鼓膜完整的传导性耳聋相关影像鉴别和治疗策略
2018-04-19刘阳
刘阳
海军总医院耳鼻咽喉头颈外科(北京100048)
鼓膜完整的传导性耳聋是一组具有共同临床特征的疾病,本文以病理和胚胎发生学为出发点,针对临床影像诊断和外科治疗策略进行梳理总结。主要疾病谱包括:耳硬化症、鼓室硬化、外伤性听骨链中断、先天性胆脂瘤、先天性听骨链畸形。其共同临床特征是:外耳道正常、鼓膜完整、传导性耳聋、A型曲线(包括As型和Ad型)、盖莱试验阴性。其它临床罕见内耳传导性耳聋如大前庭导水管综合征、上半规管裂综合征、外后半规管裂综合征、X-连锁镫井喷综合征等[1]不在本文讨论范围。其它鼓膜完整的分泌性中耳炎、粘连性中耳炎、隐匿性中耳炎等也不属于本文讨论范围。
传统HRCT常规平片能够很好的显示鼓室、鼓窦、乳突病变状态,即是否存在密度增高影及骨质破坏,因为这涉及到是否开放乳突等手术策略问题,而本组以听骨链为主的疾病则鼓室乳突鼓窦基本正常;HRCT常规平片提供的另外一个重要信息是颞骨内重要结构如内听道、耳蜗、半规管、乙状窦、颈静脉球等是否正常、畸形或破坏;但HRCT常规平片并不能很好的显示听骨链的精细结构,唐朝颖(2016)报告HRCT对先天性听骨链畸形的显示仅为40%,外伤性听骨链中断仅为50%[2]。但是,近年发展的多平面重组MPR(multi-planar ref⁃ormation)和三维容积重建技术3D-CTVR(three-dimensional volume rendered computer tomog⁃raphy)则能够很好的显示锤砧骨、镫骨及其连接,在影像上能够直观的鉴别听骨链是否完整、破坏、畸形、连接异常[34]。MPR与CTVR技术是应用现代螺旋CT,通过“各向同性扫描”方式获得组织结构内部的点阵信息(即容积数据)后,将数据通过后处理技术进行重建获得各种图像。MPR图像可以理解为将三维影像投影到同一平面,从而实现同层全程显示;CTVR则是以不同阈值用不同颜色代表,对应不同结构,通过视觉色差在人眼视网膜获得三维信息,通过旋转、阈值滤过实现物体内部的三维结构显示[4-6]。因此本文侧重于从现代影像学角度论述上述具有共同特征的一组疾病的鉴别诊断,同时兼顾各疾病的胚胎发生学及病理解剖学特征,外科听力重建方法以2013年中华耳鼻咽喉头颈外科杂志刊登《中耳炎临床分类和手术分型指南(2012)》及解读[7,8]中Ⅱ、Ⅲ型鼓室成形术为参照,介绍手术策略但不做详细的技术描述。
1 耳硬化症
1、耳硬化症(otosclerosis)于1704年由Valsava首次发现,1872由 Anton von Tröltsch 首先命名[9]。主要病理改变是耳囊骨质局灶性吸收与富含血管的海绵状新骨形成,如果这种病理改变发生或发展至前庭窗周围及环韧带导致底板固定,即可引起传导性耳聋。需要注意的是耳硬化症底板固定和先天性底板骨化是二个概念,耳硬化症主要是底板边缘和前庭窗之间形成新生骨质导致底板固定,而先天性底板骨化则是胚胎发育过程中,来自耳囊的环韧带发育不全或发育后骨化形成[10]。
2、临床诊断主要依靠病史和听力学检查。影像诊断方面常规HRCT有时可在前庭窗周围见蚕食样改变。MPR和CTVR在耳硬化症中可显示完整的听骨链,其意义在于鉴别排除听骨链中断和听骨链畸形,见图1。
3、手术方法从最初的镫骨撼动逐步演变为镫骨全切除、镫骨部分切除,直至目前底板造孔后Piston植入技术[11]。
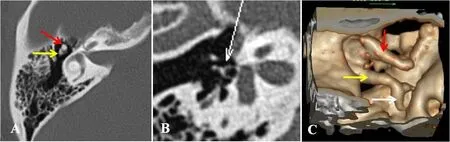
图1 耳硬化症。A:HRCT常规平片轴位,可见锤骨头(红箭头)和砧骨体(黄箭头),耳蜗和前庭骨质未见蚕食样改变。B:MPR图片,显示完整镫骨(白箭头),可见镫骨头、前后弓、镫骨底板,注意底板中央部分密度略低,在MPR图片上提示可能为软骨。C:CTVR图像,听骨链三维容积重建后完整显示听骨结构及连接,锤骨(红箭头)、砧骨(黄箭头)、镫骨(白箭头)及其前后弓和底板显示良好,从而鉴别区分了听骨链中断及畸形。Fig.1 Otosclerosis.A:Conventional axial section plane of HRCT image.Themalleus head(red arrow)and incus body(yellow arrow)is visible,the cochlear and vestibular bone shows no eroded sign.B:MPR image.The normal head,crus,and foot plane of staps can be seen.The central part of foot plane can be noted because of lower density,whichmay indicate cartilage.C:CTVR image.The whole ossicular structure and connection can be displayed well after three-dimensional reconstruction.This 3D image can exclude the ossicular chain disruption and deform ity.red arrow:malleus;yellow arrow:incus;white arrow:stapes.
2 鼓室硬化
1、鼓室硬化(tympanosclerosis)是中耳在长期慢性炎症愈合后所遗留的中耳结缔组织退行性改变,1873 年由 Von Troltsh[12]最先提出,Ho KY.(2010)年报告在中耳炎疾病中的发生率为5.5%[13]。其主要病理表现是钙盐沉积在鼓膜纤维层、鼓岬粘膜、听骨链周围,严重者可包裹整个听骨链或镫骨区域,导致听骨链固定,甚至导致底板骨化。
2、在临床诊断中除病史和听力学特征外,HRCT影像对鼓室硬化的特异影像检出率极低,有报道仅为26.13%,对听骨链中断的漏诊率为51.61%[14]。而重建后的MPR图像对钙化、骨化灶则显示良好,其钙化灶密度较软组织高但不均匀,钙化灶可包裹镫骨或与面神经粘连,见图2。在影像上单纯从底板形态与耳硬化症很难区别,但钙化灶可间接提示鼓室硬化。
3、清除病灶后听骨链重建的方式可按以下思路完成手术:①全听骨链活动完整,则保留听骨链;②底板活动,镫骨上结构完整,可按Ⅱ型手术完成;③底板活动,镫骨上结构缺如,可按Ⅲ型手术完成(图2-3);④底板固定骨化,可按耳硬化症手术完成,如果底板开窗后有内耳感染风险,可待二期手术底板开窗听力重建[15]。⑤震动声桥(VSB)植入:Pau HW(2010)年报告在二窗被钙化灶严重阻塞的情况下,在鼓岬开窗植入VSB振动子[16]。

图2 鼓室硬化.A:MPR图片,显示锤骨及融合的锤砧关节(白箭头),砧骨(黄箭头)长脚远端与钙化灶融合(红箭头),镫骨区域为密度高于软组织但低于骨组织的不均匀影像,为钙化灶(红箭头),完全包裹融合镫骨,同时与面神经相粘连(黑箭头)。B:黑箭头为暴露的面神经,红箭头显示镫骨区域广泛钙化灶。C:在剥离清除钙化灶后确认底板活动良好,植入TORP听骨(白箭头)。Fig.2 Tympanosclerosis.A:MPR image.The imaging showes the normal malleus and fused incudomalleolar joint(white arrow).The distal long processof incus(yellow arrow)confused w ith the calcification(red arrow).The density of ovalw indow area(red arrow)was higher than thatof the soft tissue but lower than that of the bone.This calcification surrounded the stapes and adhered to the facial nerve(black arrow).B:The black arrow indicate the naked facial nerve and the red arrow indicate the extensive calcification in the stapes area.C:The TORP(white arrow)was implanted after erdicating the calcification.
3 外伤性听骨链中断
1、外伤性听骨链中断可以是单纯的听骨链损伤,也可是颞骨骨折的一部分,如果仅有听骨链损伤,可表现为鼓膜完整的传导性耳聋。听骨链的病理损伤主要位于锤砧关节、砧镫关节分离移位、镫骨上结构骨折,少见的有前庭底板分离、底板骨折等等。
2、明确的外伤病史、面神经损伤、内耳损伤有助于诊断。影像诊断中常规HRCT平片对听骨链损伤的精细诊断缺乏特异性[17],但MPR图像及CT⁃VR图像则能够很好的显示听骨链损伤状态,定位损伤部位,特别是病史久远的外伤,砧骨长脚远端缺血骨质吸收等,见图3。
3、听骨链的重建是在颞骨骨折、内耳损伤、面神经损伤治疗恢复后的治疗,包括:①听骨链完整但关节离断错位、与周围组织粘连骨化等,可复位修复关节、分离粘连、或在过多分离的的关节间插入软骨片以连接听骨链(图3);②听骨链其它部位的损伤可按Ⅱ型和Ⅲ型鼓室成形完成;③底板的骨折可先以软组织覆盖骨折处再按Ⅱ型和Ⅲ型鼓室成形完成手术。
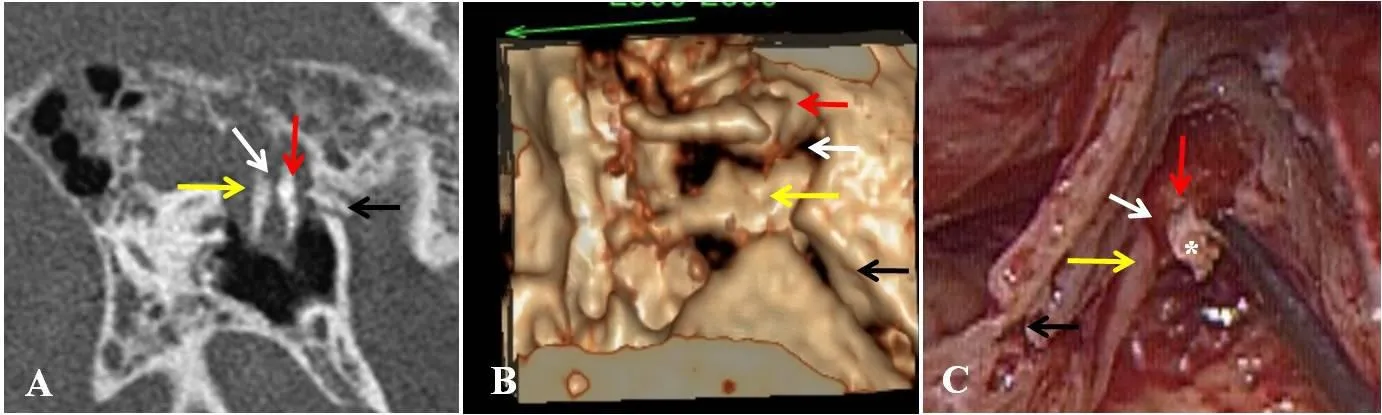
图3 外伤性听骨链中断.A:MPR图片,听骨周围可见软组织包裹,锤骨头(红箭头)与砧骨体(黄箭头)之间的锤砧关节(白箭头)呈分离状态,黑箭头指示骨折线;B:CTVR重建图像,滤除包裹听骨的软组织,显示听骨链状态,白箭头显示分离的锤砧关节;C:术中见鼓窦侧壁骨折线(黑箭头),锤砧关节分离(白箭头),白色星号为软骨,插入衬垫在锤砧关节之间,连接听骨链。Fig.3 Ttraumatic ossicular chain disruption.A:MPR image.The incudomalleolar joint was separated and the ossicular chain was surrounded by the soft tissue.red arrow:malleus head;yellow arrow:body of incus;black arrow:fracture line.B:CTVR image.After the soft tissue was filtered,the ossicular chain was displayed.White arrow:the disarticulated incudomalleolar joint.C:The broken line(black arrow)can be seen in the tympanic sinus wall.The white arrow indicate the separation of incudomalleolar joint.A small piece of cartilage(white asterisk)was inserted into the seperated incudomalleolar joint to connect the ossicular chain.
4 先天性胆脂瘤
1、先天性胆脂瘤是胚胎期外胚层上皮组织遗留于颞骨内发展而成的角化上皮,通常沿听骨内侧向后生长至中鼓室后上方,初期多破坏砧镫关节、镫骨上结构,最后逐渐发展为颞骨广泛胆脂瘤[18]。本文讨论的是Derlacki(1965)及Levenson(1986)描述的特征为胆脂瘤位于完整鼓膜内侧、伴中耳炎病史[19,20]的一组疾病,即胆脂瘤局限于鼓室引起听骨破坏导致传导性耳聋的病例。
2、常规HRCT对此病诊断并不困难,鼓窦鼓室内包裹听骨、边界清晰的软组织密度增高影提示胆脂瘤,在MRI影像中,T1加权像上呈中等偏低信号,T2加权像呈高信号,增强扫描无强化[21]。但对听骨链破坏部位的诊断,MPR图像及CTVR图像则更显优势,能够清晰的显示听骨破坏程度和缺失部位,见图4。
3、清除病灶后的听力重建与鼓室硬化基本相同,但底板固定开窗的少见。
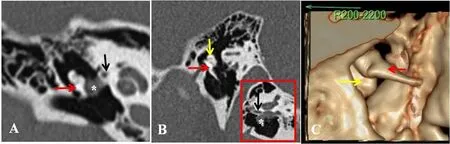
图4 先天性胆脂瘤。A:常规HRCT冠状位,红箭头指示锤骨,但听骨链结构不清,砧骨难以区分,听骨内侧软组织影(星号)提示胆脂瘤,与面神经紧邻(黑箭头),中鼓室及上鼓室内为良好的含气腔。B:MPR图像,红色箭头指示锤骨,黄色箭头指示砧骨体,未见砧骨长脚,右下红色方框内为面神经MPR图像,可见与胆脂瘤软组织影相粘连,面神经骨管部分缺如;C:CTVR三维重建图像,锤骨(红箭头)和砧骨体(黄箭头)显示清楚。滤除胆脂瘤软组织后,未见砧骨长脚和镫骨上结构。手术证实软组织影为胆脂瘤,砧骨长脚和镫骨上结构缺如,面神经水平段骨管破坏,术中以钛TORP听骨重建听骨链。Fig.4 Congenital cholesteatoma.A:Conventional coronal section plane of HRCT image.red arrow:malleus.The ossicular chain displayed unclearly and the incus could notbe identified well.The soft tissue(asterisk)inside the ossicles indicate the cholesteatoma contecting to the facial nerve(black arrow).The mesoty mpanum and attic was normal air cavity.B:MPR image.The red arrows indicate themalleus,the yellow arrow indicate the incus without long limb.The red box is the MPR image of facial nerve adhering to the cholesteatoma.C:CTVR image.The mallues(red arrow)and body of incus(yellow arrow)were displayed clearly.After the sofft tissue was filtered,the long limb of incus and stapes superstructure could not be seen.In the operation,the soft tissue was approved to be cholesteatoma,the long limb of incus and stapes superstructure absent,and the horizontal segmentof facial canal damaged.The titanium-TORPwas used to reconstruct the ossicular chain.
5 先天性听骨链畸形
广义的外中耳畸形包括耳廓畸形、外耳道畸形、中耳畸形。本文所述内容为非综合征型中耳畸形,主要为外耳道鼓膜正常的单纯听骨链畸形。1993年,Teunissen[22]较早的提出了中耳畸形的分类观点,随后 Nagao(1995)[23]、Okano(2003)[24]、袁虎(2005)[25]、Park K(2009)[26]等先后提出不同的分类观点。其中文献普遍引用的是Teunissen(1993)分类:Ⅰ类先天性镫骨固定;Ⅱ类先天性镫骨固定伴听骨链畸形;Ⅲ类先天性听骨链畸形但镫骨足板活动;Ⅳ类先天性前庭窗或蜗窗发育不全或重度发育异常。综合以上各家分类,为便于理解,本文从胚胎发生学和听力重建角度,以镫骨为中心分三个部分阐述:Ⅰ型-镫骨底板活动;Ⅱ型-镫骨底板固定;Ⅲ型-前庭窗骨性闭锁或未发育。
▲Ⅰ型-镫骨底板活动
1、胚胎发育第15周左右,第一腮弓内的Michle软骨发育成砧骨短脚、砧骨体、锤骨头等上鼓室内的听骨,如果上鼓室气化不良或Michle软骨不能完全吸收,则导致的听骨畸形主要表现为锤砧关节融合固定、砧骨体锤骨头与上鼓室骨质相融合连接[27,28];第二腮弓的Reichert软骨发育成锤骨柄、砧骨长脚、镫骨上结构、镫骨底板等中鼓室内的听骨,如果Reichert软骨发育不良导致的畸形主要表现以砧骨长脚和镫骨上结构的缺失为主[29-31]。因此,由Michle软骨和Reichert软骨发育导致的畸形可归纳为Ⅰ型,共同特点是镫骨底板活动,听骨链各部位可出现单独或合并畸形,包括锤骨头固定、砧骨体固定、锤砧关节固定、砧骨长脚缺如、砧镫骨软性连接、砧镫关节中断、孤立的豆状突、镫骨上结构与邻近结构的骨性条索状连接、镫骨上结构的缺失团块等。偶见面神经鼓室段低垂,挤压镫骨上结构[32]。考虑到现代外科重建技术,进一步分型镫骨上结构正常可列为Ⅰa型,镫骨上结构畸形可列为Ⅰb型。
2、在影像学听骨CT显示中,常规HRCT能够提示听骨链畸形,但更多精细结构并不能很好显示。MPR图像及CTVR则能够很好的显示畸形听骨精细结构,特别是镫骨前后弓在MPR图像中显示更为清晰,见图5-1-1,图5-1-2。外科听力重建中,Ⅰa型可按鼓室成形Ⅱ型完成,Ⅰb型则可按Ⅲ型完成。

图5-1-1 听骨链畸形Ⅰa型,A、B为MPR图片,C图为CT⁃VR图片。A图见锤骨(红箭头)完整,砧骨长脚缺如,砧骨体(黄箭头)与锤骨头融为一体;B图见镫骨结构良好,清晰可见前后弓、镫骨头(黑箭头)、底板;C图见锤骨柄(红箭头)良好,镫骨前后弓、镫骨头良好(黑箭头),但未见砧骨长脚。术中见镫骨底板活动,以PORP重建听骨链。Fig.5-1-1 Ossicular chain malformation type Ia.A&B:MPR image,C:CTVR images.A:The malleus(red arrow)was normal,the long process of incuswas absent,the body of in cus(yellow arrow)and the head of mallues was fused.B:The stapes was clear with the crus,head amd plate of stapes(black arrow)normaly,C:The hand of mallues(red arrow)together with crus and head of stapes(black arrow)was normal,,but the long limb of in cus wasabsent.The footplate of stapes wasmoved and the PORP was used to reconstruc the ossicular chain.
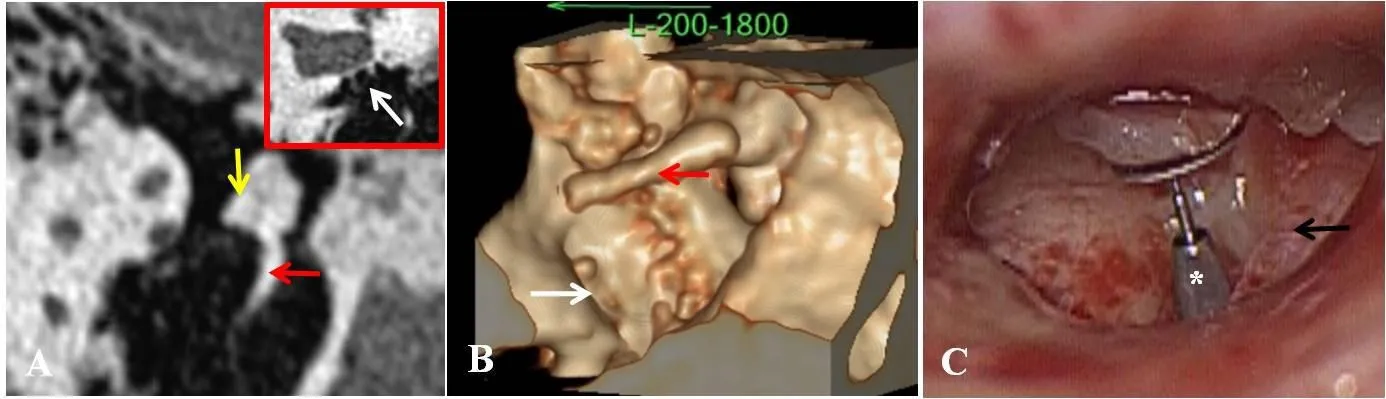
图5-1-2 听骨链畸形Ⅰb型,A图为MPR图片,见锤骨(红箭头)完整,砧骨长脚缺如,砧骨体(黄箭头)与锤骨头融为一体,红色方框内白色箭头指示为镫骨底板及底板上残余的骨性结构;B图为CTVR图片,红色箭头指示完整的锤骨柄,白色箭头指示镫骨底板及其上的残余结构,可能为前后弓发育过程中的残迹,未见砧骨长脚;C图为术中所见,镫骨上结构不存在,面神经(黑箭头)裸露低垂,覆盖前庭窗上缘,术中探查镫骨底板活动,以TORP(星号)重建听骨链。Fig.5-1-2 Ossicular chainmalformation type Ib.A:MPR image.Themalleus(red arrow)was normal,the long process of incus was absent,the body of incus(yellow arrow)and the head ofmallues was fused.The red box indicate the normal foot plate of stapesw ith the residual superstructure of stapes.B:CTVR image.The red arrow indicate the normal hand of mallus and thewhite arrow indicate the footplatew ith residual crus of stapes.The long limb of incuswas not seen.C:The surgical image.The stapes superstructure was absent,the facial nerve was dehiscent and cover the upper edge of oval w indow.The foot plate of stapes wasmoved and the TORP wasused to reconstruct the ossicular chain.
▲Ⅱ类-镫骨底板固定
1、在胚胎第14-18周,第一、二腮弓软骨发育成听骨链的同时,镫骨底板同时发育成熟,与来自迷路包囊的前庭窗及环韧带吻合[33],这一过程可导致底板固定,其胚胎发生的病理状态包括二种情况:其一是环韧带在胚胎期即没有完全发育,另外一种情况是虽已发育但出生后逐渐骨化[10],是否进一步发展成整个底板的骨化还缺乏足够的胚胎学证据。如果仅有底板固定,Teunissen[22]将其分为class1,如果底板固定的同时伴有由Michle和Reichert软骨分化而来的听骨链畸形,Teunissen[22]将其分为class2。但从现代手术方式角度看,无论底板以上听骨链结构是否正常,主流手术方式均以底板手术为核心,故本文将其列为Ⅱ类一起阐述,进一步分型仅有底板固定可列为Ⅱa型,合并底板上其他听骨链畸形可列为Ⅱb型,更有助于理解。
2、CT检查图像与Ⅰ型表现类似,如果镫骨底板以上结构正常,在CT图像上与耳硬化症不易区别,通常术中判断。外科听力重建通常在底板开窗处(底板全切除、部分切除、微孔技术)与砧骨长脚/锤骨柄之间建立连接,选用的重建材料包括TORP和Piston,类似耳硬化症手术(见图5-2)。

图5-2 听骨链畸形Ⅱ型术中图像。患者男性,28岁,气骨导间距语频30-35dB,自幼听力较差,术前影像听骨结构与耳硬化症相同,术前诊断考虑耳硬化症或先天性听骨链畸形。A图:见锤骨、砧骨(黄箭头)完整,锤砧关节活动度差,砧镫关节骨性融合,前后弓骨化,白色箭头指示去除前后弓的镫骨底板,呈骨化固定状态。黑色箭头指示面神经,骨管缺损,神经组织暴露但位置正常;B图:去除前后弓后,磨薄骨化的底板至略呈蓝色,以三棱针在底板中央偏后的位置钻孔开窗,见外淋巴液(红箭头);C图:以4.25mm Piston(星号)钛听骨重建听骨链。Fig.5-2 Ossicular chain malformation typeⅡ.A patient of 28 years old,male,had poor hearing at his childhood with A-Bgap 30-35dB(0.5,1,2KHz).The preoperative diagnosis was otosclerosis or congenital ossicular chain malformation.A:The mallus and incus were normal,the incudomallular joint moved poorly amd the incudostapedia joint was fused.The white arrow indicate the fixed foot plate with crus eradicated.The black arrow indicate the dehiscent facialnerve with normal poisition.B:The footplate was drillout(red arrow)to a hole with three edged needle after the crus mass was removed and the ossified footplate was bured to a thin bone.C:Theossicular chainwas reconstructed with a4.25mm Piston.
▲Ⅲ类:前庭窗骨性闭锁或未发育
在第一、二腮弓发育过程中的第8-10周,来自Reichert软骨的面神经组织与来自迷路包囊的骨管吻合;镫骨前庭窗吻合与面神经骨管吻合在时间与空间上高度相关,畸形相互影响[34]。所以在镫骨前庭窗区域的畸形中,前庭窗可能没有发育呈现骨性闭锁板(Ⅲ型)、或底板虽然与前庭窗吻合但底板与前庭窗骨性融合(Ⅱ型)、或底板与前庭窗吻合活动但镫骨上结构畸形(Ⅰ型),而面神经则可以部分或全部覆盖前庭窗[34-36]。因此前庭窗、镫骨、面神经胚胎发育互相影响所致畸形则列为单独一种类型。主要表现为前庭窗未发育、较厚的骨性闭锁板、前庭窗龛呈裂隙状狭窄等;同时可伴有一、二腮弓发育异常导致的听骨链畸形,畸形的镫骨或类似镫骨的畸形结构可以畸跨、挤压、覆盖面神经;裸露畸形的面神经走行在前庭窗上缘、正中或下缘或分叉走行,Su Y(2014)报告这一类型面神经畸形发生率69.1%(67/97)[36],de Alarcon A(2008)报告畸形发生率58.8%(10/17)[37]。
2、在影像学听小骨CT显示中,常规HRCT同样能够提示听骨链畸形,但MPR图像及CTVR则能够很好的显示畸形听骨精细结构。面神经走行异常的诊断在这一类型中至关重要,常规HRCT冠状位结合MPR图像,以下三点征象可以帮助诊断面神经畸形和前庭窗闭锁[38-40]见图5-3-1:①在HRCT冠状位平行通过上半规管平面划一条a线,再通过水平半规管基部划一条b线垂直a线,十字交叉线的外上象限即为面神经正常位置,如果面神经位于十字线外下象限即为走行畸形;②前庭窗龛MPR图像呈现“V”字形,说明前庭窗可能没有发育;③前庭窗闭锁骨板增厚,呈骨性结构,并非镫骨底板的半透明软骨征象。
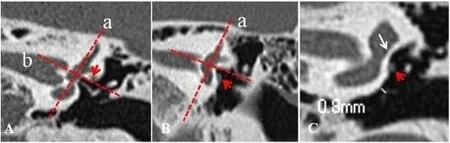
图5-3-1 面神经走行异常定位诊断。A&B:HRCT图像,a线平行通过上半规管平面,b线通过水平半规管根部垂直于a线,A图显示面神经(红箭头)处于正常位置,位于ab红十字交叉线外上象限,B图为畸形位置,位于交叉线外下象限(红箭头);B图同时显示前庭窗龛呈现横“V”字形,未见镫骨底板,提示前庭窗闭锁;C图为MPR图像,白箭头显示前庭窗呈骨性闭锁状态,与镫骨底板软骨的影像不同,闭锁板为骨性,红箭头指示面神经位于闭锁板下方。Fig.5-3-1 Localization of abnormal facial nerve in CT image.A&B:coronal secton plane of HRCT image.Line a:parallel to the plane of superior semicircular canal;Line b:crossing“line a”through the foot of horizontal semicircular canal;red arrow:facial nerve(A:normal position;B:abnormal position).The atretic oval window was displayed as“V”shape without foot plate in B image.C:MPR image.Thewhite arrow indicate the thick bone plate of oval window which is different from the cartilage of foot plate.The red arrow indicate the abnormal facial nerve inferior to the atretic plate of oval window.
3、外科治疗:①面神经位置正常或部分遮挡前庭窗:面神经可能位于前庭窗上缘或下缘,只要有足够的空间暴露前庭窗,即可将骨性闭锁的前庭窗骨板磨薄至蓝色菲薄骨质,按耳硬化症行全部/部分底板切除后在鼓膜底板之间以TORP连接,或应用微孔技术植入Piston听骨[32,41](图5-3-2)。②面神经完全覆盖前庭窗区域:此时在原前庭窗处植入听骨进行听力重建因面神经畸形已丧失条件,多数放弃,而传统的外半规管开窗因听骨链重建困难并不适合。尽管如此,仍有极具挑战性的重建技术供富有丰富经验的耳科医师选择:技术一:鼓阶开窗TORP植入技术[39-42](图5-3-3)。这一技术的主要方法是在圆窗膜前下鼓阶起始段磨除骨质至骨内膜,覆盖筋膜后放置TORP听骨,通过鼓膜-TORP-鼓阶外淋巴产生振动。这一方法的最大风险是引起神经性耳聋,关键是应保持骨内膜完整。技术二:震动声桥VSB植入[43-45],VSB振子可放置在圆窗龛,通过振动子-圆窗膜-鼓阶外淋巴产生振动,前提是圆窗龛没有闭锁,如果圆窗龛闭锁,则可以借鉴技术一将振动子放置在鼓阶起始段通过振动鼓阶外淋巴产生听力。

图5-3-2 先天性听骨链畸形Ⅲ型。A:HRCT图像,白色虚箭头指示闭锁的前庭窗,前庭窗龛呈现横“V”字形,未见镫骨底板,黑箭头指示面神经软组织影,无骨管,提示走行畸形,位于前庭窗龛下缘;B:CTVR图像,红箭头指示锤骨,形态良好,黄箭头指示砧骨长脚,远端变细,与畸形镫骨上结构相连(白箭头);C图:术中图像,黄箭头指示砧骨长脚,远端与畸形镫骨上结构(白箭头)融合连接,黑箭头指示裸露的面神经,位于闭锁的前庭窗下缘,白色虚箭头指示狭窄的前庭窗闭锁板,C图红色方框显示闭锁板机械打孔后植入Piston听骨。Fig.5-3-2 Ossicular chain malformation typeⅢ.A:HRCT image.The white dotted arrow indicate the atretic bone plate of over window which displays as a“V”shape.The black arrow indicate the abnormal naked facial nerve located to the lower edge of the oval window.B:CTVR image.The red arrow indicte the normal mullues and the yellow arrow indicte the thiner long limb connecting with the stapes superstructure(white arrow).C:Surgical image.The yellow arrow indicte the long limb of incus confussing with the stapes superstructure.The black arrow indicate the naked facial nerve located at the lower edge of oval window.The white dotted arrow indicate the narrow atretic bone plate of oval window.The red box shows the implanted Piston.

图5-3-3 先天性听骨链畸形Ⅲ型。A:HRCT图像,白色箭头指示闭锁的前庭窗骨板,厚度接近0.8mm,黑箭头指示面神经软组织,无骨管,提示走行畸形,位于前庭窗闭锁板下缘;B:CTVR图像,红箭头指示锤骨,形态良好,黄箭头指示砧骨长脚,远端变细,与畸形镫骨上结构相连,越过面神经(黑箭头)表面紧贴下方向前庭窗处走行;DEF为术中图像,D:黄箭头指示砧骨长脚,远端与畸形镫骨上结构融合连接,畸跨于裸露的面神经(黑箭头)表面,面神经完全覆盖前庭窗,白色虚箭头指示圆窗龛;E图黑色虚箭头指示在圆窗龛前方(圆窗膜的前下方)、面神经(黑箭头)下方磨除鼓岬骨质,暴露鼓阶起始段骨内膜,黄箭头指示砧镫关节,位于面神经表面,因角度关系镫骨上畸形结构被遮挡;F:显示鼓阶开窗处覆盖筋膜后植入TORP连接鼓膜;C图为术后影像,与A图同一部位,红色虚箭头指示植入的人工听骨,位于鼓阶起始段骨质内,没有进入鼓阶外淋巴腔,且位于面神经(黑箭头)下方,位置良好,与前庭窗开窗(白箭头处)具有相同的解剖学和传音生理学基础。Fig.5-3-3 Ossicular chain malformation typeⅢ.A:HRCT image.The white arrow indicates the atretic bone plate of oval w indow w ith 0.8mm thickness.The black arrow indicates the abnormal naked facial nerve located to the lower edge of oval w indow.B:CTVR Image.The red arrow indicates the normal mallus and the yellow arrow indicates the thiner long limb of crus that connected to the stapes superstructure,covered the naked facial nerve and arrived to the ovalw indow.D/E/F:Surgical image.D:The yellow arrow indicates the distal end of the long limb confused w ith the stapes superstructure and crossed naked facial nerve(black arrow).The facial nerval covered the ovalw indow fully.White dotted arrow:round w indow nich.E:The black dotted arrow indicates the burred position anterior to the round w indow nich and inferior to the facial nerve(black arrow).The bone of scala tympaniwas drilled out and the endosteum was exposed.The yellow arrow indicates the incudostapedia joint convering the facialnerve.F:The image displays the fenestration w ith the implanted TORP.C:Postoperative image.The red dottted arrow indicate the implanted TORP located at the initial segment of scal tympani.The TORP did not enter the perilymphatic cavity and located at the lower edge of facial nerve.The fenestration of scal tympani(white arrow)had the same anatomical and physiological theory comparing w ith the stepdectomy.
结语
本文所述内容为一组鼓膜完整的传导性耳聋病例的影像鉴别诊断与手术策略选择。既往术前诊断主要依靠病史和各自听力学特征,间接诊断鉴别成分较多,而现代影像特别是近年发展的三维影像重组技术,为这组疾病的鉴别提供了直观的影像,有利于术前更明确的诊断;本文手术策略的梳理总结则是根据现代听骨链重建技术的主流趋势,以镫骨病变及处理为中心进行概要论述,包括了经典手术,也有作者原创手术的经验,希望对同道临床工作有所帮助。
1 吴子明,张素珍,杨伟炎等.内耳病变导致的传导性耳聋.中华耳科学杂志,2005,3(3):222-223.Wu ZM,Zhang SZ,Yang EY.The Conductive Hearing Loss Caused by Inner Ear Lesions.Chinese Journal of Otology,2005,3(3):222-223.
2 唐朝颖,张纪帅,韩维举等.鼓膜完整的单耳传导性聋临床特点分析.中华耳鼻咽喉头颈外科杂志.2016,51(5):348-354.Tang CY,Zhang JS,Han WJ,et al.Analyses of the Clinical Char⁃acteristics of Unilateral Conductive Hearing Loss with Intacct Tympanic Membrane.Chin J Otorhinolaryngol Head Neck Surg,2016,51(5):348-354.
3 杨凤,宋任东,刘阳.三维容积重建对传导性耳聋听骨链的影像诊断.中华耳科学杂志.2015,13(4)663-666.Yang F,Song RD,Liu Y.3D-CTVR in Diagnosis of Integrity and Pathological Changes of Ossicular Chain in Conductive Hearing Loss.Chinese JournalofOtology,2015,13(4)663-666.
4 Liu Y,Yang F.Value of Section Plane,MPR,and 3D-CTVR Techniques in the Fine Differential Diagnosis of Ossicular Chain in the Case of Conductive Hearing Loss with Intact Tympanic Membrane.JournalofOtology,2017,12(2):80-85.
5 Zhang LC,Sha Y,Wang ZM,et al.3D Image of the Middle Ear Ossicles:Three Protocols of Post-processing Based on Multislice Computed Tomography.Eur Arch Otorhinolaryngol,2011,268(5):677-683.
6 Guo Y,Liu Y,Lu QH et al.CT Two-Dimensional Reformation versus Three-Dimensional Volume Rendering with Regard to Sur⁃gical Fndings in the Preoperative Assessment of the Ossicular Chain in Chronic Suppurative Otitis Media.Eur JRadiol.2013,82(9):1519–1524.
7 中华医学会耳鼻咽喉-头颈外科学分会耳科学组,中华耳鼻咽喉-头颈外科杂志编辑委员会耳科组.中耳炎临床分类和手术分型指南(2012).中华耳鼻咽喉头颈外科杂志.2013,48(1):5.Otology Committee of Chinese Medical Association of Otolaryngol⁃ogy Head and Neck Surgery,Editorial Committee of Chinese Jour⁃nal of Otolaryngology Head and Neck Surgery.The Otitis Media Clinical and Surgical Classification(2012)Guide.Chin JOtorhi⁃nolaryngol Head Neck Surg,2013,48(1):5.
8 孙建军,刘阳.中耳炎临床分类和手术分型指南(2012)解读.中华耳鼻咽喉头颈外科杂志.2013,48(1):6-10.Sun JJ,Liu Y.Otitis Media Clinical Classification and Surgical Classification Guide(2012)Interpretation.Chin JOtorhinolaryn⁃golHead Neck Surg,2013,48(1):6-10.
9 Hausler,R.General History of Stapedectomy.Adv Otorhinolaryn⁃gol,2007.65:1-5.
10 Raz Y,Lustig L.SurgicalManagementofConductive Hearing Loss in Children.Otolaryngol Clin North Am, 2002,35(4):853-875.
11 戴朴,宋跃帅.耳硬化症治疗沿革和中国之切入点.中华耳科学杂志,2012,10(3):300-302.Dai P,Song YS.The Treatment&Development of Otosclerosis and the Starting Point of China.Chinese Journal of Otology,2012,10(3):300-302.
12 王国鹏,龚树生.鼓室硬化的研究现状.中华耳鼻咽喉头颈外科杂志.2007,42(7):548-550.Wang GP,Gong SS.The Research Status of Tympanosclerosis.Chin JOtorhinolaryngol Head Neck Surg,2007,42(7):548-550.
13 Ho KY,Tsai SM,ChaiCY,et al.Clinical Analysis of In tratympan⁃ic Tympanosclerosis:Etiology,Ossicular Chain Findings,and Hearing Results of Surgery.Acta Otolaryngol,2010,13(3):370-374.
14 陈静,郑艳.鼓室硬化的颞骨HRCT表现与手术对照分析.中华耳科学杂志.2015,13(3):501-503.Chen J,Zheng Y.Temporal Bone CT Performance in Tympano⁃sclerosis with Different Ossicular Chain Lesions.Chinese Journal ofOtology,2015,13(3):501-503.
15 Gurr A,Hildmann H,Stark T S.Treatment of Tympanosclerosis,HNO:2008,56(6):651-657.
16 Pau HW,Just T.Third Window Vibroplasty:An Alternative in Surgical Treatment of Tympanosclerotic Obliteration of the Oval and Round Window Niche.Otol Neurotol,2010,31(2):225-657.
17 余蓉,陈晓巍.颞骨骨折致传导性聋的诊断与治疗进展.听力学及言语疾病杂志,2010,18(1):82-84.Yu R,Chen XW.The Progress in Diagnosis and Treatment of Con⁃ductive Deafness Caused by Temporal Bone Fracture.Journal of Audiology and Speech pathology,2010,18(1):82-84.
18 Koltai P J,Nelson M,Castellon R J,et al.The Natural History of Congenital Cholesteatoma.Arch Otolaryngol Head Neck Surg,2002,128(7):804-809.
19 Levenson MJ,Parisier SC,Chute P,et al.A Review of Twenty Congenital Cholesteatoma of the Middle Ear in Children.Otolar⁃yngol Head Neck Surg,1986;94:560-567.
20 陈希杭,程金妹,林昶等.颞骨先天性胆脂瘤的诊断和治疗.中华耳科学杂.2014,12(3):470-474.Chen XH,Cheng JM,Lin C,et al.Diagnosisand Treatment of Tem⁃poral Bone Congenital Cholesteatoma.Chinese Journal of Otolo⁃gy,2014,12(3):470-474.
21 龚桃根,柯朝阳.先天性中耳胆脂瘤的临床诊断与治疗进展.中华耳科学杂.2016,14(3):427-430.Gong TG,Ke ZY.Advances in Diagnosis and Treatment of Con⁃genital Middle Ear Cholesteatoma,Chinese Journal of Otology,2016,14(3):427-430.
22 Teunissen EB,Cremers WR.Classification of Congenital Middle Ear Anomalies:Report on 144 Ears.Ann Otol Rhinol Laryngol,1993,102:606-612.
23 Nagao Y,Nomura Y,Ohashi Y.Classification of Middle Ear Anomalies by a Correspondence Analysis Method.Nippon Jibi⁃inkoka Gakkai Kaiho[Article in Japanese],1995,98:16-23.
24 Okano T1,Iwanaga M,Yonamine H,et al.Congenital Auditory Os⁃sicle Malformation without External Ear Abnormality[Article in Japanese].Nihon Jibiinkoka Gakkai Kaiho,2003 ,106 (3):199-205.
25 袁虎,王秋菊,韩东一.先天性中耳畸形的临床分型及其与耳聋的相关性.中华耳鼻咽喉颈外科杂志,2005,40(12):893-895.Yuan H,Wang QJ,Han DY.Clinical Classification and Relation⁃ship with Conductive Deafness of Congenital Middle Ear Malfor⁃mations. Chin J Otorhinolaryngol Head Neck Surg,2005,40(12):893-895.
26 Park K,Choung YH.Isolated Congenital Ossicular Anomalies.Ac⁃ta Otolaryngol,2009,129(4):419-422.
27 Sleeks JP,Shea JJ,Pitzer FJ.Epitympanic Ossicular Fixation.Arch Otolaryngol,1967,85:63-75.
28 Ritter FN.The Histopa thology of the Congenital Fixed Malleus Syndrome.Laryngoscope,1971;81:1304-1313.
29 Raz Y,Lustig L.Surgical Management of Conductive Hearing Loss in Children.Otolaryngol.Clin North Am. 2002,35(4):853-875.Review.
30 Mukerji SS,Parmar HA,Ibrahim M,et al.Congenital Malforma⁃tions of the Temporal Bone.Neuroimaging Clin N Am,2011,21(3):603-619.
31 邹艺辉.耳的胚胎发育[J].中华耳科学杂志.2014,12(4):537-539.Zuo YH.The Embryonic Development of the Ear.Chinese Journal ofOtology,2014,12(4):537-539.
32 杨凤,宋任东,刘阳.传导性耳聋合并鼓室段面神经畸形病例的听力重建技术.中华医学杂志,2016,96(5):384-383.Yang F,Song RD,Liu Y.The Technique of Hearing Reconstruc⁃tion in the Cases of Conductive Hearing Loss with Malformed Tympanic Segment of Facial Nerve.Natl Med JChina,2016,96(5):384-383.
33 Nandapalan V,Tos M.Isolated Congenital Stapes Ankylosis:An Embryologic Survey and Literature Review.Am JOtol,2000,21:71–80.
34 Lambert PR.Congenital Absence of the OvalWindow.Laryngo⁃scope,1990,100(1):37-40.
35 Bachor E1,Just T,Wright CG,et al.Fixation of the Stapes Foot⁃plate in Children:A Clinical and Temporal Bone Histopatholog⁃ic Study.Otol Neurotol,2005,26(5):866-873.
36 Su Y,Yuan H,Song YS,et al.Congenital Middle Ear Abnormali⁃ties with Absence of the Oval Window:Diagnosis,Surgery,and Audiometric Outcomes.Otol Neurotology,2014,35:1191-1195.
37 De Alarcon A,Jahrsdoerfer RA,Kesser BW.Congenital Ab⁃sence of the Oval Window:Diagnosis,Surgery,and Audiomet⁃ric Outcomes.OtolNeurotol,2008,29(1):23-28.
38 Zeifer B,Sabini P,Sonne J.Congenital Absence of the OvalWin⁃dow:Radiologic Diagnosis and Associated Anomalies.AJNR Am JNeuroradiol,2000,21(2):322-327.
39 杨凤,刘阳.先天性前庭窗及相关结构畸形的影像诊断及个性化手术.中华耳科学杂志.2015,13(1):120-125.Yang F,Liu Y.Congenital Malformation of the Oval Window and Related Structure:Experience of Radiologic Diagnosis and Surgi⁃cal Treatment.Chinese Journal of Otology,2015,13(1):120-125.
40 Yang F,Liu Y,Sun J,et al.Congenital Malformation of the Oval Window:Experience of Radiologic Diagnosis and Surgical Tech⁃nique.Eur Arch Otorhino laryngol,2016,273(3):593-600.
41 迟放鲁,王正敏,梁琴先天性无综合征听骨畸形与听骨链重建.中华耳鼻咽喉头颈外科杂志.2003,38(5):329-331.Chi FL,Wang ZM,Liang Q.Ossicular Deformity without Syndrome and Ossiculoplasty. Chin J Otorhinolaryngol,2003,38(5):329-331.
42 Liu Y,Yang F.Scala Tympani Drill-out Technique for Oval Win⁃dow Atresia with Malformed Facial Nerve:A Report of Three Cas⁃es.Journal of Otology,2015(10):154-158.
43 巍臣义,赵守琴.先天性外中耳畸形听力植入技术研究进展.中华耳科学杂志,2016,14(6):833-836.Wei CY,Zhao SQ.Progress in Research on Hearing Implants in Congenital Malformation of External and Middle Ear.Chinese Journal of Otology,2016,14(6):833-836.
44 Yang SM,Zou YH,Li JN.Vibrant Sound bridge Implantation via the Third Window in Two Chinese Patients with Severe Bilat⁃eral Congenital Aural Atresia.Acta Otolaryngol,2014,134(1):-6.
45 Zhao S,Gong S,Han D.Round Window Application of an Ac⁃tive Middle Ear Implant(AMEI)System in Congenital Oval Win⁃dow Atresia.Acta Otolaryngol,2016;136(1):23-33.
