改良Geneva量表及其联合血浆D−二聚体对老年肺栓塞诊断价值的探讨
2015-04-21胡京敏郭丹杰
胡京敏,赵 灿,郭丹杰
改良Geneva量表及其联合血浆D−二聚体对老年肺栓塞诊断价值的探讨
胡京敏,赵 灿,郭丹杰*
(北京大学人民医院心脏中心,北京 100044)
评价改良Geneva量表及其联合血浆D−二聚体对老年患者肺栓塞(PE)的快速床旁诊断及排除价值。2009年1月至2014年4月在北京大学人民医院因胸痛、呼吸困难等症状被疑诊PE的患者276例,分为老年组(≥60岁)和非老年组(<60岁),以CT肺动脉造影(CTPA)为确诊金标准。按照改良Geneva量表分为PE低度可能性、中度可能性及高度可能性,同时检测血浆D−二聚体。分析两组患者临床特征,比较改良Geneva量表、血浆D−二聚体、改良Geneva量表联合血浆D−二聚体在两组患者中的诊断及排除诊断价值,其诊断预测价值用受试者工作特征(ROC)曲线下面积(AUC)进行评价。276例疑诊PE患者,经CTPA确诊PE 80例(≥60岁52例,<60岁28例)。运用ROC曲线评价改良Geneva量表对PE的诊断价值,老年组与非老年组AUC分别为0.974(95% CI:0.940~0.992),0.981(95% CI:0.924~0.998),差异有统计学意义(<0.001)。老年组血浆D−二聚体、改良Geneva量表联合血浆D−二聚体诊断PE的阴性预测值分别为93.8%,100.0%;非老年组分别为88.9%,100.0%。老年PE患者临床特征不典型;改良Geneva量表对老年PE患者的诊断价值低于非老年患者;对于老年及非老年疑诊PE患者,改良Geneva量表联合血浆D−二聚体均可安全排除PE,其价值优于单独检测血浆D−二聚体。
老年人;肺栓塞;改良Geneva量表;血浆D−二聚体
肺栓塞(pulmonary embolism,PE),为内源性或外源性栓子堵塞肺动脉或其分支引起肺循环障碍的临床病理生理综合征,包括肺血栓栓塞(pulmonary thromboembolism,PTE)、脂肪栓塞、羊水栓塞、空气栓塞等。PTE为PE最常见类型,占PE中的绝大多数,通常所称的PE即指PTE。PE临床表现无特异性[1],未经治疗的PE,死亡率高达30%[2],早期诊断及治疗能降低PE的死亡率[3],其临床表现无特异性,易漏诊误诊,老年患者因合并心肺疾病引起误诊率和漏诊率增高[4−6]。改良Geneva量表[7]是经过验证的准确诊断PE的重要方法,但该量表在我国老年患者的研究尚少。血浆D−二聚体<500μg/L常被用来作为PE的排除标准,本研究旨在明确老年可疑PE患者,改良Geneva量表诊断PE及其联合血浆D−二聚体快速床旁排除PE诊断的价值。
1 对象与方法
1.1 对象
2009年1月至2014年4月在北京大学人民医院因胸痛、呼吸困难等症状被疑诊PE的患者276例。其中老年组(≥60岁)187例,男性99例,女性88例,年龄60~93(75.2±7.4)岁;非老年组(<60岁)89例,男性52例,女性37例,年龄18~59(44.9±10.7)岁。
1.2 方法
1.2.1 研究对象 所有可疑PE患者记录性别、年龄、主要症状(突发呼吸困难、胸痛、咯血、晕厥、单侧下肢疼痛)和体征(心率、呼吸频率、单侧下肢水肿或深压痛)、危险因素(既往深静脉血栓、既往PE、恶性肿瘤、4周内骨折、4周内制动或手术)。应用改良Geneva量表对疑诊PE患者进行评分[8],0~3分为低度可能,4~10分为中度可能,≥11分为高度可能(表1)。
1.2.2 CT肺动脉造影(computed tomography pulmonary arteriography,CTPA) 应用美国GE Healthcare 64排探测器螺旋CT(lightspeed VCT)扫描。CTPA扫描参数为:120kV、300mA,准直器宽度20mm,球管旋转1周0.5s,图像矩阵为512×512。在GE AW4.2工作站中以1.25mm层厚,1mm间隔按标准方法重建后分析CTPA图像。
1.2.3 血浆D−二聚体检测 入院24h内抽血,采用免疫比浊法测定血浆D−二聚体水平,以≥500μg/L为阳性,<500μg/L为阴性。
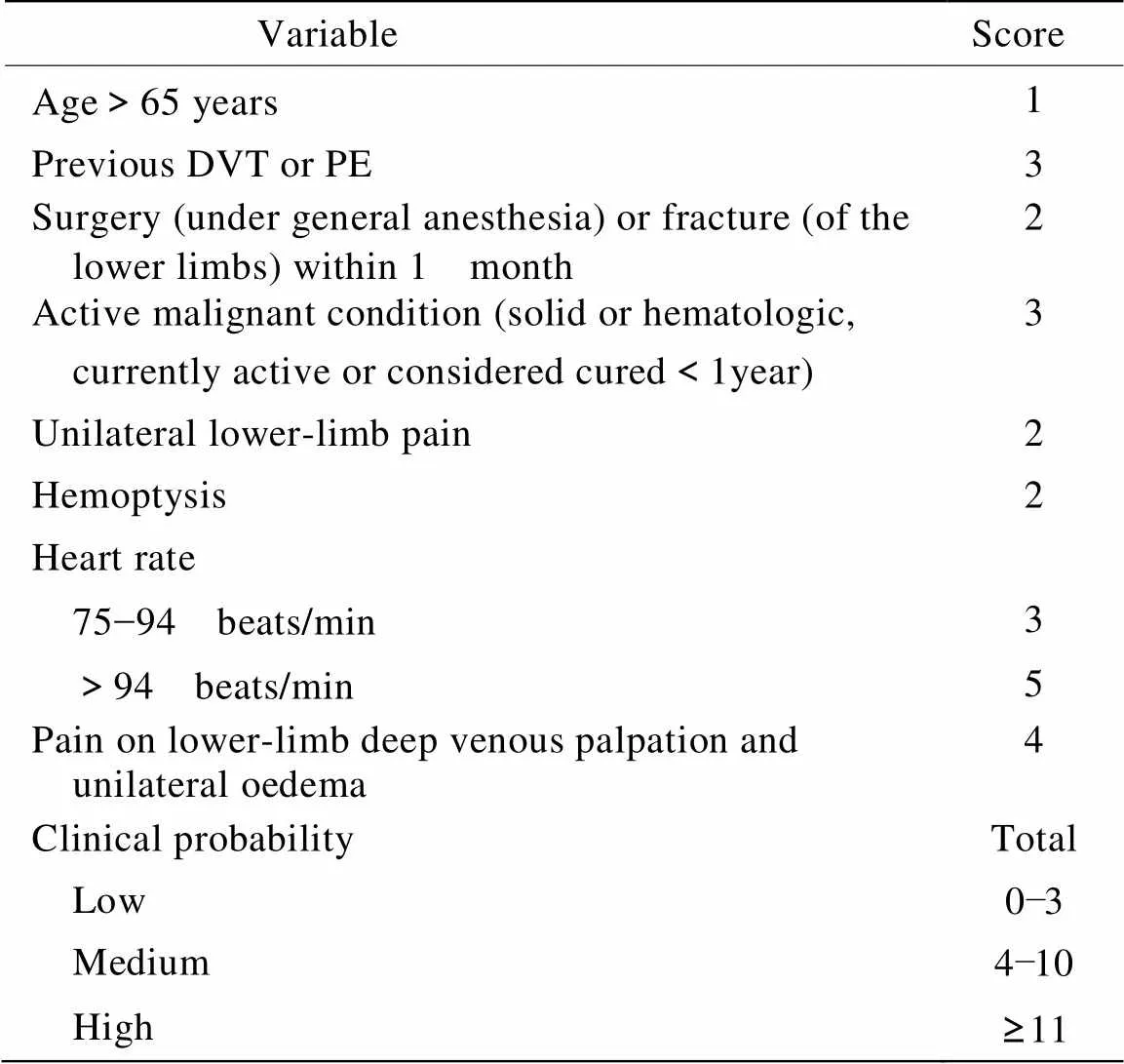
表1 改良Geneva量表
DVT: deep vein thrombosis; PE: pulmonary embolism
1.3 统计学处理
2 结 果
2.1 老年组和非老年组PE患者的临床特征比较
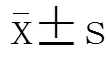
276例疑诊PE患者,最终经CTPA确诊PE 80例,其中老年组52例(65.1%),非老年组28例(34.9%)。对80例确诊的PE患者临床特征进行分析,表2结果显示,老年PE患者呼吸困难发生率高于非老年患者(=0.001);胸痛、咯血、单侧下肢疼痛发生率低于非老年患者(=0.008;=0.018;=0.002);老年PE患者呼吸频率较非老年患者有增高趋势,但差异无统计学意义(>0.05);老年PE患者心率低于非老年患者,差异亦无统计学意义(>0.05);动脉血氧饱和度低于非老年患者(=0.028);其余指标差异均无统计学意义(>0.05),提示老年PE患者症状缺乏特异性。
2.2 Geneva量表对老年患者PE的诊断价值
以CTPA为诊断PE的金标准,用改良Geneva量表对疑诊PE患者进行评分,比较其对老年组和非老年组PE的诊断价值。老年组经改良Geneva量表评估为“高度可能PE”的3例患者中经CTPA确诊2例,误诊率为33.3%(1/3);61例“低度可能PE”患者中仍有15例经CTPA确诊为PE,漏诊率为24.6%(15/61)。非老年组“高度可能PE”的9例患者中经CTPA确诊7例,误诊率为22.2%(2/9);35例“低度可能PE”患者中经CTPA确诊7例,漏诊率为20.0%(7/35)。经统计学分析,仅通过改良Geneva量表诊断老年PE的价值与非老年患者相似(>0.05;表3)。
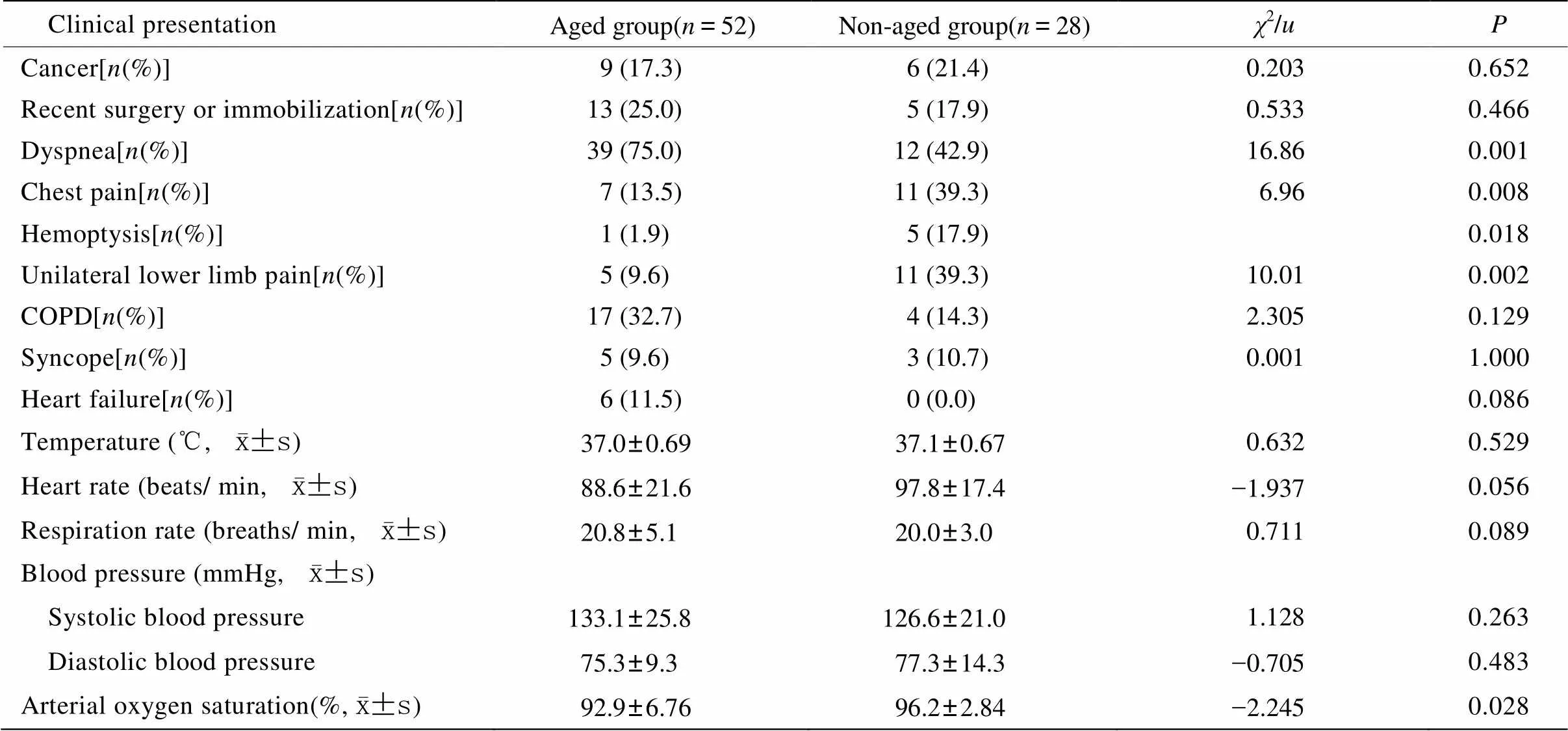
表2 老年与非老年PE患者的临床特征
PE: pulmonary embolism; COPD: chronic obstructive pulmonary disease. 1mmHg=0.133kPa
此外,进一步运用ROC曲线评估改良Geneva量表对PE的诊断价值。老年组改良Geneva量表ROC曲线见图1,AUC为0.974(95% CI:0.940~0.992),非老年组改良Geneva量表ROC曲线见图2,AUC为0.981(95% CI:0.924~0.998),老年组低于非老年组,=-1.965,=0.035,两者之间差异有统计学意义。提示改良Geneva量表对老年PE患者的诊断价值低于非老年患者。
2.3 血浆D−二聚体对老年和非老年患者PE的排除价值
检测血浆D−二聚体,比较其对两组疑诊PE的排除价值。老年组61例血浆D−二聚体<500μg/L的患者中,57例经CTPA排除PE诊断,提示血浆D−二聚体诊断老年PE的阴性预测值为93.4%;非老年组27例血浆D−二聚体<500μg/L的患者中24例经CTPA排除PE诊断,对非老年患者PE的阴性预测值为88.9%。
2.4 改良Geneva量表联合血浆D−二聚体对老年患者PE的排除价值
老年组改良Geneva量表≤3分且血浆D−二聚体<500μg/L的61例患者中经CTPA全部除外PE诊断,非老年组27例患者中经CTPA全部除外PE诊断,提示改良Geneva量表≤3分联合血浆D−二聚体<500μg/L对老年和非老年PE诊断的阴性预测值均为100%。可见两组患者中两项指标联合对PE的除外价值均高于单独血浆D−二聚体<500μg/L。
3 讨 论
随年龄增长,PE的发生率和死亡率明显增加[8]。我国老年定义为≥60岁,且符合中国老年医学会1995年提出的10点建议。老年患者合并多种疾病如呼吸系统疾病等,这些疾病的症状、体征与PE易混淆,容易误诊为PE,另外,老年人心肺功能差及受合并疾病的影响,导致发生PE时症状不典型,容易漏诊[4−6]。本研究276例患者,196例疑诊PE,但最终均经CTPA除外,早期误诊率较高。所以寻找快速诊断及除外PE的诊断方法至关重要。
有研究报道,改良Geneva量表联合D−二聚体诊断PE更准确[9]。该量表主要包括:下肢静脉血栓形成的危险因素、PE的主要症状及体征,有助于对可疑PE患者进行床旁快速的可能性评估,且不受临床医师的主观影响,依据量表评分将患者分为低度、中度、高度可能PE,国外有文献报道其具有一定的临床预测价值[10]。本研究以CTPA为确诊PE的金标准,应用改良Geneva量表对老年和非老年患者进行评分,证实该量表对老年患者诊断价值与非老年患者相似。ROC曲线是将检验指标的敏感度与特异度以图示方法结合,可准确反映二者关系,AUC越大,诊断准确性越高。本研究运用ROC曲线评价改良Geneva量表对老年组PE的诊断价值,结果显示老年组ROC的AUC低于非老年组,即改良Geneva量表在老年PE患者中的诊断价值受限,这可能是由于老年患者的临床表现缺乏特异性所致。
PE: pulmonary embolism; CTPA: computed tomography pulmonary arteriography.*Clinical probability of PE categorized by revised Geneva score: low probability: 0−3; medium probability: 4−10; high probability: ≥11.#PE was definitely diagnosed by CTPA
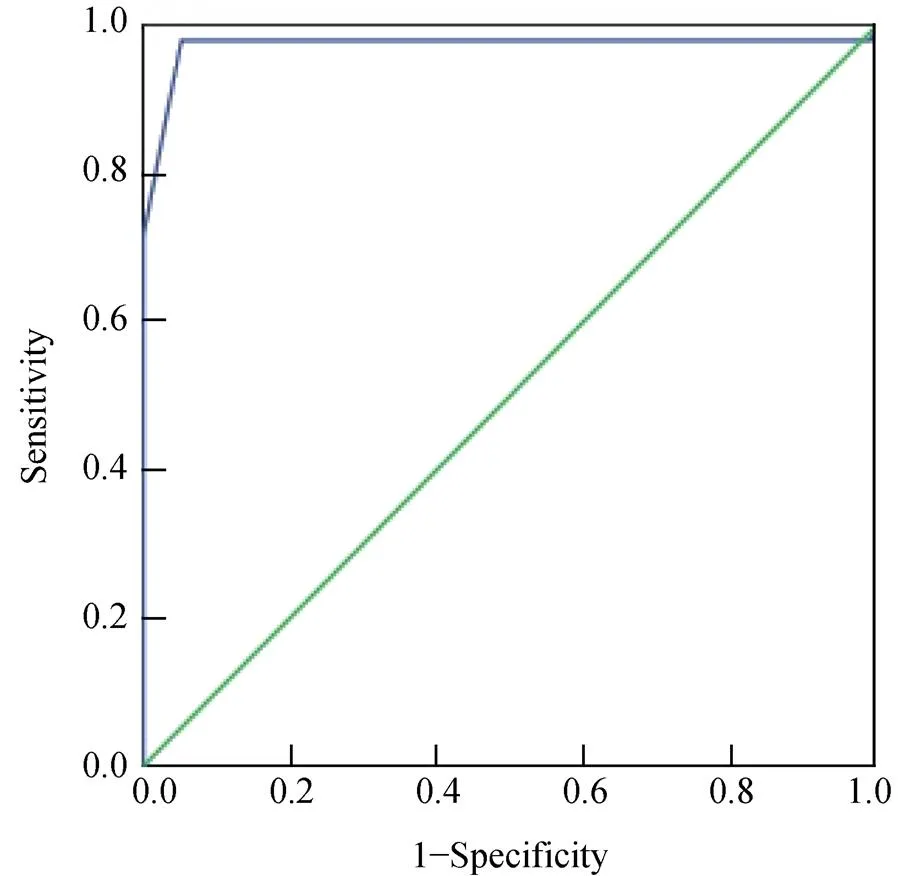
图1 改良Geneva量表预测老年PE的ROC曲线
Figure 1 The ROC curve of revised Geneva score for prediction of elderly PE ROC: receiver operating characteristics; PE: pulmonary embolism
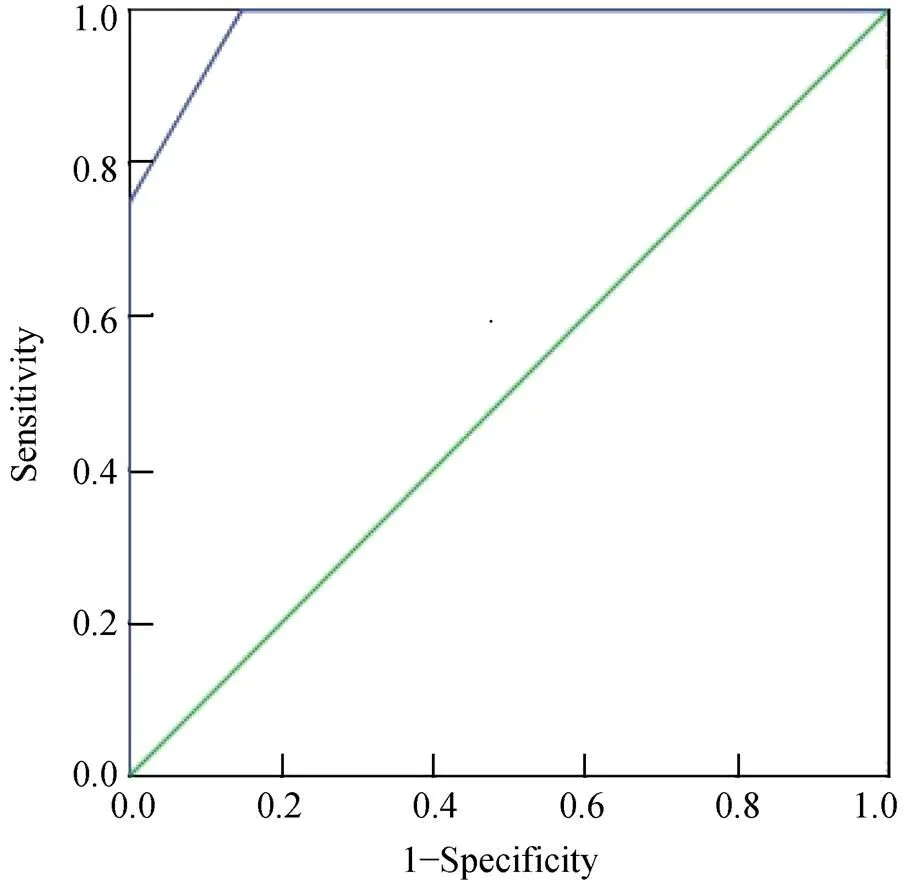
图2 改良Geneva量表预测非老年组PE的ROC曲线
Figure 2 The ROC curve of revised Geneva score for prediction of non-elderly PE ROC: receiver operating characteristics; PE: pulmonary embolism
血浆D−二聚体作为交联纤维蛋白在纤溶系统作用下产生的可溶性降解产物,其水平增高反映机体高凝状态和继发性纤溶亢进,常见于静脉血栓栓塞[11]。高龄、肌酐水平升高及合并心肌梗死、感染、手术、肿瘤等均可导致D−二聚体升高,老年患者上述危险因素和疾病的发病率均明显增加,使其诊断的敏感度和特异度降低[8]。目前主要将血浆D−二聚体水平作为PE的除外标准,但其阴性预测值仅约94%[12],仍存在假阴性可能。本研究显示在老年PE患者血浆D−二聚体的阴性预测值为93.4%,非老年组为88.9%,与其他报道一致。
有荟萃分析[13]表明,经Geneva量表或改良Geneva量表评估为“低、中度可能PE”同时D−二聚体水平正常可安全除外PE。我们的研究也得出了类似的结果,在本研究中老年组改良Geneva量表≤3分联合D−二聚体<500μg/L可将诊断的阴性预测值提高至100%。国外有研究报道,Wells量表≤4分联合血浆D−二聚体<500μg/L可将诊断的阴性预测值提高至100%[14,15],表明在诊断PE方面,改良的Geneva量表和Wells量表具有同样的价值,这与Douma等[16]的研究一致。但是Wells量表中的1项指标“除PE外其他诊断可能性小”具有很大的主观性且易受量表中其他变量的影响,降低了其诊断价值和可重复性。改良Geneva量表则采用完全客观的指标进行评分,方法简单且不易受主观因素的影响。
总之,与非老年患者相比,改良Geneva量表对PE诊断价值有限,应综合评估患者的症状、体征及危险因素,在以往患有PE,呼吸困难,下肢疼痛,有心血管基础病史时应尤为注意。除外PE时,改良Geneva量表≤3分联合血浆D−二聚体<500μg/L对老年PE的阴性预测值高于单独血浆D−二聚体<500μg/L,可用于老年患者快速除外PE诊断,减少不必要的影像学检查。本研究为单中心,小样本研究,可能存在偏差,仍需多中心,大样本资料进一步验证。
[1] Guo DJ, Hu DY, Zhou WR. Clinical analysis on diagnosis and treatment of acute pulmonary embolism[J]. Chin J Cardiol, 2003, 31(1): 49−51. [郭丹杰, 胡大一, 周伟荣. 急性肺栓塞诊断治疗的临床分析及探讨[J]. 中华心血管病杂志, 2003, 31(1): 49−51.]
[2] Carson JL, Kelley MA, Duff A,. The clinical course of pulmonary embolism[J]. N Engl J Med, 1992, 326(19): 1240−1245.
[3] Go AS, Mozaffarian D, Roger VL,. Heart disease and stroke statistics—2014 update: a report from the American Heart Association[J]. Circulation, 2014, 129(3): e28−e292.
[4] Liu CP, Li XM, Chen HW,. Depression, anxiety and influencing factors in patients with acute pulmonary embolism[J]. Chin Med J(Engl), 2011, 124(16): 2438−2442.
[5] Osório J. New D-dimer cut-off value helps to rule out pulmonary embolism in the elderly[J]. Nat Rev Cardiol, 2010, 7(7): 358.
[6] Guo Z, Ma Q, Zheng Y,. Normal blood D-dimer concentrations: do they exclude pulmonary embolism[J]? Chin Med J(Engl), 2014, 127(1): 18−22.
[7] Le Gal G, Righini M, Roy PM,. Prediction of pulmonary embolism in the emergency department: the revised Geneva score[J]. Ann Intern Med, 2006, 144(3): 165−171.
[8] Stein PD, Hull RD, Kayali F,. Venous thromboembolism according to age: the impact of an aging population[J]. Arch Intern Med, 2004, 164(20): 2260−2265.
[9] Chagnon I, Bounameaux H, Aujesky D,Comparison of two clinical prediction rules and implicit assessment among patients with suspected pulmonary embolism[J]. Am J Med, 2002, 113(4): 269−275.
[10] Klok FA, Karami Djurabi R, Nijkeuter M,Alternative diagnosis other than pulmonary embolism as a subjective variable in the Wells clinical decision rule: not so bad after all[J]. J Thromb Haemost, 2007, 5(5): 1079−1080.
[11] Parent F, Maître S, Meyer G,. Diagnostic value of D-dimer in patients with suspected pulmonary embolism: results from a multicentre outcome study[J]. Thromb Res, 2007, 120(2): 195−200.
[12] Wang Y, Liu ZH, Zhang HL,. Predictive value of D-dimer test for recurrent venous thromboembolism at hospital discharge in patients with acute pulmonary embolism[J]. J Thromb Thrombolysis, 2011, 32(4): 410−416.
[13] Carrier M, Righini M, Djurabi RK,. VIDAS D-dimer in combination with clinical pre-test probability to rule out pulmonary embolism. A systematic review of management outcome studies[J]. Thromb Haemost, 2009, 101(5): 886−892.
[14] Pasha SM, Klok FA, Snoep JD,Safety of excluding acute pulmonary embolism based on an unlikely clinical probability by the Wells rule and normal D-dimer concentration: a meta-analysis[J]. Thromb Res, 2010, 125(4): e123−e127.
[15] Klok FA, Kruisman E, Spaan J,. Comparison of the revised Geneva score with the Wells rule for assessing clinical probability of pulmonary embolism[J]. Thromb Haemost, 2008, 6(1): 40−44.
[16] Douma RA, Mos IC, Erkens PM,. Performance of 4 clinical decision rules in the diagnostic management of acute pulmonary embolism[J]. Ann Intern Med, 2011, 154(11): 709−718.
(编辑: 周宇红)
Diagnostic value of revised Geneva score combined with plasma level of D-dimer for suspected pulmonary embolism in elderly patients
HU Jing-Min, ZHAO Can, GUO Dan-Jie*
(Heart Center, People’s Hospital, Peking University, Beijing 100044, China)
To evaluate the clinical diagnostic and exclusive values of revised Geneva score and its combination with plasma level of D-dimer for suspected pulmonary embolism (PE) in the elderly patients.A total of 276 patients with suspected PE due to chest pain and dyspnea admitted in our hospital from January 2009 to April 2014 were enrolled in this study. They were divided into 2 groups based on their age, that is, the aged group (≥60 years old) and the non-aged group (<60 years old). Computed tomography pulmonary arteriography (CTPA) was considered as the gold standard for diagnosis. According to the revised Geneva score, the diagnosis of PE was categoried into different clinical probability,low, medium and high probability, and their plasma level of D-dimer was also tested. Based on their clinical features, the diagnostic values of revised Geneva score, the exclusive values of plasma D-dimer, and that of combining revised Geneva score with D-dimer together were analyzed between the 2 groups. The receiver operating characteristics (ROC) curve was used to evaluate the overall accuracy of revised Geneva score in the diagnosis of PE.Among the cohort with suspected PE, 80 cases were definitely diagnosed as PE by CTPA (52 cases ≥60 years old, and 28 cases <60 years old). The area under the ROC curve (AUC) was 0.974 (95% CI: 0.940−0.992) for the aged group and 0.981 (95% CI: 0.924−0.998)for the non-aged one, with significant difference between them (<0.001). The negative predictive values of D-dimer, and the revised Geneva score combined with D-dimer were 93.8% and 100.0% respectively for the aged patients, and 88.9% and 100.0% for the non-aged patients.The clinical features of PE are atypical in the elderly patients. The revised Geneva score has lower diagnostic value for the aged than the non-aged patients. Combination of revised Geneva score and plasma level of D-dimer is a safe strategy to rule out PE and is better than D-dimer alone for the aged and non-aged patients with suspected PE.
elderly; pulmonary embolism; revised Geneva score; plasma D-dimer
R543.2; R592
A
10.11915/j.issn.1671-5403.2015.04.066
2015−01−07;
2015−02−05
郭丹杰, E-mail: guodanjie@pkuph.edu.cn
