Evaluation of audible leak versus pressure volume loop closure for polyvinyl chloride cuff and polyurethane microcuff in endotracheal tube inflated with air:a prospective randomized study
2021-03-03PrashantKumarAbhilashaJyotiSharmaKiranpreetKaurMamtaBharadwajAnuSingh
Prashant Kumar,Abhilasha,Jyoti Sharma ,Kiranpreet Kaur,Mamta Bharadwaj,Anu Singh
1 Department of Anaesthesiology and Critical Care,Pt.B D Sharma PGIMS,Rohtak,Haryana,India
2 Department of Anaesthesiology,All India Institute of Medical Sciences,Bathinda,Punjab,India
Abstract Cuff pressure of endotracheal tube (ETT) must be high enough to seal the trachea,and must be low enough to allow adequate perfusion of tracheal mucosa.Compared with polyvinyl chloride (PVC) cuffed tubes,polyurethane cuffed tubes protect more efficiently.Different methods of ETT cuff pressure maintenance in practice have been reported.We planned to compare ETT cuff pressure using different techniques in PVC and polyurethane microcuff tubes in a prospective randomized study.Eighty surgical patients between 16-65 years belonging to American Society of Anesthesiologists physical status I-III,scheduled for orotracheal intubation under general anaesthesia,were included.All enrolled patients were randomized into four groups (n = 20 per group),followed by corresponding treatments,including intubation by PVC ETT or polyurethane microcuff ETT and cuff inflation by auscultation of audible leak or pressure volume loop.Amount of air required to inflate cuff was more in polyurethrane tube as compared to polyvinyl tube.While comparing the two methods of cuff inflation,less volume of air was required in pressure volume loop method.We concluded that PVC cuff tube and polyurethane microcuff tube both are safe tubes used in adult patients.However,when inflated using same technique polyurethane microcuff tubes required larger volume to inflate cuff.Further,pressure generated in polyurethane microcuff tubes in much lower than PVC tubes.The study was approved by the Institutional Ethics Committee of Pt B D Sharma,PGIMS,Rohtak (No.IEC/Th/18/Anst15) on January 20,2018 and registered with Clinical Trials Registry-India (registration No.CTRI/2019/01/017170) on January 18,2019.
Key words:cuff inflation; cuff pressure; manual method; microcuff; polyvinyl chloride tube; pressure volume loop; tracheal mucosa
INTRODUCTION
Endotracheal tube (ETT) is important during anesthesia to maintain airway.Its critical function is to seal airway,prevent aspiration and leak of pharyngeal contents into trachea.1Cuffpressure must be high enough to seal the trachea to prevent aspiration of oropharyngeal secretions and avoid air leaks to atmosphere.Also,it must be low enough to allow adequate perfusion of tracheal mucosa.2,3
The common methods used in routine clinical settings for inflation of endotracheal cuff pressure are finger palpation of pilot balloon,inflation to precise pressure (25 cmH2O,1 cmH2O = 0.098 kPa) and sealing method.2,4But none of them is a definitive method and an intraoperative cuff pressure monitoring by manometer or any electronic device has been developed.Currently a cuff pressure of 20-30 cmH2O is recommended for minimal risk of complications.5The aneroid manometer is the most commonly used device for monitoring cuff pressure.The pressure volume (PV) loop is the continuous real time pulmonary graphic incorporated in the monitoring system of anesthesia machines.Pressure volume loop is used for the assessment of dynamic lung compliance,detection of lung over inflation and presence of air leak.6Various types of tubes are used in routine anesthesia practice with their added advantages.Most commonly used polyvinyl chloride (PVC)tubes are cheap,easy to handle and disposable.On the other hand polyurethane cuffed tubes made of ultrathin (7 μm)material prevent leakage and microaspiration by providing a better seal.7
When cuff comprised of PVC material is inflated,tiny channels are created that encourage collection of secretions within the folds.For prevention of microaspiration intracuffpressures as high as more than 30 cmH2O have been used to seal PVC cuffs.Cuff material made of ultrathin (10 μm)polyurethane allows sealing of the lumen of the trachea at pressures of 15 cmH2O or lower.7This is because of the polyurethane material draping over the irregular tracheal mucosal contours.Compared with PVC cuffed tubes,polyurethane cuffed tubes protect more efficiently against microaspiration or substantial leakage of secretions.8Different methods of ETT cuff pressure maintenance in practice have been reported successfully with varied opinions about their efficacy.5We conducted the following study to compare ETT cuff pressure using different techniques in PVCversuspolyurethane microcuff ETT tubes.
SUBJECTS AND METHODS
Design
The prospective randomized,clinical study was conducted in the Department of Anaesthesiology,Pt.B D Sharma Post Graduate Institute of Medical Sciences,Rohtak,India.The study was approved by the Institutional Ethics Committee of Pt B D Sharma,PGIMS,Rohtak (No.IEC/Th/18/Anst15) on January 20,2018 and registered with Clinical Trials Registry-India (registration No.CTRI/2019/01/017170) on January 18,2019.Writing and editing of the article was performed in accordance to the CONsolidated Standards Of Reporting Trials(CONSORT) statement.The flow chart is shown in Figure1.
Subjects
Totally 104 patients between 16-65 years belonging to American Society of Anesthesiologists physical status I-III,9scheduled for orotracheal intubation during elective surgery under general anesthesia,were assessed for eligibility for the study.Patients with risk of pulmonary aspiration,body mass index > 35 kg/m2,and obstetric patients were excluded.Four patients were excluded as they did not meet inclusion criteria.Eighty patients after taking written informed consent were included in the study.
Anesthesia management
A standard anesthesia protocol was followed in all the patients.Either PVC (Portex®; Smiths Medical,Inc.,Plymouth,MN,USA) or polyurethane microcuff ETT (Kimberly-Clark*MICROCUFF*; Kimberly Clark,Health Care,Atlanta,GA,USA) of size 7.0 mm ID and 8.0 mm ID was used in female and male patients respectively.ETT was checked before use and it was lubricated with water based gel.After preoxygenation with 100% oxygen by facemask,induction of anesthesia was done with injection fentanyl citrate (Fent; Neon Laboratories Limited,Mumbai,India) 2 μg/kg and injection propofol (Neorof; Neon Laboratories Limited) 2 mg/kg.Nondepolarizing neuromuscular blocking agents were used to facilitate ETT insertion.All the patients were ventilated for 3 minutes using oxygen in nitrous oxide 50% and sevoflurane to achieve minimum alveolar concentration of 1-1.3.
Group allocation
Using computer generated randomization number table,the patients were divided in 4 groups with 20 in each group.Endotracheal intubation with the ETT assigned was done by direct laryngoscopy in standard sniffing position by PVC tube or polyurethane microcuff tube (Figure2A and B respectively).ETT cuff was inflated with air (mL) and fixed after checking square wave capnogram and bilateral equal air entry.Group A1 (n= 20):Patients were intubated by PVC ETT and cuffinflated by manual method using auscultation of audible leak.Group A2 (n= 20):Patients were intubated by PVC ETT and cuff inflated with air guided by PV loop (Primus®; Drager India Pvt.Ltd.,Mumbai,India).Group B1 (n= 20):Patients were intubated by polyurethane microcuff ETT and cuff inflated by manual method using auscultation of audible leak.Group B2(n= 20):Patients were intubated by polyurethane microcuffETT and cuff inflated with air guided by PV loop.Once stabilized,the pressure was checked with aneroid manometer by connecting pilot balloon of ETT via stopcock.Anaesthesia was maintained by inhalational agents or intravenous propofol as per discretion of anaesthesiologist.Neuromuscular blockade was maintained with supplemental dosages of nondepolarizing neuromuscular blocking agent.
Measurements Amount of air required to inflate cuff
In audible leak technique group,ETT cuff was infalted initially by 2 mL of air followed by increments of 0.5 mL air using 2 mL syringe till disappearance of harsh audible sounds on auscultation and acceptable palpation of the external pilot balloon was attained.Total amount of air required was recorded.In PV loop technique group,ETT cuff,both types PVC tube or polyurethane microcuff,were inflated initially by 2 mL of air followed by increments of 0.5 mL air using 2 mL syringe until the complete closure of the PV loop is displayed on the Drager Anesthesia Work Station monitor,i.e.,when the expiratory limb reached at zero volume and met the starting point of inspiratory limb.Total amount of air required was recorded (Figure3).

Figure1:The flow chart.
Intra-cuff pressure
Once adequate seal was achieved intra-cuff pressure was measured using pressure manometer (Portex Smith,Norwell,MA,USA) and was recorded.
Tidal volume discrepancy
Measure the effect of decreasing lung compliance on the difference between effective tidal volume and tidal volume at the ETT in the patient with no leak around the ETT.
Changes in intra-cuff pressure
Cuff pressure was recorded again after 1 hour and at the end of surgery.Any change in pressure was noted,if pressure exceeds more than 20 cmH2O,air of cuff was aspirated to maintain intra-cuff pressure of 20 cmH2O in aliquots of 1 mL air.Volume of air aspirated was noted.
Cuff volume before extubation
Before extubation,volume of air aspirated for complete deflation was recorded from ETT.
Tube inspection
Tube was visibly inspected for any secretions on distal portion of the cuff.
Complications
Patient was enquired for any evidence of sore throat,hoarseness of voice,and cough 30 minutes post-extubation and thereafter,was reassessed for above complaints next day in the ward.
Sample size
Our sample size calculation done by using https://www.openepi.com/SampleSize/SSCohort.htm based on Almarakbi and Kaki10recorded the amount of air to inflate the ETT cuff in PV loop technique in comparison to the audible Leak technique using PVC ETT.Assuming these as reference values,the minimum required sample size at 5% level of significance and 95% power was calculated as at least nine patients in each group.However,keeping in mind the duration of study and also a large number of such patients reporting to our hospital,we proposed to take 20 patients in each group.
Statistical analysis
The entire data was entered in Microsoft excel file and analyzed using Statistical Package for the Social Sciences version 17.0 software (SPSS Inc.,Chicago,IL,USA).The quantitative variables in all groups were expressed as mean ± standard deviation (SD) and one-way analysis of variance followed by F test was used for intergroup comparison.For multiple comparisons,post hocanalysis was done with Tukey’s test.Categorical variable were analyzed using Chi-square test.AP-value < 0.05 was considered statistically significant.
RESULTS
Demographic profile was comparable within all groups (Table1).

Figure2:The morphology of polyvinyl chloride endotracheal tube(A) and polyurethane microcuff endotracheal tube (B).

Figure3:Pressure volume loop method of cuff inflation.

Table1:Demographic profile in surgical patients using different techniques in PVC versus polyurethane microcuff ETT tubes
Comparison of different types of tracheal tubes
Tables 2 and 3 reveal that the amount of air required to inflate cuff is more in polyurethrane tube as compared to polyvinyl tube (group B1vs.group A1:P< 0.001,group B2vs.group A2:P= 0.335).Mean pressure of cuff is less in polyurethrane tube (group B1vs.group A1:P< 0.001,group B2vs.group A2:P= 0.039).After one hour,intracuff pressure was less in polyurethrane tube (group B1vs.group A1:P= 0.025,group B2vs.group A2:P= 0.006).Removal of 1 mL of air to maintain intracuff pressure at 20 cmH2O was required in only one patient with polyurethrane cuff as compared to 18 patients with PVC tube (group B1vs.group A1:P= 0.044,group B2vs.group A2:P< 0.001).Till the end of surgery intra-cuff pressure again increased to a higher extent in PVC tube as compared to polyurethrane tube (group A1 and A2vs.group B2:P= 0.031 < 0.001,group A2vs.group A1:P=0.031,group B2vs.group A1:P< 0.001).
Comparison of different methods of cuff inflation
While comparing the two methods of cuff inflation,less volume of air was required in PV loop method (group A1vs.group A2:P= 0.99,group B1vs.group B2:P< 0.001;Tables 2 and 3).

Table2:Variation in intra-cuff air with reference to different stages in surgical patients using different techniques in PVC versus polyurethane microcuff ETT tubes
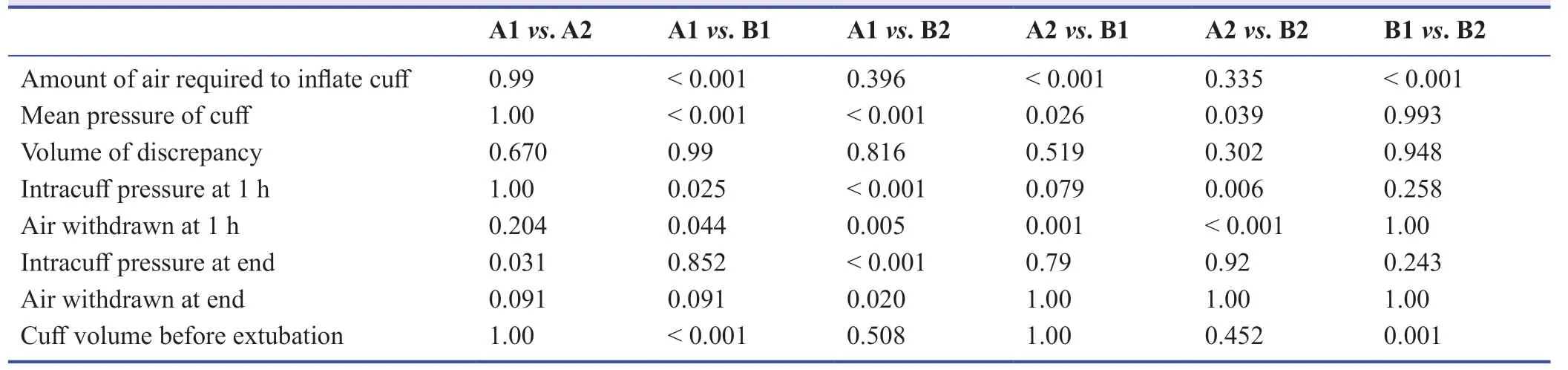
Table3:P values in different types of tracheal tubes and different types of cuff inflation methods in surgical patients using different techniques in PVC versus polyurethane microcuff ETT tubes
Side-effects of different types of tracheal tubes or cuff inflation
It was observed that under group A1,85% of the patients had nil secretions,5% each had mucous plugs,secretions and blood respectively.For group A2,80% patients had no secretions,10% had blood and 5% each had Mucous Plugs and light secretions.For group B2,95% patients had no secretions while 5% had secretions.For group B2,95% had no secretions and 5% had Mucous Plugs.Further,it was observed that there was a significant difference in secretion distribution among four groups (P< 0.001; Table4).None of the patients had hoarseness of voice in all the groups after 30 minutes as well as after 24 hours.There was no significant difference in distribution of patients with cough and sore throat between the four groups after 30 minutes as well as after 24 hours (Table5).
DISCUSSION
Volume of air to inflate cuff was more in polyurethane ETT than the PVC ETT.A significant reduction of required air in PV loop technique used for cuff inflation in polyurethanetube.These observations were strengthened by Kaki and Almarakbi6evaluated use of PV loop closure to check for ETT cuff inflation.They observed that the lower volume of air was required in PV loop technique than the other two techniques.Amount of volume was used in pilot balloon palpation method and fixed preset pressure was 5.26 ± 0.46 mL and 4.4 ± 0.36 mL,respectively.Searched literature was silent about amount of air required to inflate polyurethane microcuff in elective surgeries in adult patients.

Table4:Comparison of any secretions over distal cuffamong surgical patients with different types of tracheal tubes
There was an apparent reduction in cuff pressures in polyurethane cuff tubes.Mali et al.4observed higher cuff pressures in their study group further the cuff pressures were significantly lower in sealing group compared with constant pressure group and highest in finger palpation group.Mahmoodpoor et al.7evaluated comparison of prophylactic effects of polyurethane cylindrical or tapered cuff and PVC cuff ETTs on ventilator associated pneumonia and maintained mean cuff pressure in PVC ETT was 24.20 ± 0.47 mmHg,in polyurethane taperguard ETT was 24.10 ± 0.49 mmHg and 24.07 ± 0.48 mmHg was for polyurethane sealguard ETT (P> 0.05).Mhamane et al.11evaluated use of microcuff ETTs in pediatric laparoscopic surgeries.They observed mean sealing pressure was 11.72 cmH2O.We have also noted similar values of sealing pressure despite our population being different that is adult population.We observed in our study cuff pressure was lower in polyurethane microcuff ETT than the PVC ETT.Searched literature was silent on comparing cuff pressure in between PVC ETT and polyurethane microcuff ETT in elective surgeries.
Requirement of air withdrawn from cuff (if cuff pressure was more than 20 cmH2O after 1 hour) was less in polyurethane microcuff ETT compared to PVC tube.There is an observable increase in volume of cuff air with time in PVC cuff ETTs resulting in increased pressure.Polyurethane microcuff ETTs did not show significant increase in volume with passage of time.The searched literature did not have data to compare these observations.However,the difference might have resulted from absorption or diffusion due to different characteristics of both types of cuffs.Further,we have used 50% nitrous inoxygen in our all patients.Change in cuff pressure and air withdrawn was higher in PVC ETT.

Table5:Side effects reported postoperatively among surgical patients with different types of tracheal tubes
It is apparent that despite higher cuff volumes in both the groups of polyurethane ETT,the pressures maintained were significantly low which of paramount importance.Secretions over distal cuff were less in polyurethane ETT.Lower incidence of postoperative complications in polyurethane ETT compared to the PVC ETT which might be due to lower cuffpressure in polyurethane ETT.
For many months he had admired a beautiful sports car in a dealer1 s showroom, and knowing his father could well afford it, he told him that was all he wanted
There were few limitations to our study.Patients included belong to single geographical profile,i.e.Northern India in Asia Pacific region.Although sample size has been calculated based on literature still this small sample size may not represent whole population.
In summary,with observations made and compared with available literature it is concluded that PVC cuff tube and polyurethane microcuff tube both are safe endotracheal tubes to be used in adult patients.However,when inflated using same technique polyurethane microcuff tubes require larger volume to inflate cuff than the PVC tubes.Further,pressure generated in polyurethane microcuff tubes is much lower than PVC cuff tubes.
Author contributions
Study design:PK,JS,KK; literature search:PK,A,JS,MB,AS; data collection:PK,A,KK,MB,AS; manuscript writing:JS,MB.All authors read and approved the final version of manuscript for publication.
Conflicts of interest
None declared.
Financial support
None.
Institutional review board statement
The study was approved by the Institutional Ethics Committee of Pt B D Sharma,PGIMS,Rohtak (No.IEC/Th/18/Anst15) on January 20,2018 and registered with Clinical Trials Registry-India (registration No.CTRI/2019/01/017170) on January 18,2019.
Declaration of patient consent
The authors certify that they have obtained patient consent forms.In the form,patient have given their consent for their images and other clinical information to be reported in the journal.The patients understand that their names and initials will not be published.
Reporting statement
The writing and editing of the article were performed in accordance with the CONsolidated Standards Of Reporting Trials (CONSORT)Statement.
Biostatistics statement
The statistical methods of this study were reviewed by Dr.Madhur Verma from All India Institute of Medical Sciences Bathinda,Punjab,India.
Copyright license agreement
The Copyright License Agreement has been signed by all authors before publication.
Data sharing statement
Datasets analyzed during the current study are available from the corresponding author on reasonable request.
Plagiarism check
Checked twice by iThenticate.
Peer review
Externally peer reviewed.
Open access statement
This is an open access journal,and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License,which allows others to remix,tweak,and build upon the work non-commercially,as long as appropriate credit is given and the new creations are licensed under the identical terms.
杂志排行

Medical Gas Research的其它文章
- High-flow hydrogen inhalation might suppresses the immune function of middle-aged participants:a selfcontrolled study
- The effect of dexmedetomidine on decrease of cough,hemodynamic parameters and Ramsay score versus lidocaine during general anesthesia:a randomized clinical trial
- The role of nitric oxide in peptic ulcer:a narrative review
- Therapeutic effects of hyperbaric oxygen:integrated review
- A new mechanistic approach for the treatment of chronic neuropathic pain with nitrous oxide integrated from a systems biology narrative review
- Hyperbaric oxygen therapy decreases mortality due to Fournier’s gangrene:a retrospective comparative study