Community-acquired pneumonia complicated by rhabdomyolysis: A clinical analysis of 11 cases
2019-04-25BoZhaoRuiZheng
Bo Zhao, Rui Zheng
Bo Zhao, Rui Zheng, Department of Respiratory Medicine, Shengjing Hospital of China Medical University, Shenyang 110004, Liaoning Province, China
Corresponding author: Rui Zheng, MD, PhD, Doctor, Professor, Teacher, Department of Respiratory Medicine, Shengjing Hospital of China Medical University, No. 36 Sanhao Street,Heping District, Shenyang 110004, Liaoning Province, China. zhengr@sj-hospital.org
Abstract
Key words: Community-acquired pneumonia; Rhabdomyolysis; Exercise; Acute kidney injury
INTRODUCTION
Rhabdomyolysis (RM) is a clinical syndrome caused by various factors that may lead to damage and necrosis of skeletal muscles, destruction of cell membrane integrity,and the release of cell contents into the bloodstream, resulting in acid-base imbalance,electrolyte disorders, myoglobinuria, and even acute renal insufficiency[1]. The causes of RM can be divided into two main categories: Traumatic (e.g., crush injury, surgery,and strenuous exercise) and non-traumatic (e.g., drugs, toxic substances, and infections), with the former being more common[2]. RM caused by infection is uncommon. In addition, RM is often overlooked as symptoms are usually absent in the early disease stage. In clinical practice, community-acquired pneumonia (CAP)can induce mild RM, which can be easily missed during examination. Moreover,available data on RM are mainly from case reports[3]. In the present study, we retrospectively reviewed the clinical characteristics, test parameters, and prognosis of patients with CAP complicated by RM. The results were compared with RM induced by strenuous exercise, a common cause of RM requiring admission. The purpose of this study was to determine the characteristics of RM-related CAP and therefore improve its diagnosis and treatment.
MATERIALS AND METHODS
Study population
A total of 127 patients with RM who were admitted to our hospital between January 2012 and June 2018 were selected, and those with suspected etiologies such as crush injury, surgery, and metabolism-related, drug-related, and autoimmune-related factors were excluded. Patients with non-CAP infections were also excluded. In total,11 patients with CAP-induced RM (pneumonia group) and 48 patients with exerciseinduced RM (exercise group) were included in this study. As there are currently no standardized diagnostic criteria for RM, the following clinical criteria are commonly used: (1) Clinical manifestations, often accompanied by muscle pain, swelling, muscle weakness, and dark brown urine, oliguria, or anuria; (2) Relevant tests show serum creatine kinase (CK) exceeding the upper limit of normal by five times (>1000 U/L),myoglobinemia, or myoglobinuria; and (3) Myocardial lesions, chronic muscle-related diseases, and primary renal disease are excluded[1]. The diagnostic criteria for acute kidney injury (AKI) are rapid deterioration of renal function within 48 h, increase in absolute value of serum creatinine >26.4 μmol/L, or >150% above baseline, or urine output <0.5 mL/(kg· h) for more than 6 h[4]. The diagnostic criteria for CAP and severe CAP are based on the “Guidelines for the Diagnosis and Treatment of Community-Acquired Pneumonia in Adults in China” developed by the Chinese Thoracic Society in 2016, and CAP is scored using the pneumonia severity index(PSI)[5].
Methods
The baseline information, test results, and prognosis of 11 patients with CAP-induced RM and 48 patients with exercise-induced RM were retrospectively reviewed. Patients with CAP were treated with anti-inflammatory and mucolytic agents. All patients were managed with hydration and alkalization, and the intake/output fluid volume and related laboratory parameters were monitored.
Statistical analysis
Statistical analysis was performed using the SPSS 17.0 statistical software (SPSS Inc.,Chicago, IL, USA). Data normality was verified by a one-sample Kolmogorov-Smirnov test (P > 0.05 was considered normal). Data with normal distribution were expressed as average ± SD, and data not normally distributed were expressed as medians (M; P25, P75). Count data were expressed as percentages. The independent sample ttest or rank sum test was used to analyze the differences between two samples of measurement data, and the Chi-square test was used to analyze differences between two samples of count data. Differences with a P value < 0.05 were considered statistically significant.
RESULTS
Baseline characteristics and prognosis
All 11 patients with CAP-induced RM were men aged between 22 and 86 years, with a mean age of 61.27 ± 21.34 years, and they were significantly older than patients with exercise-induced RM. The majority of patients with CAP-induced RM showed symptoms of hyperthermia, with the highest body temperature of 39.7 (38.9, 40.6)°C.The major clinical manifestations were respiratory symptoms including cough,sputum production, and shortness of breath. Many patients also showed symptoms of weakness and reduced urine output, but lacked symptoms typical of RM. Six patients had severe CAP but were not treated with mechanical ventilation, and seven patients had AKI. The incidence of AKI was significantly higher in the exercise group, but no dialysis treatment was administered in either group. The average length of hospitalization was 16.55 ± 11.34 d. Nine patients had good prognosis and two patients died. Compared with the exercise group, the pneumonia group had a longer average length of hospitalization and a poorer prognosis. Deceased patients also had higher PSI scores (Tables 1 and 2).
Comparison of test parameters
The average white blood cell (WBC) count in the pneumonia group was 9.83 ± 3.59 ×109/L, the average C-reactive protein (CRP) level was 153.90 ± 132.93 mg/L, and the average procalcitonin level was 0.285 (0.182, 4.72) μg/L. Three patients were positive for Mycoplasma antibodies. Blood culture and multiple sputum bacterial cultures were carried out for all patients, but no clear etiologic evidence was found. No significant difference in WBC count was found between the two groups at admission. The CRP level in the pneumonia group was significantly higher than that in the exercise group.At the time of admission, the blood pH in the pneumonia group was higher than that in the exercise group, and respiratory alkalosis was a prominent manifestation. Most patients with severe CAP had respiratory failure. The highest CK and myoglobin(Mb) values in the pneumonia group were lower than those in the exercise group, and the time required to reach a peak level was also longer. Upon admission, serum creatinine and blood urea nitrogen were higher, whereas serum potassium level was lower in the pneumonia group than in the exercise group. Most patients with CAPinduced RM had a mild increase in cardiac troponin I (cTnI) at 0.03 (0.06, 0.16) μg/L.In addition, they also showed abnormal renal function, and had elevated levels of aspartate transaminase (AST), alanine aminotransferase (ALT), and lactate dehydrogenase (LDH), but the degree of increase was significantly lower than that in the exercise group. The increase in LDH in both groups was mainly attributable to the increase in LDH5 (Tables 3 and 4).
(2)导管脱落:血液透析过程中诸多管道相互连接,各个通道接口、线结处均容易出现导管脱落,护理人员在透析过程中未及时观察并发现的话则易出现导管滑脱引起出血。
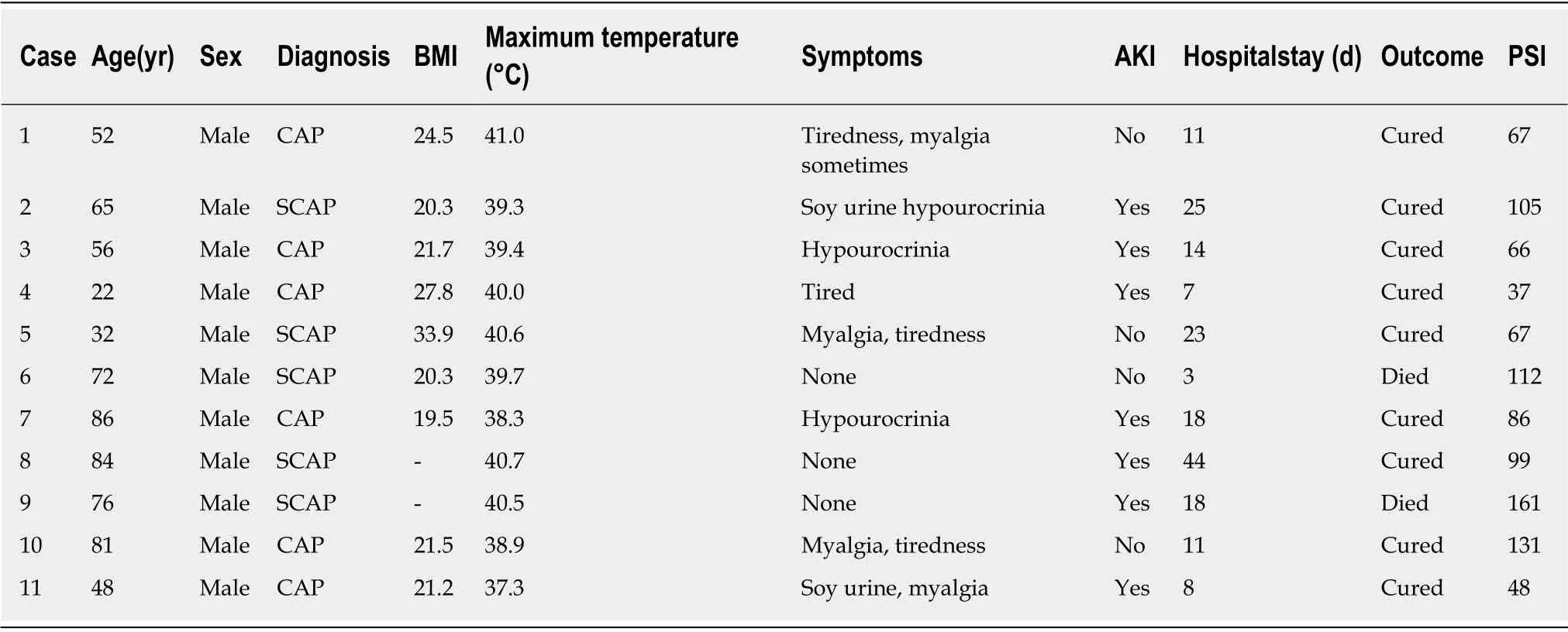
Table 1 Baseline characteristics and prognoses of patients with rhabdomyolysis induced by community-acquired pneumonia
DISCUSSION
RM may be caused by bacterial or viral infections. Although rare, RM is a serious complication that can be life-threatening. The most common site of infection is the respiratory tract[6]. Cases of RM secondary to CAP have been reported, and the main causative organisms are Legionella, Streptococcus pneumoniae, and influenza viruses.There are also reported cases caused by Mycoplasma pneumoniae, Staphylococcus aureus,and tuberculosis. Given the relatively low incidence of CAP-induced RM, there is currently a lack of systematic research and analysis including a large number of cases[6-9]. The mechanism of RM secondary to CAP is still unclear and may be attributable to the following factors: (1) Direct invasion of muscle tissue by pathogenic bacteria, (2) Toxic effects of metabolites from pathogenic bacteria, (3) Cytotoxicity mediated by inflammatory transmitters and necrosis factors, (4) Tissue damage caused by secondary immune response, and (5) Muscle damage caused by high fever,rigors, and hypoxia[10]. In our 11 patients with CAP-induced RM, sputum bacteria,fungi, tuberculosis smears, and cultures were repeated in the hospital. Blood bacterial culture and antibodies for Mycoplasma, Chlamydia and Legionella were also measured.
In this study, three patients were positive for Mycoplasmapneumoniae antibody. Of these, one patient showed symptoms characteristic of Mycoplasma pneumonia, and two patients were considered to have mixed infections. Unfortunately, no other etiologic evidence was identified. In an expert consensus on the diagnosis and treatment of mycoplasma pneumonia in children, RM has been included as a“manifestation of other systems”; however, RM caused by Mycoplasma pneumoniae is relatively uncommon in adults[11]. In addition to the aforementioned pathogenic mechanisms, the P1 and P30 proteins in the attachment organelles of Mycoplasma pneumoniae may show homology with eukaryotic myogenic proteins. Therefore, they may induce autoantibodies in the body that lead to muscle damage through antigenantibody reactions[12].
RM is more common in male patients, probably because they have larger muscle mass as well as other causes that have yet to be elucidated[6]. In this study, the majority of patients with CAP-induced RM were men. Although their mean age was significantly higher than that of patients with exercise-induced RM, it was lower than the age of peak incidence of CAP in adults in China[5]. Young and middle-aged men were considered the high-risk population for CAP-induced RM. The conventional triad of symptoms of RM are muscle pain, weakness, and dark urine[2]. Most patients included in this study showed primary CAP symptoms. All patients had high fever and elevated inflammatory markers such as CRP and procalcitonin, with mild symptoms of muscle pain, weakness, dark urine, and reduced urine output. These symptoms could be explained by infection and fever and were often neglected when acquiring information on medical history. With the exception of significantly darker urine and oliguria in some patients, which alerted the physician to the diagnosis,generally, the possibility of RM was considered only after a significant increase in CK was noted.

Table 2 Comparison of baseline characteristics and prognosis in patients with rhabdomyolysis induced by community-acquired pneumonia and by exercise
Necrosis of skeletal muscle cells can lead to the release of cellular contents into the extracellular fluid and blood circulation, eventually resulting in metabolic acidosis,hyperkalemia, and AKI[8]. In this study, patients in the pneumonia group had a higher incidence of respiratory alkalosis and lower potassium levels compared with patients in the exercise group. Possible reasons for these differences include tachypnea due to fever and hypoxia, low food intake, and sweat loss following the use of antipyretic drugs. After sweating, the patient’s extracellular fluid volume decreases, activating the renin-angiotensin-aldosterone system and promoting potassium excretion. There was a lack of typical RM characteristics such as metabolic acidosis and hyperkalemia.As the most sensitive parameter of muscle injury, CK is directly proportional to the degree of muscle injury, and its value in severe RM can reach ≥ 200 000 U/L[13]. CK begins to rise 2-12 h after muscle injury, reaches a peak in 24-72 h and then returns to normal in approximately 7-10 d. CK is a good marker for monitoring RM[13]. A Spanish group conducted a comparative study in patients with RM caused by infectious and noninfectious causes and found that the CK level in the infectious group was significantly lower than that in the noninfectious group (approximately 1/5 of the latter). Infection-induced RM may cause a lesser degree of skeletal muscle damage compared with RM caused by factors such as exercise, trauma, and drugs[14].Mb is released into the blood when muscle cells are damaged and can obstruct the renal tubules, leading to AKI. Therefore, Mb is an effective marker for predicting AKI[2]. In this study, the CK and Mb levels in the patients with CAP-induced RM were much lower than those in patients with conventional exercise-induced RM. The time to reach the respective peaks was also longer. Therefore, if patients presented during the early stage of the disease, CK and Mb might not have reached their peak levels,resulting in a missed diagnosis. The analyses above indicate that the degree of skeletal muscle damage caused by CAP was lower than that caused by strenuous exercise,and the leakage of potassium ions from cells was not severe. However, the incidence of AKI in patients with CAP-induced RM was higher, and their renal function was worse. In addition to renal tubule obstruction by Mb after muscle damage, this might also be explained by the older age of CAP patients, systemic immune inflammatory response, hyperthermia, hypoxia, and renal toxicity associated with antiinflammatory and antipyretic drugs.
In addition to significant elevations in CK and Mb, the levels of AST, ALT, and LDH can also increase in RM. The increase in LDH in skeletal muscle injury is generally believed to be primarily attributable to the increase in LDH5. The test results in this study essentially confirmed this conclusion[15,16]. However, the increases in the above parameters were significantly lower in the pneumonia group than in the exercise group.
cTnI is considered the “gold standard” for the diagnosis of myocardial injury,particularly for acute myocardial infarction. In this study, seven patients with CAP also had an increase in cTnI. Of these, one patient had rapid atrial fibrillation on admission with a significant increase in cTnI, and the other six patients had no significant electrocardiogram or echocardiography abnormalities. Minor myocardial damage caused by factors such as infection and hypoxia were not excluded. However,related articles and case reports have confirmed that false-positive cTnI may be detected in patients with RM. Troponin I (TnI) includes skeletal troponin I (sTnI) and cTnI. The amino acid sequences of cTnI and sTnI show considerable differences, and their metabolites are excreted by the kidneys[17]. Increased cTnI in RM patients may be caused by cross-immunization to sTnI during testing and decreased excretion due to reduced renal function.
Most patients had a good prognosis after appropriate antibacterial drug and symptomatic treatment, including hydration and alkalization therapies, and via monitoring fluid intake and output, and related laboratory parameters. The alkalization therapy was performed under the strict guidance of nephrologists. Renalfailure easily occurs when the urine pH is less than 6. As long as the urine pH is maintained at approximately 6.5, or even above 7.5, Mb can be filtered from the basement membrane. Therefore, for the treatment of RM, early alkalization of urine can reduce the incidence of renal failure.
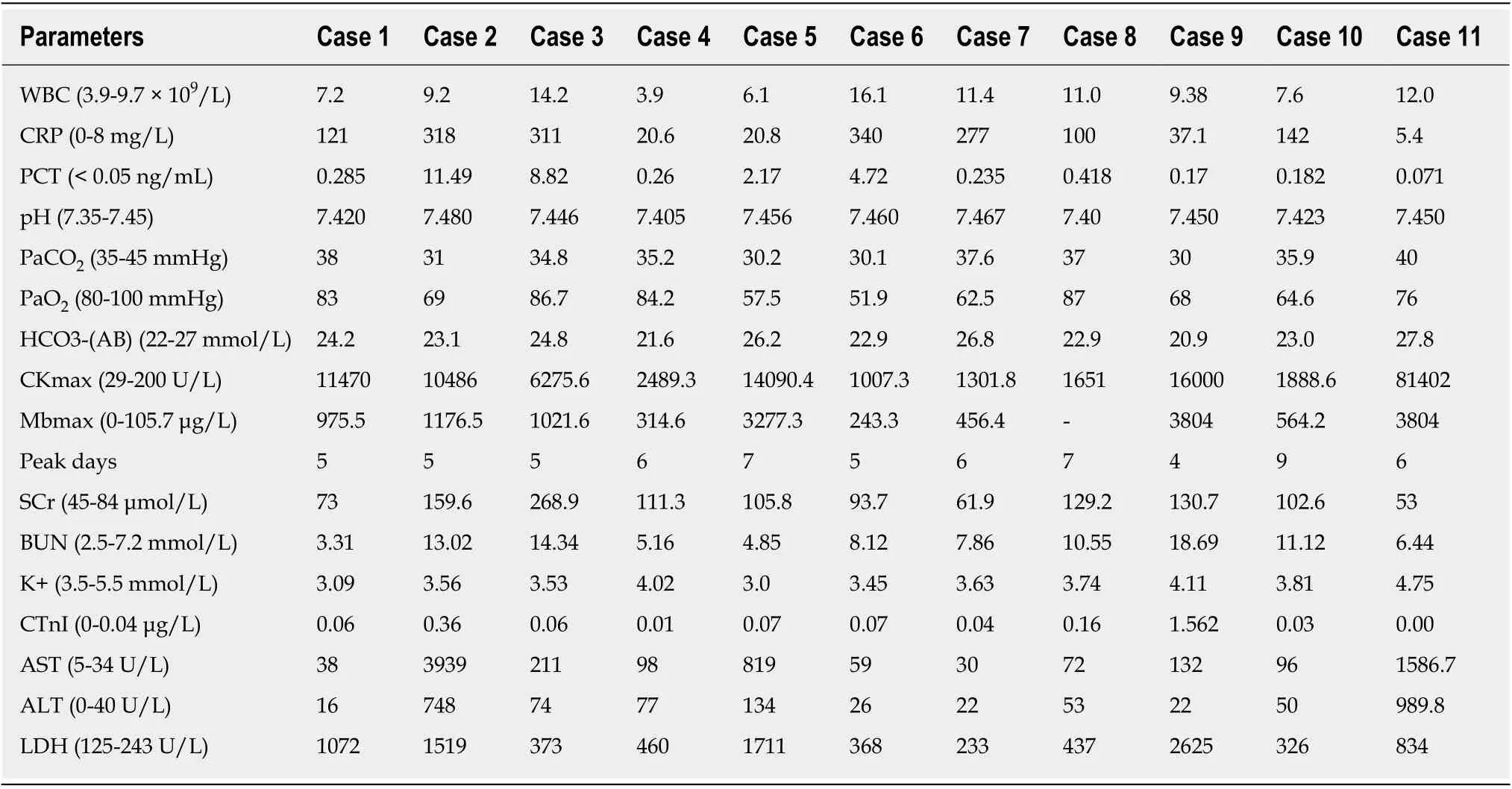
Table 3 Test parameters of patients with rhabdomyolysis induced by community-acquired pneumonia
Given the relatively low incidence of CAP-induced RM, there is currently a lack of systematic research. No standard nephrologic treatment is available for these patients.Nephrologists did not treat these patients differently from RM induced by other causes. Without referring to the pH level during blood gas analysis, urine should be alkalized as soon as possible to avoid deterioration of renal function. According to clinical observations, oxygenation index, and PSI score, the length of hospitalization and adverse events were considered to be mainly related to the severity of pneumonia.
There are some limitations to this study. Although microbiological testing was performed, no definite etiological organisms were detected except for Mycoplasma.The number of patients included in this study was relatively small, and some had undergone initial treatment in other institutions. Fortunately, most patients had been adequately treated with empirical therapy. Due to the efficacy of initial treatment,patients refused further tracheoscopy or puncture biopsy to identify the etiology.Future studies with more rigorous and comprehensive pathogenic detection are required to provide better information regarding treatment and to further elucidate the prevalence and etiology of the disease in our region.
In conclusion, as only a few cases of CAP-induced RM have been reported and the symptoms are atypical, the condition is often overlooked when acquiring information on medical history. If patients present during the early stage of the disease, CK and Mb may not have reached their peak levels. Although there may be abnormalities in hepatic and renal function and cardiac enzymes, the changes are relatively mild and are easily mistaken for damage secondary to infections. All these factors, combined with insufficient knowledge of RM disease, can lead to a missed diagnosis or misdiagnosis. In the present study, a comprehensive analysis was performed on 11 patients with CAP-induced RM who were then compared to patients with exerciseinduced RM. The results indicated that special attention should be paid to the possibility of RM in CAP patients presenting with muscle pain, weakness, dark urine,or reduced urine output, particularly in male patients presenting with fever. For patients with abnormalities in hepatic and renal function and cardiac enzymes, with or without metabolic acidosis and hyperkalemia, CK and Mb should be tested and actively monitored. Early detection and treatment could reduce the occurrence of renal function deterioration and other complications, as well as shorten the treatmentcourse.
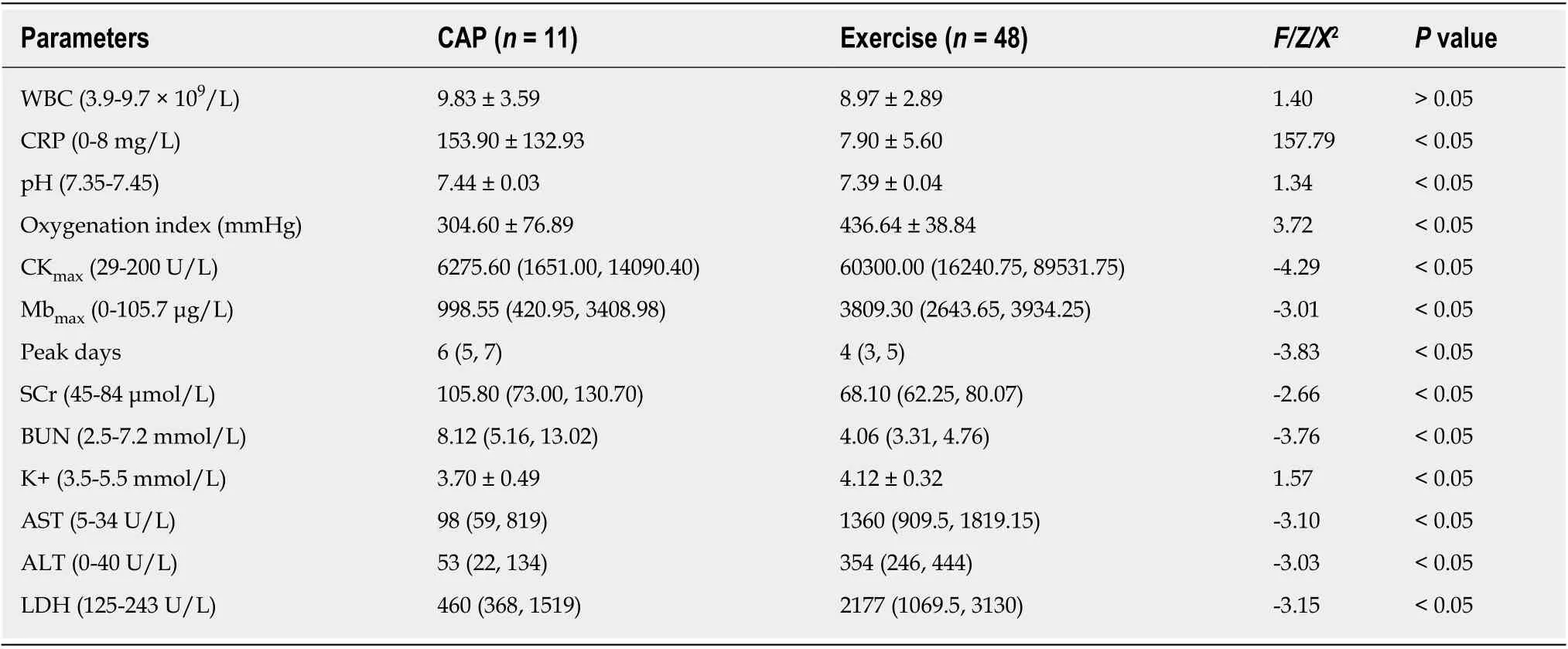
Table 4 Comparison of test parameters in patients with rhabdomyolysis induced by community-acquired pneumonia and by exercise
ARTICLE HIGHLIGHTS
Research background
In clinical practice, rhabdomyolysis (RM) can be caused by community-acquired pneumonia(CAP), which has different clinical characteristics from RM induced by exercise. RM symptoms are mild and can be easily missed during diagnosis. Further studies are needed to determine the characteristics of CAP-induced RM to improve its diagnosis and treatment.
Research motivation
Cases of RM secondary to CAP have been reported, but systematic research data are not available. We believe that some patients with CAP-induced RM have been missed or misdiagnosed due to their atypical symptoms.
Research objectives
This study aimed to investigate the clinical characteristics of patients with CAP-induced RM to avoid missed diagnosis or misdiagnosis.
Research methods
In this retrospective study, baseline information, test results, and prognosis of 11 patients with CAP-induced RM were summarized and compared with those of 48 patients with exerciseinduced RM. Statistical analysis was performed using SPSS 17.0 statistical software.
Research results
CAP-induced RM was more common in men. The major clinical manifestations were high fever and respiratory symptoms, but lacked symptoms typical of RM. Most patients had elevated inflammatory parameters, respiratory alkalosis, and relatively low serum potassium levels and often had abnormalities in hepatic and renal function and cardiac enzymes. Compared with the exercise group, the pneumonia group had substantially lower levels of creatine kinase and myoglobin, a higher incidence of acute kidney injury, and worse renal function and prognosis.Adverse events were mainly related to the severity of CAP.
Research conclusions
CAP can induce RM, which is rare and different from RM induced by exercise. Early detection and treatment could avoid missed diagnosis or misdiagnosis and reduce complications.
Research perspectives
We should pay special attention to the possibility of RM in CAP patients presenting with muscle pain, weakness, dark urine, or reduced urine output, particularly in male patients presenting with fever. For patients with abnormalities in hepatic and renal function and cardiac enzymes,with or without metabolic acidosis and hyperkalemia, creatine kinase and myoglobin should be tested and actively monitored. Early detection and treatment could reduce renal function deterioration and other complications, as well as shorten the treatment course.
猜你喜欢
杂志排行

World Journal of Clinical Cases的其它文章
- Polyunsaturated fatty acids and DNA methylation in colorectal cancer
- lmpact of resection margins on long-term survival after pancreaticoduodenectomy for pancreatic head carcinoma
- Arthroscopy combined with unicondylar knee arthroplasty for treatment of isolated unicompartmental knee arthritis: A long-term comparison
- lntact, pie-crusting and repairing the posterior cruciate ligament in posterior cruciate ligament-retaining total knee arthroplasty: A 5-year follow-up
- Dissection and ligation of the lateral circumflex femoral artery is not necessary when using the direct anterior approach for total hip arthroplasty
- Expression of interleukin-32 in bone marrow of patients with myeloma and its prognostic significance