Age-related changes of lens thickness and density in different age phases
2022-10-24YinHaoWangJingZhongXueMinLi
Yin-Hao Wang, Jing Zhong, Xue-Min Li
1Department of Ophthalmology, Peking University Third Hospital, Beijing 10091, China
2Beijing Key Laboratory of Restoration of Damaged Ocular Nerve, Peking University Third Hospital, Beijing 10091, China
3Education Department, Peking University Third Hospital,Beijing 10091, China
Abstract
● KEYWORDS: lens thickness; lens density; age; staged growth
INTRODUCTION
The lens is an important part of the eye and its physiological changes have a great impact on biological parameters of the eye[1-2]. With the changes of ocular parameters, various vision-threatening ocular disorders may occur, such as presbyopia, dysfunctional lens syndrome,cataract, and angle-closure glaucoma[3].
Age-related lens thickness changes were most studied, which can influence the chamber space. The thickness of the lens was simply thought to increase linearly with age in some studies[4-6].In recent years, more and more studies have pointed out staged changes in lens growth. Martinez-Enriquezet al[7]found the lens thickness decreased with age in the first two decades of life and then increased after age 20y. Similarly, Augusteyn[8]concluded lens thickness decreased from birth and thickened in late adolescence by analyzing data from a number of studies.This means that the lens thickness changes with age are not clear.
Lens density changes are greatly associated with ocular refractive status. Nevertheless, studies on changes in lens density with age were few and inconsistent. Kashimaet al[5]described positive associations of densities of anterior cortex,nucleus and posterior cortex with age. In contrast, another study demonstrated that posterior cortical lens density was negatively correlated with age, and that anterior cortical lens density changed little in different age groups[9]. Therefore, it has not reached a consensus that how the lens changes with age. Some studies intended to explore the lens changes with agein vitro[7,10-11], but this is not the same as the physiology of the lensin vivo. For studiesin vivo, the sample size was not enough[4,12].
Therefore, anin vivostudy with large sample size is meaningful for us to clearly figure out the age-related changes of lens. This can help us understand the lens-associated changes of ocular system with age, such as ocular structure and refraction. We intended to use the IOL Master 700, a machine based on swept source optical coherence tomography (SSOCT), to investigate age-related lens changes in the thickness and density.
SUBJECTS AND METHODS
Ethical ApprovalThis research was approved by Peking University Third Hospital Medical Science Research Ethics Committee, which was adhered to the tenets of the Declaration of Helsinki. Informed consent was exempt.
SubjectsThis is a retrospective study that included 490 right eyes and 495 left eyes from 497 individuals. The inclusion criteria were as follows: 1) underwent IOL Master in Peking University Third Hospital between December 2019 and June 2021; 2) diagnosed with myopia, hyperopia, astigmatism,ametropia, dry eye, conjunctivitis. Patients with following problems were excluded: 1) pupil dilation and fixation loss; 2)glaucoma, uveitis, cataract, fundus disease, congenital ocular disorder, history of ocular trauma and surgery (diagnosed with medical records, anterior segment photography, fundus photos,B-scan, or OCT).
We collected gender, birth date, examination date, the axial length, the central corneal thickness, and the whole lens thickness (WLT) from IOL Master. Age was calculated with birth date and examination date. Anterior cortical lens thickness(ACLT), nuclear lens thickness (NLT), posterior cortical lens thickness (PCLT), the whole lens density (WLD), anterior cortical lens density (ACLD), nuclear lens density (NLD), and posterior cortical lens density (PCLD) were obtained through imaging processing software.
IOL MasterAll patients underwent IOL Master 700 (Carl Zeiss Meditec AG, Jena, Germany) without pupil dilation.Based on a long-range SS-OCT technique, IOL Master 700 achieves a maximal scan depth of 44 mm, covering almost the entire length of the eye axis, and scanning a longer range of structures[13-14]. Therefore, IOL Master is capable of generating images of full eye, where cornea, lens, and macular fovea can be observed (Figure 1A). Additionally, we use macular fovea to judge patient’s fixation. Images with fixation loss were excluded.
Image ProcessingLens images were exported from IOL Master 700. We divided the lens into three parts, including anterior lens cortex, lens nucleus, and posterior lens cortex(Figure 1A). Two investigators independently marked the border line among the different parts of lenses. Disagreements were resolved by consensus. When the border lines were ambiguous to plot, we only measure the whole lens density and thickness. GetData Graph Digitizer 2.26 (http://getdata-graphdigitizer.com/) was used to measure thickness and Image-Pro Plus 6.0 (Media Cybernetics, Silver Spring, MD, USA) for density (Figure 1B-1E).

Figure 1 Measurement of the lens thickness and density A: The structure of lens; B: The anterior cortical lens density; C: The nuclear lens density; D: The posterior cortical lens density; E: The whole lens density.
Statistical AnalysisThe R version statistical package 4.1.0 and SPSS 26.0 (SPSS Inc., Chicago, IL, USA) were used for the statistical analysis. In our study, eight regression models were performed to explore the associations of lens thickness and density with age, including linear regression model, quadratic regression model, cubic regression model, quartic regression model, quintic regression model, piecewise regression model,spline regression model, and general addictive model. We compared models based on the adjustedR2, residual standard error (RSE) and clinical understandability, and thereafter chose models for these associations. The higher the adjustedR2was or the smaller the RSE was, the better the model fit. ThePvalue <0.05 was considered as statistical significance. The Chisquare test and Kruskal-WallisHtest were used to compare differences among age groups.
RESULTS
A total of 497 people with 490 right eyes and 495 left eyes were included. There were 265 females and 232 males ageing from 3 to 69 years old. Figure 2 showed the age and gender distribution. No significant difference was found in gender distribution among all age groups (P=0.940). There was no significant difference in central corneal thickness between different age groups (right eyes,P=0.756; left eyes,P=0.855).For people aging from 18 to 50 years old, we divided them into several groups based on age, including 18-20, 21-25, 26-30, 31-35, 36-40, 41-45, and 46-50 years old. No significantdifference was found (right eyes,P=0.757; left eyes,P=0.889)in axial length. The parameters of lenses were listed in Table 1.Lens ThicknessEight regression models were used to demonstrate the association between lens thickness and age in year (Table 2). Except for the WLT, piecewise regression model was the most suitable for describing lens thickness changes with age. Generalized additive model was most suitable for the WLT (adjustedR2=0.623), whereas it was difficult to understand and apply. Therefore, piecewise regression model was chosen with a slightly lower adjustedR2(0.619) for the whole lens thickness. Figure 3 illustrated the piecewise regression models of right lens thickness with age.The equation of right lens thickness (mm) and age (y) were shown as follows:

Table 1 Lens parameters among different age groups mean±SD

Table 2 Regression models between right lens thickness and age in year

Figure 2 Age and gender distribution.

The regression models for the association of left lens thickness with age were similar to the right lens thickness.

Figure 3 Lens thickness changes of right eyes through age A: The association between the whole central lens thickness and age; B: The association between the anterior cortical lens thickness and age; C: The association between the nuclear lens thickness and age; D: The association between the posterior cortical lens thickness and age. Blue lines represent the piecewise regression results, and red lines represent the linear regression results.

Table 3 Regression models between right lens density and age in year
Lens DensityEight regression models were used to demonstrate the association between lens density and age in year (Table 3). Piecewise regression model was the most suitable for describing lens density changes with age except for the WLD of right eyes and the ACLD. By comparing the adjustedR2value, we found generalized additive model was the best for the WLD of right eyes. However, it was difficult to understand and apply without providing coefficients. Therefore,piecewise regression model was chosen with a slightly lower adjustedR2(0.675) for the WLD of right eyes. The ACLD did not fit well with any model, in which generalized additive model was the most suitable by a slight advantage (adjustedR2=0.207). The piecewise regression models of right lens density with age were shown in Figure 4. For the association of ACLD with age, we used piecewise regression model to show the tendency roughly. The equation of right lens density and age (y) were shown as follows:
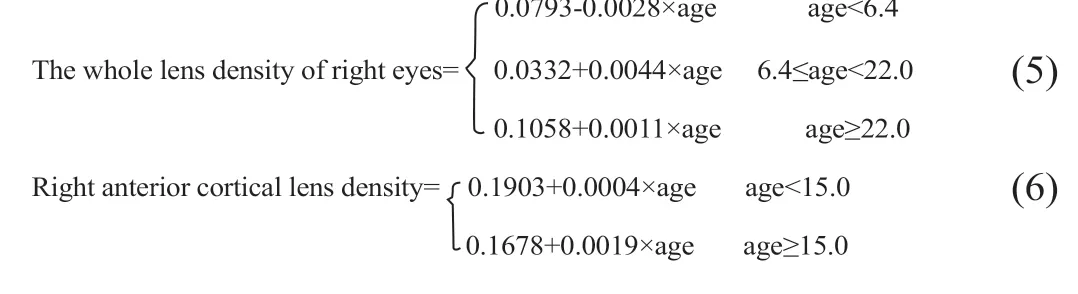

The regression models for the association of left lens density with age were similar to the right lens.
DISCUSSION
As lens is an important structure of the eye and greatly influences the intraocular environment, researchers have tried to clarify the growth tendency of the lens. While prior studies have shown different changing models in lens growth with small sample sizes[4,15], the exact changing patterns were not demonstrated in a larger population sample. In this 497-peopleincluded study, we found staged changes of lens thickness and density in different age phases through SS-OCT.

Figure 4 Lens density changes of right eyes through age A: The association between the whole lens density and age; B: The association between the anterior cortical lens density and age; C: The association between the nuclear lens density and age; D: The association between the posterior cortical lens density and age. Blue lines represent the piecewise regression results, and red lines represent the linear regression results.
In this study, we found that the changes of lens thickness with age were not simply linear. The whole lens thickness decreased with age before 7 years old, and then increased with age. Between the ages of 7 and 16, the lens thickness slowly increased at a rate of 0.0045 mm per year. After 16 years old, the growth rate of lens thickness was faster than before,increasing about 0.0265 mm per year. The WLT decreased with age after birth, which was similar to some studies[16-18]. This thinning is probably due to the remodeling and compaction of lens fibers, which occurs in both the nucleus and cortex primarily after birth[8]. In addition, the growing and expanding of the eye balls after birth exert a stretching force on the lens in the equatorial plane, making the lens thinner[19]. That is to say, the shape of the lens continues to change during the first decade of life, with equatorial diameter increasing at the expense of lens thickness[20]. Since the epithelial cells of the lens produce lens fibers throughout life, the lens thickness increases with age after a period of decline[21], which is consistent to our results.
However, the changing patterns of the cortical and nuclear thickness were not the same as the whole lens. After birth,anterior cortex, nucleus, and posterior cortex thinned together.At around 7-8 years old, the thickness of the lens cortex began to increase, whereas the nucleus continued thinning. Therefore,although the whole lens seemed to be stable between the ages of 8 and 16, the inner structures kept dynamic. It was probably due to the balance between nuclear compaction and cortical growth[20-22]. After 18 years old, lens cortex and nucleus showed stepwise increases accordantly. Lens cortex grows because of the production of lens fibers[21], while it is likely that nucleus thickens due to the movement of cortical fibrocytes towards the lens nucleus[1,23].
As shown in Figure 3, there was an apparent gap in the thickness of the lens cortex and nucleus between the ages of 10 and 14.In our study, we noticed that, for children from 10-14 years old, some had thickened lens cortex while others did not. It is possible that the cortical lens thickness has increased before this age, but SS-OCT is not accurate enough to detect it.Only if the difference in density is significant enough, can it be detected. The lens cortex is divided into four major zones called C1, C2, C3, C4 according to the Oxford system of lens zoning[24]. During the first decade of life, there are only two cortical zones, C1 and C2. Once the zone C3 is formed, there is little increase in its width[25], which explains why there is a gap in the thickness of the lens cortex between the ages of 10 and 14.In this study, the WLD and NLD decreased with age during the first 6-7y after birth. However, lens compaction occurs throughout life, and nuclear compaction develops most rapidly in young lenses[22], which theoretically increases the lens density. We assumed that this reduction may be resulted from the lens remodeling, making the lens structure much more regular and subsequently transparent[23]. Changes in lens proteins and lipids affect biological parameters of the lens,such as lens density. The proteins and lipids in the center of lenses change significantly with age, particularly between 40 and 50 years old[26]. However, in our study, lens density did not change significantly in fourth decade and later, and their lens density even tended to decrease. One possible explanation is that the sample size of patients after 40 years old was too small to explore the true association. It is also possible that those who have not developed cataracts after 45-50 years old[27]are more difficult to increase the lens density.
Patients without pupil dilatation were selected, because dilated pupil would stretch the lens at equatorial plane, which would have a great impact on thickness measurements in our study.Additionally, the normal pupil state was more conducive to the examination and positioning of its cornea and pupil center when using the IOL Master[28], so as to obtain more accurate measurement results. Theoretically, it is reasonable to make the patient’s lens at the maximum accommodation. In this case, the lens is in its most natural state due to the minimal external force[29]. However, it was difficult to get the patient’s lens at maximum accommodation, especially for the children.Furthermore, results based on eyes at natural status sometimes are more meaningful for application.
Compared with the previous studies[4,15], our study had a larger sample size, and we explored the lens thickness and density in the younger children. Age-dependent changes in the thickness and density of lens cortex, nucleus, and the whole lens were investigated in our research, which were little studied before.In addition, we compared the adjustedR2values to select a more appropriate model rather than the linear model. However,the study also had some limitations. In children before 18 years old, the axial length increases with growth. Therefore, it is different to match the axial length between the age groups of <18 years old and ≥18 years old. Axial length gradually increased with age roughly in patients before 18 years old.However, our results showed that the lens thickness did not increase continuously with age, which was not accordance to the changing tendency of axial length. In fact, because the results originated fromin-vivoobservation, all effects of agerelated changes in ocular structure on lens thickness were included. This was one of the advantages of our study, which reflected the real changes of the lens during individual growth and development. The axial length was smaller in patients over 50 years old than those in other groups. This was probably due to the limited number of patients over 50 years old. The number of participants decreased significantly after the age of 45, because it was difficult to find patients with completely normal lenses at this age, which may lead to inaccurate results in this age group. In the images of some younger patients, a small area with increased density, which was thought to be caused by reflection, was seen behind the anterior cortex.Although the reflective area was excluded from the density measurement, errors in density measurements occurred inevitably. Moreover, there are many other factors correlated with lens thickness, including gender, body mass index, central corneal thickness, axial length, hyperopic refractive error,cigarette smoking and diabetes[17,30-31]. Our study only focused on age and did not explore other factors, which needed to be further explored in the future.
In summary, we explored the relationship between lens thickness, density, and age by measuring the normal values of lens thickness and density. We collected 497 patients’ data to show that both the WLT and WLD decreased with age before 7 years old and increased after then. Our study confirmed that the lens thickness and density did not show a simple linear relationship with age. As we all known, it is important to understand the changes of biological parameters of the lens with age for early identification of some diseases of the lens,such as age-related cataract. In the future, measurements of the lens thickness and density may be used as a predictor of lens disease.
ACKNOWLEDGEMENTS
Authors’ contributions:Wang YH: designed the experiment,conducted the experiment, analyzed, and interpreted data,proofed, and revised the article; Zhong J: conducted the experiment, analyzed, and interpreted data, wrote the article;Li XM: designed the experiment, provided materials, proofed,and revised article.
Foundation:Supported by the National Science Foundation of Beijing Municipality (No.7202229).
Conflicts of Interest:Wang YH,None;Zhong J,None;Li XM,None.
杂志排行

International Journal of Ophthalmology的其它文章
- Lacrimal sac lymphoma: a case series and literature review
- Therapeutic potential of pupilloplasty combined with phacomulsification and intraocular lens implantation against uveitis-induced cataract
- Prophylaxis with intraocular pressure lowering medication and glaucomatous progression in patients receiving intravitreal anti-VEGF therapy
- Optimal timing of preoperative intravitreal anti-VEGF injection for proliferative diabetic retinopathy patients
- Prognosis value of Chinese Ocular Fundus Diseases Society classification for proliferative diabetic retinopathy on postoperative visual acuity after pars plana vitrectomy in type 2 diabetes
- Visual field defects and retinal nerve fiber layer damage in buried optic disc drusen: a new insight