that the groups could be comparable.The total number of patients in this study was 197,and these patients were divided into control group (118/59.9%) and HBOT group (79/40.1%).The mean age,comorbidities,and anatomical severity classification were similar between the two groups.In period I,34 out of 118 (28.8%) patients died,while in the HBOT group,3 out of 77 (3.7%) patients died (P < 0.001).The use of adjuvant HBOT in combination with classical treatment was associated with reduced mortality.This study was approved by the Institutional Review Board and the Ethics Committee of Ribeirão Preto Medical School,University of São Paulo,Brazil(No.08/2018) on May 2,2018.
Key words:fascitis; gangrene; hyperbaric oxygenation; infection; morbidity; mortality; necrotizing; treatment outcome; wound healing
INTRODUCTION
Fournier’s gangrene (FG) is a polymicrobial infection caused by aerobic and anaerobic microorganisms that act in synergy to cause necrotizing fasciitis affecting mainly the genital,perineal and perianal regions.1-3This infectious process occurs through obliterating endarteritis and leads to thrombosis of the cutaneous and subcutaneous vessels and,consequently,necrosis of the skin in the affected region.2,4Without treatment,the process may not only rapidly extend to the anterior abdominal wall,dorsal region,upper limbs and retroperitoneum but also induce sepsis,multiple organ failure and death.1,5-7
Some systemic diseases are risk factors for the development of gangrene,including diabetes mellitus,alcoholism,hypertension,obesity,smoking,immunosuppressive conditions such as human immunodeficiency virus infection,radiotherapy and chemotherapy.8-12FG was initially described as a disease of unknown cause,but it is now known that an underlying pathological process can be found in most cases,although in a significant number of patients,the cause cannot be determined.8,11,13,14Foci in the urogenital tract that have been described in the literature are due to several causes,such as urethral stenosis,delayed bladder sampling,scrotal abscess,orchitis,epididymitis,renal abscess,traumatic urethral catheterization,urethral calculus,bladder cancer,penile cancer,prostate massage and prostate biopsy.15,16In the digestive tract,foci originating from perianal abscesses,colon and rectal cancer,appendicitis and acute diverticulitis,Crohn’s disease,incarcerated hernias and perforation of the rectum by a foreign body (chicken bone) have been reported.17-19
The most frequent manifestations are pain,erythema,edema and necrosis of the scrotum or perianal and perineal region in association with fever and chills.On the other hand,the disease may manifest insidiously or as sepsis.14,20,21Other local manifestations include blisters,crepitus,cyanosis,and secretion with a strong and repulsive stinking odor.It should be remembered that skin manifestations constitute the “tip of the iceberg” as the infection spreads rapidly and aggressively along deep fascial planes.4As previously mentioned,FG is a polymicrobial infection,causing a true environment where aerobic and anaerobic bacteria are found,and it is usually nonpathogenic but is associated with devastating consequences under favorable conditions.Acting synergistically,these bacteria act through different mechanisms,contributing not only to the seriousness but also to the fast spread of the process.1,22
The classical treatments for FG consist of broad-spectrum antibiotic therapy and emergency surgical debridement,with the aim of removing all necrotic tissue,interrupting the progression of the infectious process and minimizing systemic toxic effects.23-25The extent of necrotic tissue resection,until viable tissue is reached,should guide the surgeon as the aim to be achieved during the surgical procedure (Figure1).

Figure1:Fifth postoperative day of a complicated hemorrhoidectomy in a 37-year-old woman,without comorbidities.
Hyperbaric oxygen therapy (HBOT) is a therapeutic modality consisting of pressurization in a hermetically sealed chamber with 100% oxygen.26HBOT exerts a direct antibacterial effect on anaerobes,and the activity of endotoxins is reduced in the presence of high tissue levels of oxygen.The benefits from this treatment include improved phagocytic action of neutrophils,increased proliferation of fibroblasts and angiogenesis,reduced edema due to vasoconstriction,increased intracellular antibiotic transport and oxygen-free radical synthesis.27,28
HBOT plays a prominent role in the physiopathology of anaerobic bacteria.Several authors recommend the use of HBOT as an adjuvant treatment for this type of infection.29HBOT can decrease the extent of necrosis and reduce mortality and morbidity rates.30,31This therapy has a facilitating effect on wound healing and accelerates recovery after debridement,even reducing the need for further surgery.32
Many controversial issues exist surrounding the role of HBOT in the management of FG.Some studies show that HBOT reduces mortality in patients with FG.30,33However,other data do not support the routine use of HBOT in the treatment of FG.34Thus,we conducted this study to compare the evolution of patients treated with all classical measures with or without adjuvant HBOT oxygen therapy.
SUBJECTS AND METHODS
Ethics approval
This study was approved by the Institutional Review Board and the Ethics Committee of Ribeirão Preto Medical School,University of São Paulo,Brazil (No.08/2018) on May 2,2018.Written informed consent was obtained from enrolled patients and their legal guardians.All procedures were in accordance with the ethical standards of the responsible institutional and national committee on human experimentation and with the 1964Helsinki Declarationand its later amendments or comparable ethical standards.
Study design and data collection
We conducted a retrospective study using the HBOT database at Ribeirão Preto Hyperbaric Medicine Center,affiliated with University of São Paulo,Brazil.We also reviewed electronic medical records from the emergency unit at Ribeirão Preto Medical School and at São Paulo Hospital (Ribeirão Preto,São Paulo,Brazil).In both groups,all patients with FG were included.However,we excluded patients who were operated by other surgical teams,to avoid selection bias.In the HBOT database,the following variables were collected continuously and prospectively:name and registration number of patients,age,sex,comorbidities,HBOT indications,number of sessions,complications and mortality-related HBOT.All clinicodemographic information,including anatomic classification of FG,photographic documentation of gangrene and 30-day mortality rates,was confirmed in electronic medical records.The patients were divided into two groups according to the treatment period and the place where they underwent surgical treatment for FG.Control group (n= 118) was formed by patients who underwent traditional treatment for Fournier's syndrome (debridement care,antibiotic therapy and intensive care) at the Emergency Unit of the Ribeirão Preto Medical School from 1990 to 2002.All patients were operated by the same surgical team.HBOT group (n= 79) comprised patients with Fournier’s syndrome who underwent traditional treatment combined with HBOT at Hospital São Paulo from 2012 to 2019.The patients were operated by the same surgical team of control group or by another group with the same surgical training.
HBOT
All patients in HBOT group underwent sessions of adjuvant HBOT.The sessions were performed daily,for 2 hours,with a pressure of 2.4 ATA (243.18 kPa).The protocol used was 15 consecutive sessions of HBOT.If the healing process was complete before 15 sessions,the treatment was interrupted.In some cases,the number of sessions was higher due to incomplete healing.The evolution of the treatment was evaluated by a team composed of a nurse and a physician who work with HBOT,and a coloproctologist who provided basic care for the disease and decided on the maintenance or interruption of HBOT.The hyperbaric device used for all patients was a monoplace Sechrist 2800 Chamber (Anaheim,CA,USA).
Anatomical classification of FG
All patients were classified according to the Féres classification,35which separates patients into four groups of anatomical severity according to the area affected after the first debridement (Table1).As this classification is based on the affected area,it can be done retrospectively as long as there is photographic documentation right after the first debridement.This classification ensured that the groups could be comparable.
Comorbidities
Comorbidities between the two groups,such as diabetes,hypertension,alcoholism,and smoking,which are factors that interfere with the prognosis,were also evaluated.
Colostomy and cystostomy
Colostomy and cystostomy rates were evaluated in the two groups.Colostomy was performed when the anal sphincter was compromised by the necrosis.Cystostomy was performed in those cases when vulva or penis where compromised.Both surgical procedures were performed on patients with extensive necrosis.

Table1:Anatomical classification of the extent of necrosis area and correlation with mortality,according to Féres et al.35
Statistical analysis
Categorical variables are expressed as absolute and relative frequencies.Continuous variables are expressed as the mean ±standard deviation (SD).The Kruskal-Wallis test was used to check for the normality of variables.Comparisons of categorical variables between groups were performed using Fisher’s exact test.AP-value < 0.05 was considered statistically significant.GraphPad Prism 8 (GraphPad,San Diego,CA,USA)was used for statistical analysis.
RESULTS
Clinical and demographic characteristics of FG patients
The total number of patients in this study was 197,and the patients were divided into control group,which included 118 patients (59.9%),and HBOT group,which included 79 patients(40.1%).The average number of HBOT sessions performed in HBOT group was 15 (range 11-26).The average age in control group was 46.6 years (range 1-82) and that in HBOT group was 48.2 years (10-81).Sixteen out of 118 patients(13.5%) in control group and 9 out of 79 patients (11.4%) in HBOT group needed mechanical ventilation.There was no significant difference between the groups.In both periods,there were a higher proportion of men than women.The data are shown in Table2.
Anatomical classification of FG patients with or without HBOT
Regarding the anatomical severity classification,there was no significant difference between control and HBOT groups(P> 0.05; Figure2).
Comorbidities of FG patients with or without HBOT
Concerning the risk factors,such as systemic arterial hypertension (P= 0.42),diabetes mellitus (P= 0.21),alcoholism(P= 0.43),and smoking (P= 0.51),there was no significant difference between control and HBOT groups (Table2).
Colostomy and cystostomy of FG patients with or without HBOT
Complementary surgical procedures,such as colostomy and cystostomy had similar rates in both groups (P= 0.84 andP= 0.76,respectively).
Antibiotic therapy and surgical approach of FG patients with or without HBOT
In control group,the combination of gentamicin,metronida-zole and crystalline penicillin (triple antibiotic therapy) was used (n= 82).In older patients (> 60 years),or those with impaired renal function,gentamicin was replaced by ceftriaxone (n= 36).In cases of sepsis,with the need to broaden the spectrum,imipenem associated with vancomycin was used(n= 46).In HBOT group,the combination of ceftriaxone,metronidazole and oxacillin (triple antibiotic therapy) was used (n= 79).In cases of sepsis with the need to expand the spectrum,meropenem associated with vancomycin was used(n= 14).In addition,in control group all cases were operated on by the same surgical team.In HBOT group,about half (n= 38) of the cases were operated by the same surgical team of control group,and the rest (n= 41) were operated on by another team with the same surgical training.
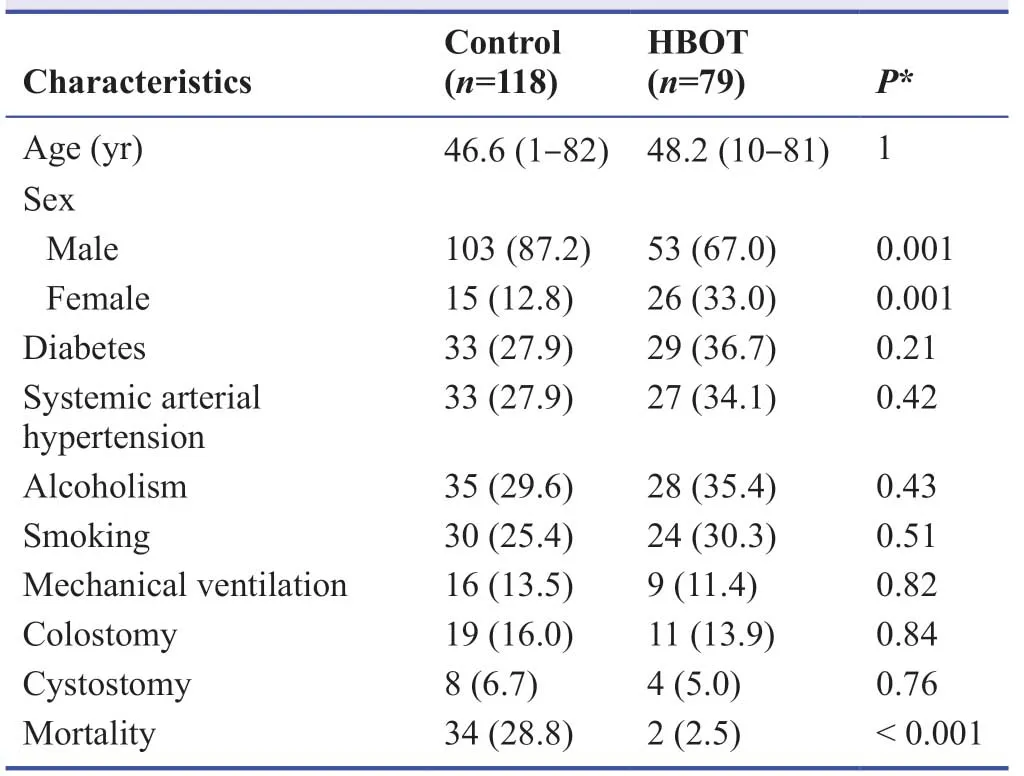
Table2:Baseline Fournier’s gangrene patient’s characteristics
Mortality of FG patients with or without HBOT
In control group,34 out of 118 (28.8%) patients died,while in HBOT group,3 out of 77 patients died (3.7%).This difference was statistically meaningful (P< 0.001; Figure3).
DISCUSSION
Adjunctive HBOT,which is associated with surgical management,reduced mortality in patients with FG.Even with the extensive debridement and adequate antibiotic therapy established in period I,the mortality rates remained high.Some authors have tried to identify and validate factors that may be related to mortality.5,16,18,34However,the conclusions of these studies are not consistent.One study concluded that the time elapsed between the beginning of the disease and surgical treatment is the most important factor affecting mortality.18In another study,the authors concluded that the duration of symptoms from the onset of the condition to hospitalization is a contributing factor to mortality and identified anorectal location,renal failure and extension of gangrene as other important factors.11,35

Figure2:Anatomical classification of Fournier’s gangrene.
In another study where the authors analyzed several factors by scoring physiological changes based on the Acute Physiology and Chronic Health Evaluation II score,they concluded that the main factor influencing mortality is the set of physiological changes that can be grouped in what the authors called the Fournier Gangrene Severity Index.36Confirmation of the validity of the Fournier Gangrene Severity Index was established in two studies37,38but questioned in a third,where the authors concluded that this index may not reflect the severity of the disease.The main factors related to mortality in FG are the time elapsed between the beginning of the disease and surgical treatment,extent of necrosis,systemic repercussions represented by physiological changes reflecting the impact of the disease on the patient and early use of HBOT.36
We have previously proposed an anatomic classification and correlated the extent of the disease and mortality rates in FG.Since the extent of the disease is easily measurable,we chose to use this methodology to compare our patients who did and did not received HBOT treatment.In this study,there were no significant differences between the groups according to the anatomical severity classification,showing that the severity of control and HBOT groups were similar and could be comparable.The comorbidities and complementary surgical procedures in control and HBOT groups were not different,showing again that both groups were similar.Additionally,the two antibiotic therapy schemes used in both periods have a similar spectrum of action,showing that the results were not influenced by the use of better antibiotics.In both periods,the basic surgical principles included wide debridement of the devitalized tissue.Thus,there was no interference from the surgical technique in the good results of HBOT group.
The majority of published studies show a beneficial role of HBOT in reducing mortality due to FG.One study,with a total of 161 patients with a diagnosis of FG,showed that mortality due to FG was observed in 36.0% of patients who did not undergo HBOT and in 19.4% of patients who underwent HBOT,showing that HBOT is an independent predictor of reduced mortality due to FG.30Another study showed that the mortality rate was lower in the HBOT group (2/16,12.5%)than in the non-HBOT group (4/12,33.3%).39
Another study included 42 consecutive patients with necrotizing fasciitis who presented to a major referral center and were treated with adjunctive HBOT as part of an aggressive program of surgery,antibiotics,and critical care.40Compared to “standard” regimens for necrotizing fasciitis,their experience with HBOT from adjunctive to comprehensive and aggressive management demonstrated reduced mortality (34%vs.11.9%).The treatments were safe,and no surgical delays or interference to standard therapy could be attributed to HBOT.40One study concluded that early diagnosis combined with extensive surgical debridement,broad-spectrum antibiotic therapy and oxygen therapy,when available,are important measures to contain the rapid progression of the disease,thus decreasing the mortality rate.33
There are few reports that do not support the routine use of HBOT in the treatment of FG.A report showed mortality rates of 12.5% in the non-HBOT group and 26.9% in the HBOT group.34However,this study was limited by the small number of patients included (n= 42),and adjuvant HBOT was indicated in patients who were more ill.Thus,these facts can explain the higher mortality in the HBOT group.In our study,which included 179 patients,the mortality of the HBOT group was 3.7%vs.28.8% in the non-HBOT group,showing a decrease in mortality with HBOT.
Even critical patients with sepsis who were admitted to the intensive care unit and required mechanical ventilation and the use of vasoactive drugs,can undergo HBOT and present benefits from this treatment.41In our study,9 out of 79 patients(11.4%) needed mechanical ventilation during HBOT,and no incidents were observed.Beginning HBOT soon after the first debridement increases the possibility of a satisfactory evolution,in terms of both wound evolution and systemic improvement of the patients’ septic condition (Figure4).
Literature on this subject is scarce and controversial.Some studies present case reports and small cohorts.42Others present larger series.8However,few studies are randomized and prospective double-blind trials.43The indications for HBOT in FG are classical,and this treatment presents satisfactory results.30,31,38Our study clearly showed that the adjuvant use of HBOT reduces mortality.
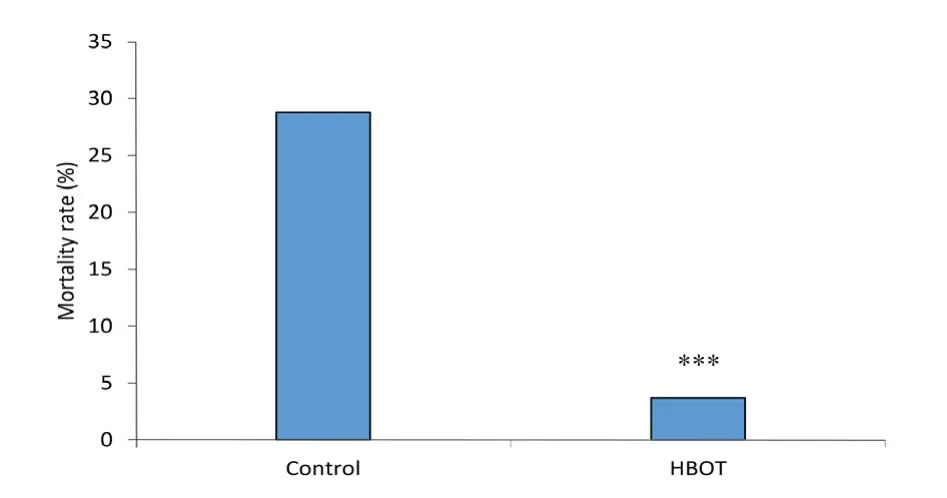
Figure3:Mortality rate of Fournier’s gangrene patients with or without HBOT.

Figure4:Evolutionary aspects of Fournier’s gangrene treated by adjuvant treatment with hyperbaric oxygen therapy showing a good evolution of the granulation and scar tissue.
Based on our 30 years’ experience in treating these patients with or without adjuvant HBOT,we were able to clearly and unequivocally see the effect of this treatment.The patients improved locally and systemically.There was a decrease in morbidity and mortality and a shortened hospitalization period.10,30,34,43-49Thus,we recommended the systematic use of adjuvant HBOT for this serious condition.
Despite being safe,50this method is not without complications; the most common complication is ear barotrauma,which sometimes interrupts treatment.51,52Claustrophobia(especially in monoplace chambers) can occur in up to 12%of patients and is another problem that can lead to treatment interruption.53In our series,we observed no complications from the hyperbaric treatment,and the patients completed the treatment successfully.
Most studies have series with a lower number of patients and do not present a comparison of similar groups as our study.According to our review,our study,with 197 patients,represents one of the largest published series on this subject in the medical literature which strengthen our findings.However,some limitations should be noted.Among the limiting factors of this study,we can mention that this comparative study was retrospective and historically compared two periods.This may lead to some bias in the analysis,but prospective randomized studies would not be ethical for this condition as this method is already classically used and leads to benefits; thus,depriving patients of treatment would not be recommended.54Another aspect that may have influenced and caused some bias in the results is the fact that not all patients were operated on by the same surgeon and in the same department,which may lead to differences.However,groups I and II were similar in terms of age,comorbidities and anatomical severity classification.In short,early diagnosis combined with surgical debridement,broad-spectrum antibiotic therapy and HBOT need to be performed in all patients.We can conclude that the use of adjuvant HBOT for FG reduced mortality.
Author contributions
Study design:OF; data collection:OF,LES; data analysis and interpretation:OF,MRF,JJRR,JMM,LES,ACF,HPC,RSP; data analysis:RSP; statistical analysis:MRF; manuscript draft:OF; manuscript writing:RSP; manuscript revision:OF,MRF,RSP; manuscript supervision:JJRR.All authors contributed to the analysis and interpretation of data,revision of the manuscript for important intellectual content,granted final approval of the version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflicts of interest
The authors declared no potential conflicts of interest with respect to the research,authorship and/or publication of this article.
Financial support
There has been no financial support for this work that could have influenced its outcome.
Institutional review board statement
This study was approved by the Institutional Review Board and the Ethics Committee of Ribeirão Preto Medical School,University of São Paulo,Brazil (No.08/2018,May 2,2018).All procedures were in accordance with the ethical standards of the responsible institutional and national committee on human experimentation and with the 1964Helsinki Declarationand its later amendments or comparable ethical standards.
Declaration of patient consent
We certify that we have obtained all appropriate patient consent forms.All images/photos used in the manuscript were taken under the patients’ consent and authorization,as long as their names were not disclosed and confidentiality regarding their identity was respected.These patients understand that their names and initials will not be published and due efforts will be made to conceal their identity,but anonymity cannot be guaranteed.
Reporting statement
The writing and editing of the article were performed in accordance with the Transparent Reporting of Evaluations with Nonrandomized Designs (TREND) Statement.
Copyright transfer agreement
The Copyright License Agreement has been signed by all authors before publication.
Data sharing statement
Datasets analyzed during the current study are available from the corresponding author on reasonable request.
Plagiarism check
Checked twice by iThenticate.
Peer review
Externally peer reviewed.
Open access statement
This is an open access journal,and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License,which allows others to remix,tweak,and build upon the work non-commercially,as long as appropriate credit is given and the new creations are licensed under the identical terms.
杂志排行

Medical Gas Research的其它文章
- High-flow hydrogen inhalation might suppresses the immune function of middle-aged participants:a selfcontrolled study
- The effect of dexmedetomidine on decrease of cough,hemodynamic parameters and Ramsay score versus lidocaine during general anesthesia:a randomized clinical trial
- Evaluation of audible leak versus pressure volume loop closure for polyvinyl chloride cuff and polyurethane microcuff in endotracheal tube inflated with air:a prospective randomized study
- The role of nitric oxide in peptic ulcer:a narrative review
- Therapeutic effects of hyperbaric oxygen:integrated review
- A new mechanistic approach for the treatment of chronic neuropathic pain with nitrous oxide integrated from a systems biology narrative review