生长抑素预防ERCP术后胰腺炎及高淀粉酶血症有效性的Meta分析
2021-04-29林秋满邱萍徐林芳龚敏文萍文剑波李兴王桂良
林秋满 邱萍 徐林芳 龚敏 文萍 文剑波 李兴 王桂良

[摘要] 目的 對应用生长抑素预防内镜逆行胰胆管造影(ERCP)术后胰腺炎(PEP)和ERCP术后高淀粉酶血症(PEHA)的研究进行Meta分析。 方法 搜索电子数据库,包括PubMed、EMBASE、Cochrane图书馆和科学引文索引以检索相关试验。纳入比较生长抑素和空白对照预防PEP的对照试验。使用随机效应模型和固定效应模型进行Meta分析以评估PEP、PEHA和ERCP术后腹痛的比率。 结果 生长抑素组PEP和PEHA比率均明显低于空白对照组(RR=0.45,95%CI:0.33~0.61,P<0.00001;RR=0.51,95%CI:0.39~0.67,P<0.00001)。对于短时间注射亚组,生长抑素组与空白对照组之间的PEP和PEHA比率比较,差异无统计学意义(RR=0.49,95%CI:0.22~1.11,P=0.09;RR=0.88,95%CI:0.450~0.172,P=0.71)。对于长时间注射亚组,生长抑素组的PEP和PEHA比率明显低于空白对照组(RR=0.43,95%CI:0.31~0.59,P<0.00001;RR=0.51,95%CI:0.30~0.69,P<0.00001)。对低危PEP亚组,生长抑素组与空白对照组PEP比率比较,差异无统计学意义(RR=0.60,95%CI:0.37~0.97,P=0.96);对于高危PEP亚组,生长抑素组PEP比率显著低于空白对照组(RR=0.62,95%CI:0.41~0.93)。对于长时间注射高风险PEP亚组,生长抑素组的PEP比率明显低于空白对照组(RR=0.54,95%CI:0.34~0.86,P=0.01)。生长抑素组的ERCP术后腹痛总发生率明显低于空白对照组(RR=0.60,95%CI:0.33~1.10,P=0.01)。PEP发病率的漏斗图显示没有不对称性和负斜率。结论 长时间注射生长抑素可以显著降低高风险患者PEP、PEHA和ERCP后腹痛的发生率,而对于低风险患者则无需使用。
[关键词] 内镜逆行胰胆管造影;生长抑素;胰腺炎;高淀粉酶血症
[中图分类号] R657.3 [文献标识码] A [文章编号] 1673-9701(2021)06-0001-09
Meta analysis of the effectiveness of somatostatin in preventing pancreatitis and hyperamylasemia after ERCP
LIN Qiuman QIU Ping XU Linfang GONG Min WEN Ping WEN Jianbo LI Xing WANG Guiliang
Department of Gastroenterology, Pingxiang Hospital Affiliated to Southern Medical University, Pingxiang 337000, China
[Abstract] Objective To conduct a meta-analysis of somatostatin in preventing post-endoscopic retrograde cholangiopancreatography pancreatitis(PEP) and post-endoscopic retrograde cholangiopancreatography hyperamylasemia (PEHA). Methods The electronic databases, including PubMed, EMBASE, Cochrane Library, and Science Citation Index, were searched to retrieve relevant experiments. A controlled trial comparing somatostatin and blank control to prevent PEP was included. Random effects model and fixed effects model were used for meta-analysis to evaluate the rate of abdominal pain after PEP, PEHA, and ERCP. Results The ratios of PEP and PEHA in the somatostatin group were significantly lower than those in the blank control group(RR=0.45, 95%CI: 0.33-0.61, P<0.00001; RR=0.51, 95%CI: 0.39-0.67, P<0.00001). For the short-term injection subgroup,there was no statistical difference between the ratios of PEP and PEHA between the somatostatin group and the blank control group(RR=0.49, 95%CI: 0.22-1.11, P=0.090; RR=0.88, 95%CI: 0.450-0.172, P=0.71). For the long-term injection subgroup, the ratio of PEP and PEHA in the somatostatin group was significantly lower than that of the blank control group(RR=0.43, 95%CI: 0.31-0.59, P<0.00001; RR=0.51, 95%CI: 0.30-0.69, P<0.00001). For the low-risk PEP subgroup, there was no significant difference in the PEP ratio between the somatostatin group and the blank control group (RR=0.60, 95%CI: 0.37-0.97, P=0.96). For the high-risk PEP subgroup,the PEP ratio of the somatostatin group was significantly lower than that of the blank control group(RR=0.62, 95%CI: 0.41-0.93). For the long-term injection of the high-risk PEP subgroup, the PEP ratio of the somatostatin group was significantly lower than that of the blank control group(RR=0.54, 95%CI: 0.34-0.86, P=0.01). The total rate of abdominal pain after ERCP in the somatostatin group was significantly lower than that of the blank control group(RR=0.60, 95%CI: 0.33-1.10, P=0.01). The funnel chart of the incidence of PEP showed no asymmetry or negative slope. Conclusion Long-term injection of somatostatin can significantly reduce the incidence of abdominal pain after PEP, PEHA and ERCP in high-risk patients, but it is not necessary for low-risk patients.
[Key words] Endoscopic retrograde cholangiopancreatography; Somatostatin; Pancreatitis; Hyperamylasemia
内镜逆行胰胆管造影(Endoscopic retrograde cholangiopancreatography,ERCP)是一项发展很快的重要的诊断与治疗技术,可用于胆总管结石、胆道肿瘤、胆管狭窄、胰腺癌等疾病的诊断和治疗,具有创伤小、术后恢复快、疗效可靠等优点,其主要并发症是腹痛、腹胀、术后胰腺炎(Post-ERCP pancreatitis,PEP)、高淀粉酶血症、胆管炎、脓毒血症、消化道出血和十二指肠穿孔等,其中PEP是最为常见的并发症,如何预防PEP是临床工作者的一项重要研究课题[1]。预防PEP的主要药物有非甾体类抗炎药物(吲哚美辛、双氯芬酸和布洛芬等)和蛋白酶抑制剂(生长抑素、乌司他丁、奥曲肽、加贝酯和奈莫司他等),生长抑素是这类药物中最为广泛应用,能抑制胰腺外分泌功能,减少胃泌素及缩胆囊素分泌[2]。但在国内外应用生长抑素抑制PEP的临床研究中,得出的结论不一致。本研究运用循证医学方法,对已报道的国内外应用生长抑素抑制PEP的文献进行Meta分析,为预防ERCP术后并发症提供理论证据,现报道如下。
1 资料与方法
1.1 文献纳入与排除标准
纳入标准:(1)将患者分为两组,生长抑素组和空白对照组;(2)患者接受ERCP;(3)该研究至少报道了以下结果指标之一:PEP、PEHA或ERCP后腹痛。排除标准:(1)非随机对照性研究设计;(2)临床病例报告及缺乏空白对照组的单组研究;(3)缺乏必要数据的研究。
1.2 文献检索策略
通过计算机检索PubMed、OVID、Cochrane library、EBSCO、Embase、Web of Science、中国知网、万方数据库,检索相关参考文献。相关文献检索词为:“somatostatin” “post-ERCP pancreatitis”“endoscopic retrograde cholangiopancreatography” “ERCP”“Hyperamylasemia”“生长抑素”“ERCP术后胰腺炎”“内镜逆行胰胆管造影”“高淀粉酶血症”。
1.3 文献质量评价及数据提取
所纳入的文献通过两名研究者对文献的偏倚风险进行评估,并且对不相一致的结果进行复查,若存在争议则通过讨论方式解决。对偏倚风险采用Cochrane系统评价手册进行评估。由两名研究者交叉核对所需数据资料,并且通过第三名研究者对分歧进行评判。所提取的文献内容包括第一作者、第一作者所属国家、研究发表时间、研究对象的病例数、性别、年龄、采用的干预方法、结果、退出或失访的患者等。基于以下两个因素进行亚组分析:(1)生长抑素输注模式,包括推注(单次剂量生长抑素0.25 mg或4 μg/kg静脉注射);短时间注射(生长抑素0.25 mg/h,滴注或泵静脉注射<4 h);长时间注射(生长抑素0.25 mg/h,滴注或泵静脉注射≥4 h);(2)PEP风险水平,包括高风险PEP(①Oddi括约肌障碍;②近期发生过急性胰腺炎;③预切口括约肌切开术;④插管次数≥3次;⑤胰管注射)和低风险PEP(无上述高风险PEP因素)[3]。
1.4 统计学处理
所获取的数据通过Review Manager 5.3统计学软件进行整理和分析。其中的计数资料统计量通过风险比(Risk ratio,RR)进行分析,95%置信区间(Confidenceinterval,CI)表示区间估计。对异质性采用χ2检验进行检验,P<0.1时,表示研究结果之间有异质性,对异质性大小采用I2定量进行分析。I2≤50%时,采用固定效应模型分析。I2>50%时,采用随机效应模型分析。以Egger检验和漏斗图分析潜在的发表偏倚。以α=0.05作为检验水准,P<0.05为差异有统计学意义。
2 结果
2.1 文献检索结果及纳入文献的基本特征
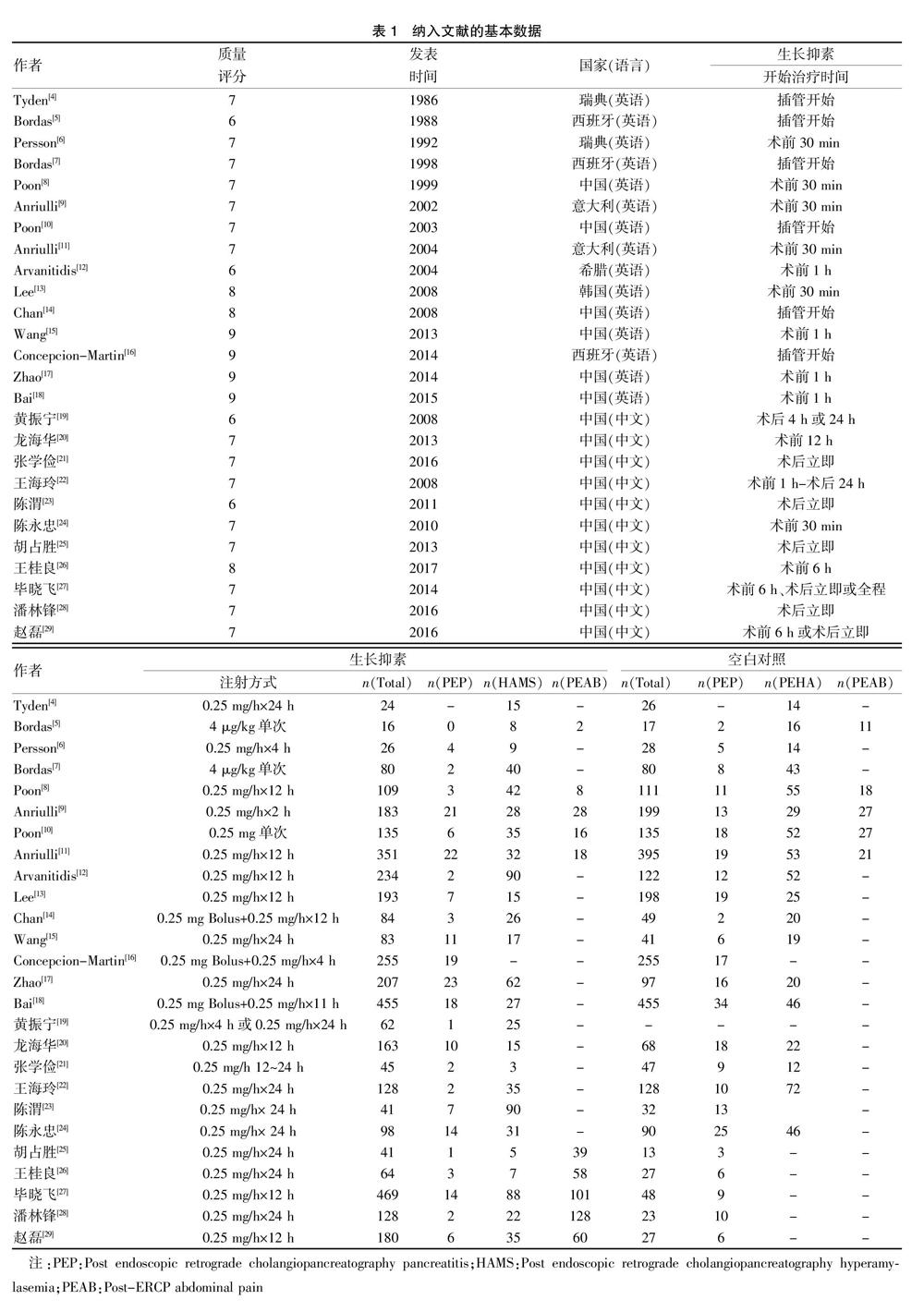
通过计算机检索,共有1590篇相关文献被纳入本研究,排除1344篇不符合纳入标准的文献,包括重复性论文、非随机对照研究(RCT)论文和Meta分析论文,得到246篇相关文献,在排除220篇不符合要求的文献,包括非空白对照与生长抑素对比的论文、联用了其他药物和动物实验的文献,最后纳入26篇文献[4-29]。文献内容涉及患者共6764例,其中3827例为生长抑素组,2937例为空白对照组。所纳入文献的基本特征及质量评价见图1、表1。
2.2 Meta分析结果
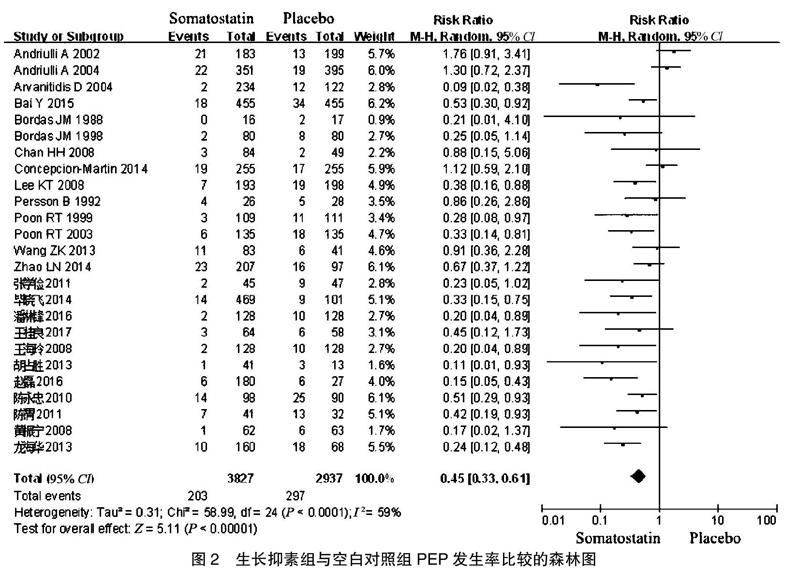
2.2.1 生长抑素与空白对照组总PEP发生率比较 生长抑素组PEP发生率为5.3%,空白对照组PEP发生率为10.1%,研究之間存在异质性(P<0.001,I2=59%),采用随机效应模型进行检验。与空白对照组相比,生长抑素组PEP发生率显著降低(RR=0.45,95%CI:0.33~0.61,P<0.0001)。见图2。
2.2.2 注射方式亚组分析生长抑素与空白对照组比较的PEP发生率 根据给药方式和剂量,将纳入患者进一步分为长时间注射亚组(静脉滴注或泵入时间≥4 h)、短时间注射亚组(一次性静脉推注,滴注或泵入时间<4 h)。Meta分析结果显示,长时间注射亚组各研究间无异质性(P=0.002,I2=55%),采用随机效应模型进行检验。与空白对照组比较,长时间注射生长抑素可显著降低PEP发生率,组间比较,差异有统计学意义(RR=0.43,95%CI:0.31~0.59,P<0.0001);短时间注射亚组各研究间有异质性(P=0.005,I2=68%),采用固定效应模型检验。与空白对照组比较,短时间注射生长抑素不能降低PEP发生率,组间比较,差异无统计学意义(RR=0.49,95%CI:0.22~1.11,P=0.09)。见图3。
本研究的不足之處在于:(1)纳入的文献数量不多,将研究对象细分为高风险亚组和低风险亚组的文献不多,部分文献质量不高;(2)分析ERCP术后腹痛的文献不多。上述的因素可能在一定程度上影响了本项研究的可靠性。因此,尚且需要更多的随机对照研究证明本研究结果的稳定性。
[参考文献]
[1] S?覬reide JA,Karlsen LN,Sandblom G,et al.Endoscopic retrograde cholangiopancreatography(ERCP):Lessons learned from population-based national registries:A systematic review[J]. Surg Endosc,2019,33(6):1731-1748.
[2] Testoni PA.Somatostatin:Still a pharmaceutical defense weapon against post-ERCP pancreatitis? A 30-year story[J].Endoscopy,2015,47(5):393-395.
[3] Dumonceau JM,Andriulli A,Elmunzer BJ,et al.Prophylaxis of post-ERCP pancreatitis:European society of gastrointestinal endoscopy(ESGE) guideline-updated June 2014[J].Endoscopy,2014,46(9):799-815.
[4] Tydén G,Nyberg B,Sonnenfeld T,et al.Effect of somatostatin on hyperamylasemia following endoscopic pancreatography[J].Acta Chir Scand Suppl,1986,530:43-45.
[5] Bordas JM,Toledo V,Mondelo F,et al.Prevention of pancreatic reactions by bolus somatostatin administration in patients undergoing endoscopic retrograde cholangio-pancreatography and endoscopic sphincterotomy[J].Horm Res,1988, 29(2-3):106-108.
[6] Persson B,Slezak P,Efendic S,et al.Can somatostatin prevent injection pancreatitis after ERCP?[J].Hepatogastroenterology,1992,39(3):259-261.
[7] Bordas JM,Toledo-Pimentel V,Llach J,et al.Effects of bolus somatostatin in preventing pancreatitis after endoscopic pancreatography:Results of a randomized study[J].Gastrointest Endosc,1998,47(3):230-234.
[8] Poon RT,Yeung C,Lo CM,et al.Prophylactic effect of somatostatin on post-ERCP pancreatitis:A randomized controlled trial[J].Gastrointest Endosc,1999,8(5):593-598.
[9] Andriulli A,Clemente R,Solmi L,et al.Gabexate or somatostatin administration before ERCP in patients at high risk for post-ERCP pancreatitis:A multicenter,placebo-controlled,randomized clinical trial[J].Gastrointest Endosc,2002,51(4):488-495.
[10] Poon RT,Yeung C,Liu CL,et al.Intravenous bolus somatostatin after diagnostic cholangiopancreatography reduces the incidence of pancreatitis associated with therapeutic endoscopic retrograde cholangiopancreatography procedures:A randomised controlled trial[J].Gut,2003, 52(12):1768-1773.
[11] Andriulli A,Solmi L,Loperfido S,et al.Prophylaxis of ERCP-related pancreatitis:A randomized,controlled trial of somatostatin and gabexate mesylate[J].Clin Gastroenterol Hepatol,2004,2(8):713-718.
[12] Arvanitidis D,Anagnostopoulos GK,Giannopoulos D,et al.Can somatostatin prevent post-ERCP pancreatitis? Results of a randomized controlled trial[J].J Gastroenterol Hepatol,2004,19(3):278-282.
[13] Lee KT,Lee DH,Yoo BM.The prophylactic effect of somatostatin on post-therapeutic endoscopic retrograde cholangiopancreatography pancreatitis:A randomized,multicenter controlled trial[J].Pancreas,2008,37(4):445-448.
[14] Chan HH,Lai KH,Lin CK,et al.Effect of somatostatin in the prevention of pancreatic complications after endoscopic retrograde cholangiopancreatography[J].J Chin Med Assoc,2008,71(12):605-609.
[15] Wang ZK,Yang YS,Cai FC,et al.Is prophylactic somatostatin effective to prevent post-endoscopic retrograde cholangiopancreatography pancreatitis or hyperamylasemia? A randomized,placebo-controlled pilot trial[J].Chin Med J (Engl),2013,126(13):2403-2408.
[16] Concepcion-Martin M,Gomez-Oliva C,Juanes A,et al.Somatostatin for prevention of post-ERCP pancreatitis:A randomized,double-blind trial[J].Endoscopy,2014,46(10):851-856.
[17] Zhao LN,Yu T,Li CQ,et al.Somatostatin administration prior to ERCP is effective in reducing the risk of post-ERCP pancreatitis in high-risk patients[J].Exp Ther Med,2014,8(2):509-514.
[18] Bai Y,Ren X,Zhang XF,et al.Prophylactic somatostatin can reduce incidence of post-ERCP pancreatitis:Multicenter randomized controlled trial[J].Endoscopy,2015,47(5):415-420.
[19] 黃振宁,陶霖.生长抑素及其类似物在预防胆总管结石内镜逆行胰胆管造影术后胰腺炎中的作用[J].内科,2008(5):707-708.
[20] 龙海华,梁秀兰,刘振鹏,等.生长抑素预防ERCP术后并发症的价值[J].现代消化及介入诊疗,2013(2):108-109.
[21] 张学俭.胆总管取石术后并发胰腺炎患病率及不同药物预防效果的调查分析[J].现代消化及介入诊疗,2016(5):708-710.
[22] 王海玲,王云溪,段双霞.国产生长抑素预防ERCP术后胰腺炎的临床研究[J].中国医药指南,2008(19):60-61.
[23] 陈渭,黄文柱,智发朝.生长抑素预防逆行胰胆管造影术后胰腺炎的随机对照[J].广州医学院学报,2011(4):80-83,87.
[24] 陈永忠.生长抑素预防治疗性ERCP术后高淀粉酶血症及胰腺炎的临床观察[J].中国现代药物应用,2010,(12):162-163.
[25] 胡占胜,张健康.生长抑素在预防胆总管结石患者ERCP术后胰腺炎和高淀粉酶血症中的临床作用[J].中国现代医生,2013,51(25):28-30.
[26] 王桂良,邱萍,徐林芳,等.4种蛋白酶抑制剂预防胆总管结石患者ERCP术后高淀粉酶血症和胰腺炎的成本-效果分析[J].中国药房,2017(14):1880-1884.
[27] 毕晓飞,张俊文.不同时期使用生长抑素对预防ERCP术后胰腺炎及高淀粉酶血症的作用[J].重庆医学,2014(29): 3885-3886,3889.
[28] 潘林锋,张英杰,张国强,等.生长抑素对ERCP术后急性胰腺炎的预防作用研究[J].浙江医学,2016(17):1449-1450.
[29] 赵磊.不同时期应用生长抑素对预防ERCP术后胰腺炎及高淀粉酶血症的影响[J].中国医药指南,2016,(10):183.
[30] Desilets DJ. Management of post-ERCP complications[J]. Minerva Chir,2017,72(2):157-168.
[31] Andriulli A,Leandro G,Niro G,et al.Pharmacologic treatment can prevent pancreatic injury after ERCP:A meta-analysis[J]. Gastrointest Endosc,2000,49(1):1-7.
[32] Omata F,Deshpande G,Tokuda Y,et al.Meta-analysis:Somatostatin or its long-acting analogue,octreotide,for prophylaxis against post-ERCP pancreatitis[J]. J Gastroenterol,2010,45(8):885-895.
[33] Xie Q,Lei WS,Xing ZX,et al. Prophylactic effect of somatostatin in preventing post-ERCP pancreatitis:An updated meta-analysis[J]. Saudi J Gastroenterol,2015,21(6):372-378.
[34] 潘树波,耿小平.生长抑素预防内镜逆行胰胆管造影术 后胰腺炎效果的Meta分析[J]. 中华外科杂志,2016,54(3):466-472.
[35] Wang G,Xiao G,Xu L,et al.Effect of somatostatin on prevention of post-endoscopic retrograde cholangiopancreatography pancreatitis and hyperamylasemia:A systematic review and meta-analysis[J]. Pancreatology,2018, 18(4):370-378.
(收稿日期:2020-08-17)
