颈前路椎间盘切除植骨融合术后吞咽困难36例分析
2015-03-21朱守荣张永刚
吴 兵,朱守荣,王 岩,张永刚
解放军总医院 骨科,北京 100853
颈前路椎间盘切除植骨融合术后吞咽困难36例分析
吴 兵,朱守荣,王 岩,张永刚
解放军总医院 骨科,北京 100853
目的探讨颈前路椎间盘切除植骨融合(anterior cervical discectomy and fusion,ACDF)术后吞咽困难的原因、危险因素、治疗方法。方法回顾性分析我科2013年1 - 12月收治的行ACDF患者355例。36例出现吞咽困难,其中男性12例,女性24例,平均年龄46.6(36 ~ 75)岁。结果36例均随访6个月以上,分别于术后1 ~ 4 d、术后3个月、术后6个月记录Bazaz吞咽困难评分。术后1 ~ 4 d吞咽困难发生率10.1%,术后3个月、6个月分别为6.2%、2.3%。随访3个月时无重度吞咽困难患者。Logistic回归分析显示,多节段颈椎手术及高位颈椎手术是术后出现吞咽困难的危险因素。结论多节段减压固定及高位颈椎手术是潜在的危险因素。术中注意保护颈部神经、采用甲泼尼龙治疗,可有效减少术后吞咽困难的发生。
吞咽困难;椎间盘切除术;颈椎病;手术并发症
吞咽困难是颈椎病患者经颈前路椎间盘切除植骨融合(anterior cervical discectomy and fusion,ACDF)术后的并发症之一,多数患者临床表现轻,遗留严重症状的病例少,故临床重视程度不够。近年国内外对颈椎术后吞咽困难关注度有所增加[1-5]。中、重度吞咽困难对患者生活质量及心理有较大影响,需引起临床重视。本文旨在探讨ACDF术后吞咽困难的原因、可能的危险因素及有效的防治方法。
资料和方法
1 病例资料 选取我科2013年1 - 12月收治的行ACDF的颈椎病患者355例,术前无吞咽困难的主诉。男性212例,女性143例,平均年龄42.3(33~81)岁。患者在全麻下手术,减压方式包括单纯间盘切除、椎体次全切或两种并存,切除后纵韧带彻底减压。钛板螺钉固定者296例,Zero-p固定者59例(“零切迹钛板”,植入后,椎前无突出的内固定物)。单节段减压融合固定211例,双节段107例,三节段35例,四节段2例。所有患者术中均给予甲泼尼龙1 g冲击治疗,术后3 d小剂量(80 mg/d)维持;术后同时使用甲钴胺、神经节苷脂治疗。部分文献报道高位颈椎(C2/3、C3/4) ACDF术后吞咽困难的发病率似较高,我们做此假定,分为两组:累及C3/4及以上节段者35例(包括多节段病例),余下320例为C3/4以下节段者[6-9]。
2 评价标准 采用Bazaz吞咽困难评价标准:无:进食流质食物和固体食物时均无吞咽困难;轻度:进食固体食物时很少发生吞咽困难,进食流质食物时无障碍;中度:进食固体食物时偶尔发生吞咽困难,进食流质食物很少发生;重度:进食固体食物时经常发生吞咽困难,无论进食流质食物时有或无障碍[7]。术后1 ~ 4 d第1次评价,术后3个月、6个月门诊或电话随访。
3 统计学方法 将病例资料进行二项Logistic回归分析。所有统计处理采用SPSS17.0计算。
结 果
1 吞咽困难发生率 术后1 ~ 4 d主诉吞咽困难36例,平均年龄46.6(36 ~ 75)岁,男12例(发生率为5.66%),女24例(发生率为16.78%)。从手术节段数看,吞咽困难发生率随节段数增多而增高。从手术节段的部位看,累及高位颈椎时发生率明显增高。从内固定方式看,钛板螺钉内固定组发病率为10.1%,Zero-p固定组为10.2%。术后3个月随访325例,吞咽困难20例(发生率6.2%,女14例,男6例);术后6个月随访300例,吞咽困难7例(发生率2.3%,女5例,男2例)。术后1 ~4 d吞咽困难36例中,重度2例、中度9例、轻度25例;术后3个月时无重度病例,中度6例、轻度14例;术后6个月时,中度2例、轻度5例。见表1。
2 危险因素的Logistic分析 本组病例中性别、年龄及内固定方式对术后吞咽困难并无统计学差异。而手术节段数、固定部位有统计学差异(P<0.01)。见表2。

表1 ACDF术后1 ~ 4 d吞咽困难的发生率Tab. 1 Incidence rate of dysphagia after ACDF from 1 to 4 days
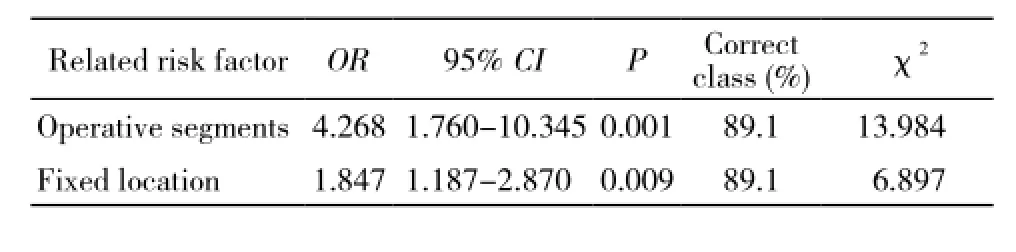
表2 ACDF术后1 ~ 4 d吞咽困难的Logistic分析Tab. 2 Logistic regression analysis of dysphagia after ACDF from 1 to 4 days
讨 论
吞咽过程受多支神经支配,主要包括舌下神经、舌咽神经、喉上神经、喉返神经、迷走神经,这些神经穿过或接近颈前手术入路,直接或间接损伤会引起不同程度及表现形式的吞咽功能障碍[10-11]。还有一些研究表明,部分患者术前即存在吞咽功能异常,推测可能是由于颈脊髓受压,引起中枢性损害及吞咽动作的神经冲动传导异常[12-13]。故脊髓型颈椎病的患者可能是术后吞咽困难的易感人群。
由于对吞咽困难定义不清以及评价方法不统一,文献报道ACDF术后吞咽困难发病率为2% ~77%[2-5]。我们采用Bazaz标准,重点关注患者吞咽固体或流食的主观体验。本研究显示,吞咽困难发生率较低,且随时间推移减少,严重程度减轻。可能的原因是:1)我院颈前路手术技术相对成熟,神经损伤概率低。2)常规术中应用甲泼尼龙冲击,术后3 d小剂量维持。Cho等[13]认为,颈椎手术使用类固醇可减轻吞咽困难的发生率。而Pedram等[14]认为颈前路手术使用甲泼尼龙不能减少吞咽困难的发生率,但该研究给药方式剂量相对保守。我们认为本研究较低的发生率与甲泼尼龙治疗可能存在一定关联。3)术后应用甲钴胺、神经节苷脂等神经营养药物,对神经损伤有一定的预防和治疗作用,可能使部分患者原本要出现的症状被掩盖。
许多文献报道了颈椎前路术后出现吞咽困难的危险因素,如性别、高龄、术前已有吞咽困难、多节段手术、手术部位等[2,7-10,13]。女性是报道比较集中的危险因素,原因不清。Bazaz等[7]报道女性发生率在24.7%、男性仅11.7%;Lee等[8]发现女性吞咽困难的发生率是男性的2倍左右;本研究亦显示女性发生率约为男性的3倍。多节段手术也是提及较多的因素,Riley等[9]发现3节段手术吞咽困难发生率显著增高。本研究也显示,手术节段越多、累及C3/4及以上节段的高位颈椎手术是术后吞咽困难的危险因素。然而,多节段颈椎手术可能包含高位颈椎节段,不同节段部位的手术引起神经损伤的风险并不一致,故这两个因素应该结合临床进行分析。
多项研究表明,是否使用钛板内固定,对吞咽困难发生率的影响并没有统计学的差异[2,5,7-9,13]。但Azab等[15]发现使用超薄钛板术后吞咽困难发生率较低。还有作者得出3 ~ 7 mm厚度钛板不会增加术后吞咽困难发生率的结论[5]。我们采用椎前切迹差值较大的两种内固定材料进行对比,发生率未发现明显差异。
吞咽困难是ACDF术后并发症之一,女性相对多见,尽管总体预后较好,但症状严重时对患者生活质量有很大影响,需引起临床医生的高度重视。多节段减压固定融合术及高位颈椎手术是潜在的危险因素。手术中操作轻柔、注意保护颈部神经、围术期采用甲泼尼龙治疗,可能会有效减少术后吞咽困难的发生。
1 Phillips FM, Lee JY, Geisler FH, et al. A prospective, randomized,controlled clinical investigation comparing PCM cervical disc arthroplasty with anterior cervical discectomy and fusion 2-Year results from the US FDA IDE clinical trial[J]. Spine (Phila Pa 1976), 2013, 38(15): E907-E918.
2 Rihn JA, Kane J, Albert TJ, et al. What is the incidence and severity of dysphagia after anterior cervical surgery?[J]. Clin Orthop Relat Res, 2011, 469(3): 658-665.
3 Mummaneni PV, Burkus JK, Haid RW, et al. Clinical and radiographic analysis of cervical disc arthroplasty compared with allograft fusion: a randomized controlled clinical trial[J]. J Neurosurg Spine, 2007, 6(3):198-209.
4 Shih P, Simon PE, Pelzer HJ, et al. Osteophyte formation after multilevel anterior cervical discectomy and fusion causing a delayed presentation of functional dysphagia[J]. Spine J, 2010, 10(7):e1-e5.
5 Chin KR, Eiszner JR, Adams SB Jr. Role of plate thickness as a cause of dysphagia after anterior cervical fusion[J]. Spine (Phila Pa 1976), 2007, 32(23):2585-2590.
6 Papavero L, Heese O, Klotz-Regener V, et al. The impact of esophagus retraction on early dysphagia after anterior cervical surgery: does a correlation exist?[J]. Spine (Phila Pa 1976),2007, 32(10):1089-1093.
7 Bazaz R, Lee MJ, Yoo JU. Incidence of dysphagia after anterior cervical spine surgery: a prospective study[J]. Spine(Phila Pa 1976), 2002, 27(22):2453-2458.
8 Lee MJ, Bazaz R, Furey CG, et al. Risk factors for dysphagia after anterior cervical spine surgery: a two-year prospective cohort study[J]. Spine J, 2007, 7(2):141-147.
9 Riley LH, Skolasky RL, Albert TJ, et al. Dysphagia after anterior cervical decompression and fusion - Prevalence and risk factors from a longitudinal cohort study[J]. Spine (Phila Pa 1976), 2005, 30(22): 2564-2569.
10 Martin RE, Neary MA, Diamant NE. Dysphagia following anterior cervical spine surgery[J]. Dysphagia, 1997, 12(1):2-8.
11 Schindler JS, Kelly JH. Swallowing disorders in the elderly[J]. Laryngoscope, 2002, 112(4):589-602.
12 Frempong-Boadu A, Houten JK, Osborn B, et al. Swallowing and speech dysfunction in patients undergoing anterior cervical discectomy and fusion: a prospective, objective preoperative and postoperative assessment[J]. J Spinal Disord Tech, 2002, 15(5):362-368.
13 Cho SK, Lu Y, Lee DH. Dysphagia following anterior cervical spinal surgery A SYSTEMATIC REVIEW[J]. Bone Joint J, 2013, 95B(7):868-873.
14 Pedram M, Castagnera L, Carat X, et al. Pharyngolaryngeal lesions in patients undergoing cervical spine surgery through the anterior approach: contribution of methylprednisolone[J]. Eur Spine J,2003, 12(1):84-90.
15 Azab W, Abdel-Razek M, Ali A, et al. Outcome evaluation of a Zero-Profile implant for anterior cervical diskectomy with fusion[J]. Turk Neurosurg, 2012, 22(5): 611-617.
Patients with dysphagia after anterior cervical discectomy and fusion: An analysis of 36 cases
WU Bing, ZHU Shourong, WANG Yan, ZHANG Yonggang
Department of Orthopedics, Chinese PLA General Hospital, Beijing 100853, China
ZHU Shourong. Email: zhusr301@aliyun.com
Objective To discuss the cause, risk factors and treatment of dysphagia after anterior cervical discectomy and fusion (ACDF). Methods Clinical data about 36 cases with dysphagia selected from 355 cases who accepted ACDF in our hospital from January 2013 to December 2013, including 12 males and 24 females with an average age of 46.6 years old (range from 36-75 years old), were retrospectively analyzed. Results All the 36 patients with dysphagia, whose Bazaz's score were respectively recorded at postoperative 1-4 days, 3rd month and 6th month, were followed up at least 6 months. The incidence rate of dysphagia was 10.1% at postoperative 1-4 days, 6.2% at postoperative 3rd month, and 2.3% at postoperative 6th month. There were no cases with severe dysphagia at postoperative 3rd month. Logistic regression analysis showed that multiple segmental cervical spine surgery and highlevel cervical spine surgery might be the risk factors of postoperative dysphagia. Conclusion Multiple segmental decompression and fusion and high cervical spine surgery are two potential risk factors. The occurrence of dysphagia after ACDF can be avoided by the protection of cervical nerves and the usage of methylprednisolone.
dysphagia; discectomy; cervical spondylosis; operative complications
R 619
A
2095-5227(2015)02-0121-03
10.3969/j.issn.2095-5227.2015.02.007
时间:2014-09-12 10:46
http://www.cnki.net/kcms/detail/11.3275.R.20140912.1046.001.html
2014-07-18
吴兵,男,硕士,主治医师。Email: foxwu20002000@ 126.com
朱守荣,男,硕士,副主任医师。Email: zhusr301@aliyun. com
