结构脂肪乳在高龄胃肠道肿瘤术后患者肠外营养的应用
2015-04-21孙倩美
白 熙,孙倩美
结构脂肪乳在高龄胃肠道肿瘤术后患者肠外营养的应用
白 熙,孙倩美*
(首都医科大学附属北京朝阳医院综合科,北京 100020)
探讨结构脂肪乳在高龄胃肠道肿瘤术后患者肠外营养的应用。选择2012年1月至2014年10月在北京朝阳医院老年病房住院的经病理证实为胃肠道肿瘤的高龄术后患者68例,随机分为结构脂肪乳组(STG组)35例,对照组(MCT/LCT组)33例,分别给予肠外营养支持治疗。监测两组患者营养指标、脂代谢、糖代谢指标、肝酶、胆红素、超敏C反应蛋白(hs-CRP)及免疫指标变化。术前及术后治疗前,两组患者上述指标间差异均无统计学意义(>0.05)。进行6d等氮、等热量肠外营养支持治疗后,两组的TP、ALB、TC及STG组的PAB、MCT/LCT组的LDL-C显著高于治疗前(<0.05)。STG组营养指标显著高于MCT/LCT组同期水平(<0.05);STG组TC、LDL-C显著低于MCT/LCT组同期水平(<0.05)。治疗3d后,STG组hs-CRP较治疗前显著降低(<0.05),且下降程度大于MCT/LCT组(<0.05)。治疗6d后,两组CD3+、CD4+均较治疗前明显升高(<0.05);STG组CD3+、CD4+及CD4+/CD8+比值显著高于MCT/LCT组(<0.05)。治疗后两组糖代谢指标、肝酶、胆红素差异无统计学意义(>0.05)。结构脂肪乳对于胃肠道肿瘤术后高龄老年患者,在促进蛋白合成、维持血脂稳定、改善炎症反应及免疫抑制方面优于常规MCT/LCT,临床应用安全性较高。
老年人;脂肪乳剂,静脉注射用;胃肠外营养;胃肠肿瘤;T淋巴细胞亚群
高龄老人罹患胃肠道肿瘤,营养状况及免疫功能进一步下降。脂肪乳作为肠外营养治疗中的重要组分,参与供能并影响免疫功能。脂肪乳包括:长链甘油三酯(long-chain triglycerides,LCT)及中链甘油三酯(medium-chain triglycerides,MCT)。由于二者配比不同,临床存在不同剂型。本研究旨在探讨结构脂肪乳(结构甘油三酯,structured triglycerides,STG)与物理混合的脂肪乳剂(MCT/LCT)对高龄老年胃肠道肿瘤术后患者治疗效果的影响,为临床制定合理的营养治疗方案提供依据。
1 对象与方法
1.1 研究对象
选择2012年1月至2014年10月在北京朝阳医院老年病房住院的经病理证实为胃肠道肿瘤的高龄术后患者68例。其中男性45例,女性23例;年龄75~96(81.5±10.3)岁;食管癌10例,胃癌21例,结肠癌24例,直肠癌13例。将患者随机分为两组,即STG组35例,MCT/LCT组33例。分别接受STG和MCT/LCT肠外营养支持治疗。两组患者在性别、年龄、体质量指数、肿瘤部位、组织学分型均具有可比性(>0.05;表1)。
排除标准:(1)合并脂质代谢异常;(2)合并糖尿病或其他代谢性疾病(甲状腺功能亢进、甲状腺功能减退、肾上腺皮质功能异常);(3)合并急性感染;(4)心、肺、肝功能衰竭;(5)肌酐清除率<50ml/min。
1.2 营养支持治疗
两组患者于术后第1天开始,连续6d接受等氮、等热量的肠外营养治疗。非蛋白热卡为20kCa/(kg·d)[83.6kJ/(kg·d)],由葡萄糖和脂肪乳提供,糖脂热量比约为1∶1。脂肪(甘油三酯,三酰甘油,triglycerides,TG)为1.0g/(kg·d)。STG组为20%结构脂肪乳注射液(250ml/瓶,其中LCT占64%,MCT占36%);MCT/LCT组为20%中/长链脂肪乳剂(250ml/瓶,其中LCT占50%,MCT占50%)。氮量为0.15g/(kg·d),氮源均为复方氨基酸注射液(8.5%乐凡命)。非蛋白质热卡(kCa)与氮量(g)比值为133∶1。以“全静脉混合液”形式通过周围静脉或中心静脉输注,输注时间为15~18h/d,周期为术后第1天至第6天。术后第1天输入1/2的营养需要量,第2天开始为全量。
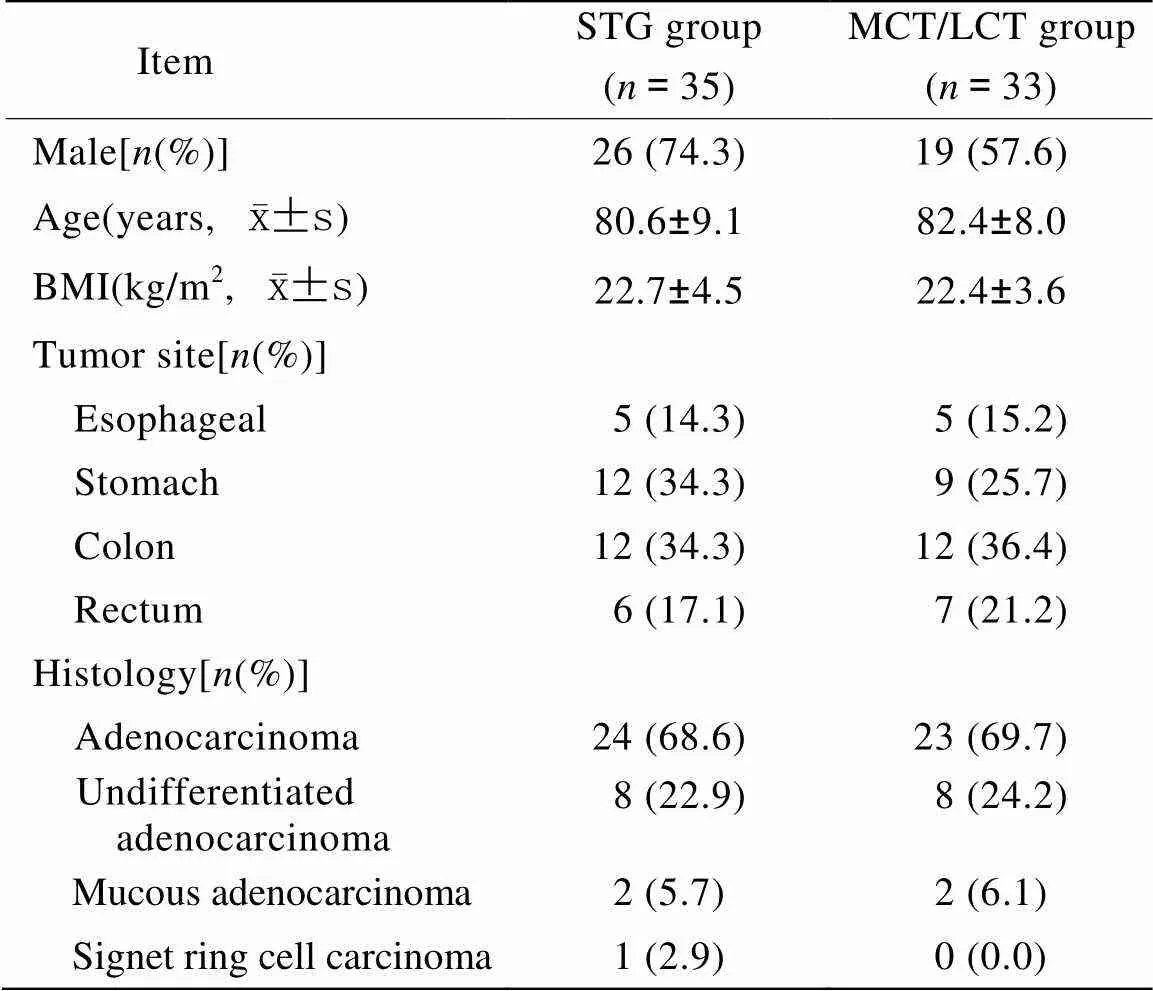
表1 两组患者临床资料比较
STG: structured triglycerides; MCT: medium-chain triglycerides; LCT: long-chain triglycerides; BMI: body mass index
1.3 监测指标
两组患者均在术前、术后第1天营养治疗前、治疗3d后、治疗6d后采集空腹外周静脉血进行标本测定。营养指标:血清总蛋白(total protein,TP)、白蛋白(albumin,ALB)、前白蛋白(pre-albumin,PAB);脂代谢指标:总胆固醇(total cholesterol,TC)、高密度脂蛋白胆固醇(high-density lipoprotein cholesterol,HDL-C)、低密度脂蛋白胆固醇(low-density lipoprotein cholesterol,LDL-C)、TG;糖代谢指标:空腹血糖(fasting blood glucose,FBG)、餐后2h血糖(2-hour postprandial blood glucose,2hPBG);肝功能指标:丙氨酸氨基转移酶(alanine aminotransferase,ALT)、天门冬氨酸氨基转移酶(aspartate transaminase,AST)、γ−谷氨酰转肽酶(γ-glutamyl-transferase,γ-GT)、总胆红素(total bilirubin,TBIL)、直接胆红素(direct bilirubin,DBIL);炎性反应指标:超敏C反应蛋白(high sensitivity C-reactive protein,hs-CRP);细胞免疫指标:CD3+、CD4+、CD8+比率及CD4+/CD8+比值。
1.4 统计学处理

2 结 果
2.1 营养指标
术前及术后治疗前两组营养指标间比较差异无统计学意义(>0.05)。与术前比较,术后治疗前两组均出现蛋白水平明显下降(<0.05)。营养治疗3d后蛋白质水平仍未恢复至术前水平。营养治疗6d后,两组蛋白质水平均恢复至术前水平,且STG组TP、ALB、PAB及MCT/LCT组TP、ALB均显著高于治疗前(<0.05)。两组间比较,营养治疗6d后STG组TP、ALB、PAB显著高于MCT/LCT组同期指标(<0.05;表2)。
2.2 脂代谢指标
术前及术后治疗前两组脂代谢指标间比较差异无统计学意义(>0.05)。营养治疗6d后,STG组TC、MCT/LCT组TC、LDL-C显著高于治疗前(<0.05);STG组TC、LDL-C低于MCT/LCT组同期水平,两组间比较差异有统计学意义(<0.05)。两组同期TG水平间比较差异无统计学意义(>0.05;表3)。
2.3 糖代谢指标及肝酶、胆红素变化
两组FBG、2hPBG、ALT、AST、γ-GT、TBIL、DBIL治疗前后比较差异无统计学意义(>0.05);组间同期水平比较差异亦无统计学意义(>0.05)。
2.4 炎性反应指标hs-CRP
术前两组间hs-CRP比较差异无统计学意义(>0.05)。术后治疗前两组hs-CRP水平均较术前明显升高(<0.05)。营养治疗3d后,两组hs-CRP水平均较治疗前下降,STG组较治疗前显著降低(<0.05),且下降程度大于MCT/LCT组(<0.05)。营养治疗6d后,两组hs-CRP水平进一步下降,但仍未降至术前水平,两组间比较差异无统计学意义(>0.05;表4)。
2.5 免疫指标
两组术前细胞免疫指标比较差异无统计学意义(>0.05)。术后治疗前两组CD3+、CD4+、CD8+、CD4+/CD8+较术前均有不同程度下降(<0.05)。此后逐渐回升,治疗6d后两组CD3+、CD4+均较治疗前明显升高(<0.05);STG组CD3+、CD4+比率及CD4+/CD8+比值显著高于MCT/LCT组,两组间比较差异有统计学意义(<0.05;表5)。

表2 两组治疗前后营养指标比较
STG: structured triglycerides; MCT: medium-chain triglycerides; LCT: long-chain triglycerides; TP: total protein; ALB: albumin; PAB: pre-albumin. Compared with before the treatment in the same group,*<0.05; compared with group MCT/LCT at the same time point,#<0.05; compared with before the operation in the same group,△<0.05
表3 两组治疗前后脂代谢指标比较
STG: structured triglycerides; MCT: medium-chain triglycerides; LCT: long-chain triglycerides; TC: total cholesterol; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; TG; triglycerides. Compared with before the treatment in the same group,*<0.05; compared with group MCT/LCT at the same time point,#<0.05
表4 两组治疗前后hs-CRP比较
STG: structured triglycerides; MCT: medium-chain triglycerides; LCT: long-chain triglycerides; hs-CRP: high sensitivity C-reactive protein. Compared with before the treatment in the same group,*<0.05; compared with group MCT/LCT at the same time point,#<0.05; compared with before the operation in the same group,△<0.05
表5 两组治疗前后免疫指标比较
STG: structured triglycerides; MCT: medium-chain triglycerides; LCT: long-chain triglycerides. Compared with before the treatment in the same group,*<0.05; compared with group MCT/LCT at the same time point,#<0.05; compared with before the operation in the same group,△<0.05
3 讨 论
ALB和PAB均在肝合成,是反映机体蛋白质代谢水平的客观指标。它们的半衰期分别为20d和2~3d,因此PAB在判断蛋白质急性变化方面较ALB更为敏感,是评价营养状态的灵敏指标[1]。本试验中,营养支持6d后,STG组TP、ALB、PAB均显著高于MCT/LCT组,可能与血浆的脂蛋白脂酶活性较高,STG在体内水解较快、氧化完全、供能更加迅速有关。提示STG在蛋白质代谢方面较MCT/LCT脂肪乳剂具有更积极的影响。
脂肪乳在提供能量的同时还提供必需脂肪酸[2],并且,脂质参与细胞膜的结构、功能以及炎症和免疫调节等[3,4],从而成为肠外营养不可缺少的组分。脂肪乳包括LCT脂肪乳剂和MCT脂肪乳剂。LCT脂肪乳剂可为机体提供能量和必需脂肪酸;MCT脂肪乳剂在体内具有水解氧化快、代谢不需要肉毒碱参与及对免疫系统影响小等优点。但由于MCT不含必需脂肪酸,所以常使用物理混合MCT/LCT脂肪乳剂[5,6]。人体对物理混合MCT/LCT的代谢实际上是对MCT与LCT两种脂肪乳的分别代谢,因此体内存在两者代谢的彼此干扰。当MCT水解完成后会抢占水解酶,使LCT的水解过程变慢,造成血清中TC、LDL-C浓度持续处于较高状态[7]。
STG是将中链脂肪酸与长链脂肪酸混合、加热、并在酶的催化下在同一甘油骨架上进行结构重组而成,在此过程中TG中的脂肪酸以随机方式进行结构的再酯化,理论上可避免MCT与LCT两种脂肪乳代谢的相互干扰,减少肝负担和脂肪酸堆积[8]。本试验应用STG营养治疗6d后TC、LDL-C显著低于MCT/LCT组,与STG的水解过程较为平稳均匀、代谢更快有关。证实STG脂肪廓清速度优于MCT/LCT脂肪乳剂。与相关研究结果相符[9.10]。
本试验,两组患者在治疗后糖代谢指标、肝酶、胆红素差异无统计学意义,表明脂肪乳剂对糖代谢及肝功无不良影响。与其他相关研究结果相符[11]。
目前广泛应用的中长链脂肪乳为物理混合制剂,其中富含多不饱和脂肪酸(约占60%),易受自由基攻击产生链式反应,引发脂质过氧化,并形成脂质过氧化物,对机体产生过氧化损伤,进一步通过对线粒体膜蛋白和DNA的作用,导致线粒体损伤和氧化磷酸化功能障碍,引发能量代谢紊乱,加重机体应激状态[12]。在STG中多不饱和脂肪酸仅为38%。其结构特点决定了它能以等速释放长链脂肪酸和中链脂肪酸入血[13,14]。在本研究中,术后两组患者hs-CRP较术前明显升高,说明手术创伤对机体产生了明显的急性炎性反应。营养治疗3d后,STG组患者hs-CRP水平显著降低,且明显低于MCT/LCT组,表明STG对机体造成的应激反应影响较小。
一些临床和实验研究提示,输注脂肪乳剂有损于机体的免疫功能,并增加感染的危险性,其机制主要与脂肪酸有关[15]。脂肪酸的改变可影响这些免疫调节因子的产量和活性[16]。T淋巴细胞亚群中CD3+代表细胞免疫的总体水平,CD3+减少表示机体细胞免疫功能总体减弱;CD4+为辅助T细胞,辅助B细胞分化产生抗体,分泌淋巴因子激活其他细胞产生炎性反应,并介导其作用;CD8+为免疫抑制细胞,辅助其他免疫细胞的功能,抑制抗体的合成分泌及T细胞增殖。本研究结果显示,两组术后治疗前CD3+、CD4+、CD8+均有不同程度下降,此后均逐步回升,治疗6d后STG组CD3+、CD4+较MCT/LCT组明显升高,CD4+/CD8+亦明显高于MCT/LCT组,提示STG对机体细胞免疫功能影响相对小。结合此时STG组hs-CRP较MCT/LCT组下降显著,证实炎性反应的减轻伴随着免疫功能的恢复。
总之,本试验可见,与传统的MCT/LCT相比,STG对于胃肠道肿瘤术后高龄老年患者在促进蛋白合成、维持血脂稳定、改善手术应激导致的炎症反应及免疫抑制方面优于常规MCT/LCT,对糖代谢、肝酶、胆红素代谢影响不大,临床应用具有一定优势,安全性较高。
[1] Bae HJ, Lee HJ, Han DS,. Preallbumin levels as a useful marker for predicting infectious complications after gastric surgery[J]. Gastrointest Surg, 2011, 15(12): 2136−2144.
[2] Zhou KG, He GZ, Zhang R,. Effects of lymphatic drainage and ω-3 polyunsaturated fatty acids on intestinal ischemia-reperfusion injury in rats[J]. Natl Med J China, 2011, 91(25): 1775−1779. [周开国, 何桂珍, 张 睿, 等. 淋巴引流及ω-3多不饱和脂肪酸干预对大鼠肠道缺血再灌注的影响[J]. 中华医学杂志, 201l, 91(25): 1775−1779.]
[3] Bai XP, Li HL, Yang WY,. Effects of fenofibrate on the expression of peroxisome proliferator-activated-gamma coactivator-lα in skeletal muscle of rats infused with intralidis[J]. Natl Med J China, 2010, 90(40): 2856−2859. [白秀平, 李宏亮, 杨文英, 等. 非诺贝特对胰岛素抵抗大鼠肌肉过氧化物酶体增殖物激活受体γ协同刺激因子lα基因表达的影响[J]. 中华医学杂志, 2010, 90(40): 2856−2859.]
[4] Furuhashi M, Ishimura S, Ota H,. Lipid chaperones and metabolic inflammation[J]. Int J lnflam, 2011, 2011: 642612.
[5] Lyu QQ, Tong SL. Effect of structured lipid emulsion on acute inflammatory reaction and immunologic function in gastrointestinal cancer patients after operation[J]. Mod J Integr Tradit Chin West Med, 2014, 23(9): 923−925. [吕清泉, 童仕伦. 结构脂肪乳对消化道肿瘤术后患者急性炎性反应和免疫功能的影响[J]. 现代中西医结合杂志, 2014, 23(9): 923−925.]
[6] Su MS, He L, Liu ZW,. Applied studies of structured triglyceride for parenteral nutrition in severe hemorrhagic shock patients after resuscitation[J]. Natl Med J China, 2012, 92(12): 827−830. [苏茂生, 何 蕾, 刘志伟, 等. 结构脂肪乳在严重出血性休克复苏后患者肠外营养的应用[J]. 中华医学杂志, 2012, 92(12): 827−830.]
[7] Wang XY, Li N, Tan L,. The effect of structolipid and physical mixed MCT/LCT on plasma lipid metabolism of patients after abdominal operation[J]. Parenter Enteral Nutr, 2006, 13(4): 209−211. [王新颖, 李 宁, 谭 力, 等. 结构脂肪乳剂对腹部中等手术后病人脂肪代谢的影响[J]. 肠外与肠内营养, 2006, 13(4): 209−211.]
[8] Cao YQ, Feng WM. Application of structured triglyceride in alleviative treatment of malignant obstructive jaundice[J]. Parenter Enteral Nutr, 2014, 21(2): 87−90. [曹亚琴, 冯文明. 结构脂肪乳在恶性梗阻性黄疸病人姑息治疗中的应用[J]. 肠外与肠内营养, 2014, 21(2): 87−90.]
[9] Wanten GJ, Calder PC.Immune modulation by parenteral lipid emulsions[J]. Am J Clin Nutr, 2007, 85(5): 1171−1184.
[10] Puiggros C, Sanchez J, Chacon P,. Evolution of lipid, profile, liver function, and pattern of plasma fatty acids according to the type lipid emulsion administered in parenteral nutrition in the early postoperative period after digestive surgery[J]. JPEN J Parenter Enteral Nutr, 2009, 33(5): 501−512.
[11] Tipoe GL, Lau TY, Nanji AA,. Expression and functions of vasoactive substances regulated by hypoxia-inducible factor-1 in chronic hypoxemia[J]. Cardiovasc Hematol Agents Med Chem, 2006, 4(3): 199−218.
[12] Lin HG, Li N. Application progress in lipid emulsions[J]. Parenter Enteral Nutr, 2011, 18(4): 244−246. [林海冠, 李 宁. 静脉用脂肪乳剂的应用进展[J]. 肠外与肠内营养, 2011, 18(4): 244−246.]
[13] Tang Y, Wu XS, Zhang DW,. The comparative study of structured triglyceride and physical mixed MCT/LCT on fatty acid metabolism in healthy subjects[J]. Parenter Enteral Nutr, 2011, 18(4): 196−199. [唐 云, 武现生, 张大伟, 等. 结构脂肪乳剂与物理混合的中/长链脂肪乳剂脂肪酸代谢比较研究[J]. 肠外与肠内营养, 2011, 18(4): 196−199.]
[14] Bi XL, Sui SR, Sui ZG. The effect of structoglyceride on resting energy expenditure lipid peroxidation in patients with gastrointestinal neoplasm[J]. Parenter Enteral Nutr, 2013, 20(1): 4−7. [毕晓林, 隋善儒, 隋忠国. 结构脂肪乳剂对胃肠肿瘤病人静息能量代谢和脂质过氧化的影响[J]. 肠外与肠内营养, 2013, 20(1): 4−7.]
[15] Chambrier C, Lauverjat M, Bouletreau P.Structured triglyceride emulsions in parenteral nutrition[J].Nutr Clin Pract, 2006, 21(4): 342−350.
[16] Socha P, Koletzko B, Demmelmair H,. Short-term effects of parenteral nutrition of cholestatic infants with lipid emulsions based on medium-chain and long-chain triacylglycerols[J]. Nutrition, 2007, 23(2): 121−126.
(编辑: 周宇红)
Application of structured triglycerides for parenteral nutrition in elderly patients after gastrointestinal tumor surgery
BAI Xi, SUN Qian-Mei*
(Department of General Medicine, Beijing Chaoyang Hospital, Capital Medical University, Beijing 100020, China)
To determine the efficiency of structured triglycerides [STG, with the ratio of medium-chain triglycerides to long-chain triglycerides (MCT/LCT) accounting for 36% to 64%] for total parenteral nutrition (TPN) in the elderly patients with gastrointestinal (GI) tumor operation.Sixty-eight elderly pathologically-identified GI tumor patients undergoing surgical treatment and then being admitted to the Department of Geriatrics of our hospitalfrom January 2012 to October 2014 were recruited in this study. The cohort was randomly divided into 2 groups, STG group (=35) and MCT/LCT group (the ratio accounting for 50% to 50%,=33). They were all given TPN for 6 d after their operations. The parameters of nutrition, lipid metabolism, glucose metabolism, liver enzymes, bilirubin, high sensitivity C-reactive protein (hs-CRP) and immunologic profiles at baseline and 3 and 6d after treatment were measured and recorded respectively.There was no significant difference in the above-mentioned parameters between the 2 groups before and immediately after surgery. The levels of total protein (TP), albumin (ALB) and total cholesterol (TC) in the both groups, that of prealbumin (PAB) in the STG group, and that of low-density lipoprotein-cholesterol (LDL-C) in the MCT/LCT group were significantly increased after 6 days’ isonitrogen isocaloric nutritional support (<0.05). The nutritional parameters were significantly higher in the STG group than in the MCT/LCT group at the same time points (<0.05), but the levels of TC and LDL-C were remarkably lower in the former than in the latter. At 3d after treatment, the level of hs-CRP was reduced significantly in STG group compared to that of before treatment (<0.05), and the reduction was greater than that in the MCT/LCT group (<0.05). The CD3+and CD4+cell counts were increased significantly than before treatment in both groups (<0.05), but the counts of CD3+and CD4+cells and the ratio of CD4+/CD8+were much higher in the STG group than in the partner one (<0.05). No statistical difference was seen in glucose levels, liver function and bilirubin level between the 2 groups after treatment (>0.05).STG is superior to the conventional MCT/LCT in promoting protein synthesis, stabilizing lipid profiles, ameliorating the inflammatory reaction, as well as regulating the immune system, for TPN in the elderly patients after GI tumor operation, and also has higher safety in clinical application.
aged; fat emulsions, intravenous; parenteral nutrition; gastrointestinal neoplasms; T lymphocyte subsets
R592; R735
A
10.11915/j.issn.1671-5403.2015.06.102
2015−02−28;
2015−05−04
孙倩美,E-mail: Sunqianmei5825@163.com
