颈髓损伤患者颈肩部残存肌力与呼吸功能恢复的关系
2017-12-01杨明亮唐丽杨德刚陈亮宫慧明李建军
杨明亮,唐丽,杨德刚,陈亮,宫慧明,李建军
·临床研究·
颈髓损伤患者颈肩部残存肌力与呼吸功能恢复的关系
杨明亮1,2a,唐丽1,2b,杨德刚1,2a,陈亮1,2a,宫慧明1,2a,李建军1,2a
目的 观察颈髓损伤患者颈肩部残存肌力与呼吸功能的相关性。方法 2015年1月至2016年6月,30例创伤性颈髓损伤患者于损伤后5周、24周检查患者胸锁乳突肌、斜方肌、三角肌肌力,进行感觉、运动功能评分,检测肺功能。结果 间断脱机患者三角肌肌力与肺活量在伤后5周、24周呈正相关(r>0.806,p<0.05),感觉评分在伤后5周存在相关性(r=0.914,p<0.01),运动评分(r=0.979,p<0.001)、斜方肌肌力(r=0.894,p<0.01)在伤后24周存在相关性。结论 颈肩部残存肌力,特别是三角肌肌力对颈髓损伤患者呼吸功能有一定影响。
颈髓损伤;肺功能;肌力;三角肌;斜方肌;胸锁乳突肌
颈髓损伤是一种致命的创伤,除导致患者四肢瘫痪外,常累及脊髓内呼吸中枢(膈神经核、C3-5),导致广泛呼吸肌肉瘫痪。在急性期,84%颈髓损伤患者存在呼吸系统并发症,20%患者需要气管切开和机械通气治疗;4%~5%严重颈髓损伤患者需终身使用呼吸机[1-6]。对慢性颈髓损伤,许多患者可因发热、活动增加、情绪焦虑等诱发呼吸困难,出现胸闷不适,严重影响生活质量[7]。能否从神经系统检查结果筛选一些指标,预测患者呼吸功能恢复[8-10]?从神经解剖及临床经验分析,有三对肌肉应予以重点考虑:首先是颈肩部的斜方肌、胸锁乳突肌,它们由副神经支配,对颈髓损伤患者瘫痪的吸气肌肉具有代偿作用[11-12];另一对是三角肌,它与支配膈肌的脊髓节段几乎定位在同一范围,能间接反应膈肌瘫痪程度[9-12]。本研究旨在调查上述三对肌肉残存肌力对颈髓损伤患者呼吸功能的影响。
1 资料与方法
1.1 一般资料
2015年1月至2016年6月,从中国康复研究中心北京博爱医院脊柱脊髓神经功能重建科及ICU筛选创伤性颈髓损伤患者。患者正式纳入前签署书面知情同意,并经中国康复研究中心医学伦理委员会审批。共39例患者纳入研究,其中30例完成随访,脱落原因为出院后失访。完成随访的患者中,男性26例,女性4例;平均年龄(42.4±18.9)岁;完全性损伤16例,不全性损伤14例。
纳入标准:年龄18~60岁间;病程≤6周。
排除标准:存在严重肺部感染、肺不张、胸腔积液、肋骨骨折、脑外伤、慢性阻塞型肺病等。
1.2 呼吸功能评级
依据机械通气依赖程度,吸氧依赖程度,日常生活中是否存在肺功能障碍导致胸闷、气促症状等,将患者分为:呼吸机依赖(A级)、间断脱机(B级)、呼吸功能不全(C级)、自主呼吸(D级)。伤后(5±1)周和(24±2)周,对患者评级。
评级标准:A级,呼吸机维持,或最近1周内尝试脱机,但单次脱机时间不能维持1 h;B级,最近1周内至少有1次脱机,单次脱离呼吸机时间>1 h;C级,自主呼吸,但存在胸闷、气促,低氧血症等,需吸氧缓解,或低强度活动诱发胸闷、气促,需降低活动量缓解症状;最近1周内上述症状至少出现1次;D级,自主呼吸,无肺功能障碍导致的胸闷、气促,低氧血症等。
1.3 颈肩肌肉肌力评估
采用徒手肌力测定评估胸锁乳突肌、斜方肌、三角肌肌力,计算双侧肌力之和。
1.4 神经损伤评估
根据美国脊髓损伤协会(American Spinal Cord Injury Association,ASIA)制订的脊髓损伤分类标准[13-14]评估神经损伤程度及分级。
1.5 肺功能检查
采用Sorinnes-B-5503肺功能检测仪(Medisoft S.A,de Ciney,Belgium)。患者平卧位,测试前解除腹带,佩戴鼻夹,并吹气测试。重复检查2次,间隔3~5 min,取最佳结果。不使用支气管扩张剂,重点评估肺活量[15-17]。
1.6 统计学分析
采用SPSS 19.0统计软件进行分析。计量资料符合正态分布,采用(xˉ±s)表示,分级间比较采用独立样本t检验,相关性检验采用Pearson相关性分析。显著性水平α=0.05。
2 结果
2.1 功能评估
5周时,B级感觉、运动评分,肌力均明显高于A组(p<0.01);C组运动评分、三角肌肌力、肺活量、潮气量均高于B级(p<0.05);D组运动评分、肌力、肺活量均高于C级(p<0.05)。见表1、表2。
与伤后5周相比,伤后24周,B级肺活量提高55%,C级提高50%。见表1。
伤后24周,A级患者2例转为B级,2例转为D级;B级患者4例转为D级;C级患者6例转为D级。这14例患者感觉、运动、肌力评分及肺功能结果见表3。
2.2 感觉、运动、肌力评分与肺功能的相关性
呼吸功能B级患者三角肌肌力与肺活量在伤后5周、24周呈正相关,感觉评分在伤后5周存在相关性,运动评分、斜方肌肌力在伤后24周存在相关性(p<0.05)。呼吸功能C级患者三角肌肌力与肺活量在伤后5周呈正相关(p<0.05)。见表4。各项评估指标与潮气量的相关性不明显。见表5。
将伤后24周呼吸功能改善的10例B级、C级患者单独进行分析,显示B级三角肌肌力、运动评分与肺活量在伤后5周、24周呈正相关,感觉评分在伤后5周相关,斜方肌肌力在伤后24周呈正相关;C级运动评分和三角肌肌力与肺活量在伤后5周呈正相关。见表6。感觉、运动、肌力评分与潮气量的相关性不明显。见表7。

表1 伤后不同时间患者感觉、运动、肌力及肺功能检查结果
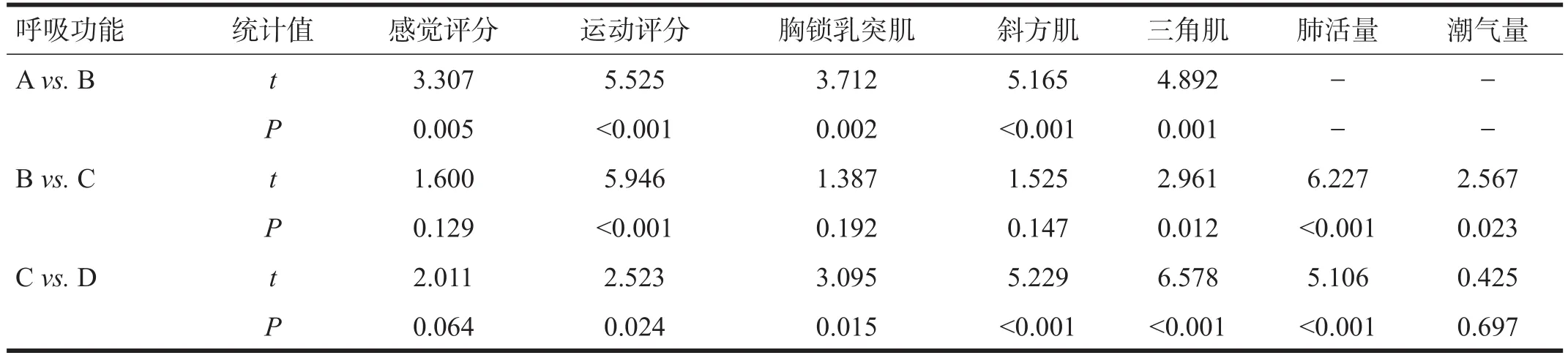
表2 伤后5周患者感觉、运动、肌力及肺功能统计学分析结果

表3 呼吸改善患者伤后不同时间感觉、运动、肌力及肺功能检查结果
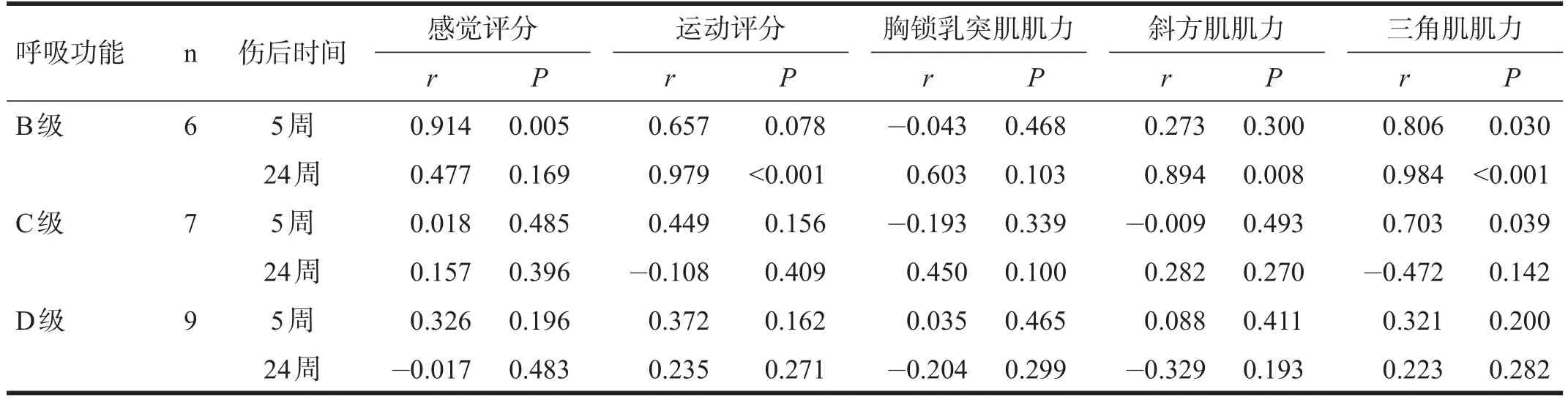
表4 患者感觉、运动、肌力评分与肺活量的相关性分析
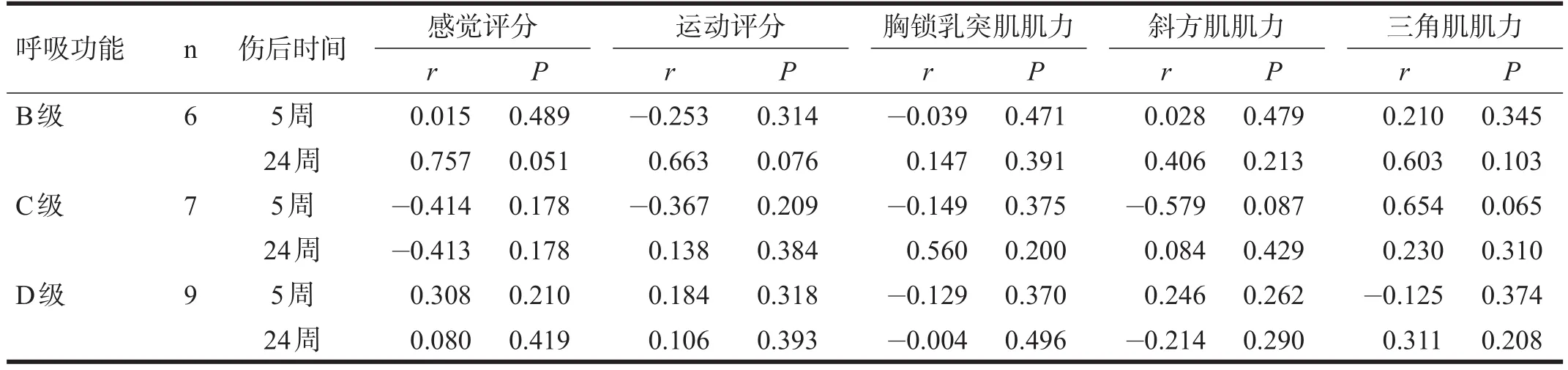
表5 患者感觉、运动、肌力评分与潮气量的相关性分析

表6 呼吸功能改善患者感觉、运动、肌力评分与肺活量的相关性分析

表7 呼吸功能改善患者感觉、运动、肌力评分与潮气量的相关性分析
3 讨论
斜方肌和胸锁乳突肌位于颈肩部,由副神经的脊髓根支配,具有一定的辅助吸气作用[18-20]。对健康人群,其辅助吸气作用并不重要;但在颈髓损伤患者,特别是膈肌严重瘫痪患者,可代偿吸气肌功能[21]。胸锁乳突肌收缩上提胸骨,能恢复部分胸廓活动;斜方肌上提肩胛骨,补偿肋间外肌功能。两组肌肉在呼吸康复中有重要意义[22-23]。临床观察显示,斜方肌、胸锁乳突肌肌力小于Ⅲ级患者,通常需要呼吸机维持生命;斜方肌、胸锁乳突肌肌力大于Ⅲ级患者,通常能间断脱机。本组病例呼吸功能A级患者,双侧斜方肌、胸锁乳突肌肌力分别为(2.6±1.7)、(3.3±2.2);B级患者分别为(6.3±0.5)、(6.8±0.8)。这一结果与临床经验相符。
膈肌位于体腔内,分割胸、腹腔,其活动及肌力无法在直视下用常规的徒手肌力检测方法评估。支配三角肌与膈肌的神经胞体,在脊髓内位于相同节段范围(C3-5),对创伤性颈髓损伤患者,从神经解剖角度分析,似可用三角肌肌力间接评估膈肌损伤程度及预测其恢复。本研究显示,呼吸功能B、C级患者的三角肌残存肌力及恢复与肺活量相关。提示三角肌能间接指示膈肌损伤程度和预测膈肌恢复潜能。
本研究根据患者对机械通气依赖程度、吸氧依赖程度、日常生活中是否存在呼吸功能障碍导致的胸闷、气促症状等,对颈髓损伤患者进行呼吸功能分级。A级患者无自主呼吸,可认为其肺活量、潮气量为0。由A级到D级,患者的呼吸功能障碍由重到轻,各级间肺活量有提高,患者的生活质量也不同。该分级方案对颈髓损伤患者呼吸功能的临床评估有一定指导意义。
总之,颈髓损伤患者,斜方肌、胸锁乳突肌活动能代偿部分胸式呼吸,对膈肌严重瘫痪患者,补偿呼吸功能具有重要意义。三角肌肌力残余及恢复情况可以较好指示膈肌功能及恢复。
[1]Wyndaele M,Wyndaele JJ.Incidence,prevalence and epidemiology of spinal cord injury:What learns a worldwide literature survey?[J].Spinal Cord,2006,44(9):523-529.
[2]Onders RP,Elmo M,Khansarinia S,et al.Complete worldwide operative experience in laparoscopic diaphragm pacing:Results and differences in spinal cord injured patients and amyo-trophic lateral sclerosis patients[J].Surg Endosc,2009,23(7):1433-1440.
[3]Branco BC,Plurad D,Green DJ,et al.Incidence and clinical predictors for tracheostomy after cervical spinal cord injury:A national trauma databank review[J].J Trauma,2011,70(1):111-115.
[4]Burney RE,Maio RF,Maynard F,et al.Incidence,characteristics,and outcome of spinal cord injury at trauma centers in north america[J].Arch Surg,1993,128(5):596-599.
[5]Tester NJ,Fuller DD,Fromm JS,et al.Long-term facilitation of ventilation in humans with chronic spinal cord injury[J].Am J Respir Crit Care Med,2014,189(1):57-65.
[6]Brown R,DiMarco AF,Hoit JD,et al.Respiratory dysfunction and management in spinal cord injury[J].Respir Care,2006,51(8):853-870.
[7]Hagen EM.Acute complications of spinal cord injuries[J].World J Orthop,2015,6(1):17-23.
[8]Wu HT,Zhao CP,Li Z,et al.Value of preventive tracheotomy in patients with acute cervical spinal cord injury[J].Zhonghua Yi Xue Za Zhi,2013,93(47):3762-3765.
[9]Chiodo AE,Scelza W,Forchheimer M.Predictors of ventilator weaning in individuals with high cervical spinal cord injury[J].J Spinal Cord Med,2008,31(1):72-77.
[10]Berney SC,Gordon IR,Opdam HI,et al.A classification and regression tree to assist clinical decision making in airway management for patients with cervical spinal cord injury[J].Spinal Cord,2011,49(2):244-250.
[11]Yang ML,Li JJ,Gao F,et al.A preliminary evaluation of the surgery to reconstruct thoracic breathing in patients with high cervical spinal cord injury[J].Spinal Cord,2014,52(7):564-569.
[12]Terson de Paleville D,Lorenz D.Compensatory muscle activation during forced respiratory tasks in individuals with chronic spinal cord injury[J].Respir Physiol Neurobiol,2015,217(10):54-62.
[13]Committee M,Burns S,Biering-Sorensen F,et al.International standards for neurological classification of spinal cord injury,revised 2011[J].Top Spinal Cord Inj Rehabil,2012,18(1):85-99.
[14]Kirshblum S,Waring W 3rd.Updates for the International Standards for Neurological Classification of Spinal Cord Injury[J].Phys Med Rehabil Clin NAm,2014,25(3):505-517.
[15]Roth EJ,Nussbaum SB,Berkowitz M,et al.Pulmonary function testing in spinal cord injury:Correlation with vital capacity[J].Paraplegia,1995,33(8):454-457.
[16]Biering-Sorensen F,Krassioukov A,Alexander MS,et al.International Spinal Cord Injury Pulmonary Function Basic Data Set[J].Spinal Cord,2012,50(6):418-421.
[17]Zakrasek EC,Nielson JL,Kosarchuk JJ,et al.Pulmonary outcomes following specialized respiratory management for acute cervical spinal cord injury:A retrospective analysis[J].Spinal Cord,2017,55(6):559-565.
[18]Placheta E,Tinhofer I,Schmid M,et al.The spinal accessory nerve for functional muscle innervation in facial reanimation surgery:An anatomical and histomorphometric study[J].Ann Plast Surg,2016,77(6):640-644.
[19]Hamada T,Usami A,Kishi A,et al.Anatomical study of phrenic nerve course in relation to neck dissection[J].Surg RadiolAnatomy,2015,37(3):255-258.
[20]Brinzeu A,Sindou M.Functional anatomy of the accessory nerve studied through intraoperative electrophysiological mapping[J].J Neurosurg,2017,126(3):913-921.
[21]Overland J,Hodge JC,Breik O,et al.Surgical anatomy of the spinal accessory nerve:Review of the literature and case report of a rare anatomical variant[J].J Laryngol Otol,2016,130(10):969-972.
[22]何志伟,赵红梅.脊髓损伤患者肺功能特点及康复综述[J].中国康复理论与实践,2015,21(4):441-444.
[23]李建军,杨明亮,杨德刚,等.创伤性脊柱脊髓损伤评估、治疗与康复专家共识[J].中国康复理论与实践,2017,23(3):274-287.
Correlation between Residual Strength of Neck and Shoulder Muscles and Respiratory Function in Patients with Cervical Spinal Cord Injury
YANG Ming-liang1,2a,TANG Li1,2b,YANG De-gang1,2a,CHEN Liang1,2a,GONG Hui-ming1,2a,LI Jian-jun1,2a
1.Capital Medical University School of Rehabilitation Medicine,Beijing 100068,China;2.a.Department of Spinal and Neural Function Reconstruction;b.Department of Cardiovascular Medicine,Beijing Bo'ai Hospital,China Rehabilitation Research Center,Beijing 100068,China
LI Jian-jun.E-mail:crrclij2010@sohu.com
Objective To investigate the correlation between residual strength of neck and shoulder muscles and respiratory function in patients with cervical spinal cord injury.Methods From January,2015 to June,2016,the muscle strength of sternocleidomastoid,trapezius and deltoid was tested in 30 patients with cervical spinal cord injury five and 24 weeks after injury.Meanwhile,their neurological and pulmonary function was evaluated.Results There was correlation between the vital capacity and muscle strength of deltoid both five and 24 weeks after injury(r>0.806,p<0.05)in the patients intermittent without ventilation,and it was found in sense score five weeks after injury(r=0.914,p<0.01),motor score(r=0.979,p<0.001)and the muscle strength of trapezius(r=0.894,p<0.01)24 weeks after injury.Conclusion The residual strength of neck and shoulder muscles,especially of deltoid,plays an important role in the respiratory function in patients with cervical spinal cord injury.
cervical spinal cord injury;pulmonary function;muscle strength;trapezius;sternocleidomastoid;deltoid
10.3969/j.issn.1006-9771.2017.11.014
R651.2
A
1006-9771(2017)11-1308-05
[本文著录格式] 杨明亮,唐丽,杨德刚,等.颈髓损伤患者颈肩部残存肌力与呼吸功能恢复的关系[J].中国康复理论与实践,2017,23(11):1308-1312.
CITED AS:Yang ML,Tang L,Yang DG,et al.Correlation between residual strength of neck and shoulder muscles and respiratory function in patients with cervical spinal cord injury[J].Zhongguo Kangfu Lilun Yu Shijian,2017,23(11):1308-1312.
1.首都医科大学康复医学院,北京市100068;2.中国康复研究中心北京博爱医院,a.脊柱脊髓神经功能重建科;b.心血管内科,北京市100068。作者简介:杨明亮(1967-),男,汉族,湖南汨罗市人,博士,主任医师,硕士生导师,主要研究方向:脊柱脊髓损伤及并发症的诊断治疗,呼吸功能重建,神经康复。通讯作者:李建军(1962-),男,汉族,山东威海市人,教授,主任医师,博士生导师,主要研究方向:脊柱脊髓损伤临床治疗与康复、康复管理。E-mail:crrclij2010@sohu.com。
2017-05-27
2017-08-24)