Proton pump inhibitors and adverse effects in kidney transplant recipients:A meta-analysis
2019-07-12BoonphiphopBoonphengCharatThongprayoonTarunBathiniKonikaSharmaMichaelMaoWisitCheungpasitporn
Boonphiphop Boonpheng,Charat Thongprayoon,Tarun Bathini,Konika Sharma,Michael A Mao,Wisit Cheungpasitporn
Abstract
Key words:Proton pump inhibitors;Kidney;Renal transplantation;Meta-analysis hypomagnesemia;Systematic reviews
INTRODUCTION
Proton pump inhibitors(PPIs)are commonly prescribed after transplantation for prophylaxis against peptic ulcer disease and for treatment of gastro-esophageal reflux disease or dyspepsia.Prolonged exposure to this class of medication has been shown to be associated with kidney dysfunction[1,2],as well as other non-renal adverse outcomes,including hypomagnesemia[3],fracture[4],or dementia[5]in the general population.The risk of kidney dysfunction associated with PPIs is particularly concerning to kidney transplant recipients who are already at risk for acute kidney injury.
Mycophenolate mofetil(MMF)is an antimetabolite that is commonly used as part of the maintenance immunosuppression in kidney transplant recipients[6].MMF is a prodrug that is hepatically metabolized to the active compound mycophenolic acid(MPA)after oral administration.MPA exerts its immunosuppressive effects by reversibly inhibiting the de novo synthesis of purine nucleotides,leading to reduced proliferation of B- and T-cell lymphocytes,induction of activated T lymphocyte apoptosis,and downregulation of adhesion molecule expression,resulting in lower leukocyte trafficking and recruitment[7].Because gastrointestinal discomfort is a common side effect of MMF,PPIs are commonly prescribed to alleviate the symptoms.However,pharmacokinetic studies[8-12]have shown that PPIs reduce the absorption of MMF and lower the exposure to MPA presumably by its potent inhibition of gastric acidification compared with another class of acid suppressant,the H2-receptor antagonists[13,14].Randomized controlled trials[15,16]and observational studies[17-19]have also shown that reduced exposure to MPA is associated with higher risk of acute rejection and overall worse allograft outcome in kidney transplant recipients.However,the clinical significance of this drug interaction in kidney transplant recipients is unknown.Several studies[20,21]have shown a possible increased risk of acute rejection with PPI exposure whereas others have not[22-24].
Some studies[25,26]have shown that concurrent PPI can increase tacrolimus drug concentration,leading to higher risk of toxicity through cytochrome or p-glycoprotein inhibition in patients with certain Cytochrome P450 2C19(CYP2C19)and/or CYP3A5 genotypes.However,this is not expected to increase the risk of rejection,but calcineurin inhibitor toxicity may lead to renal dysfunction.Other commonly used immunosuppressive drugs are not known to have significant interaction with PPIs.
PPI may also interfere with magnesium absorption in the gastrointestinal tract,causing hypomagnesemia[3].The mechanism of renal dysfunction related to PPIs is not clear although acute interstitial nephritis(AIN)associated with PPIs has been purposed[1,2].
Therefore,we conducted this systematic review and meta-analysis to investigate the adverse outcomes in kidney transplant recipients on PPI compared with those without PPI exposure.The outcomes of interest include biopsy-proven acute rejection,graft loss,kidney dysfunction,hypomagnesemia,and overall mortality.
MATERIALS AND METHODS
Search strategy
The protocol for this meta-analysis is registered with PROSPERO,No.CRD420-18115676.PRISMA statement guidelines were followed for conducting and reporting meta-analysis data[27].A systematic review was conducted in MEDLINE,EMBASE,and Cochrane databases from inception to October 2018 to identify studies that evaluated adverse effects of PPIs in kidney transplant recipients by using the search terms “kidney transplant” and “proton pump inhibitor,” as described in the online supplementary data without any language restriction.References of selected articles were also manually searched for additional studies.
Inclusion criteria
Studies were eligible for this meta-analysis if the following inclusion criteria were met:(1)Randomized controlled trial,cohort(either prospective or retrospective),case-control study or cross-sectional study published as an original study to evaluate the outcomes of kidney transplantation in patients on PPIs;(2)Odds ratios(ORs),relative risk(RR),hazard ratio(HR),and standardized incidence ratio(SIR)with 95%confidence intervals(CIs)or sufficient raw data to calculate these ratios were provided;and(3)Subjects not on PPIs were used as comparators in cohort and crosssectional studies.
Study eligibility was independently evaluated by the investigators(BB and CT).Any disagreement was resolved by mutual consensus.The quality of each study was appraised using the Newcastle-Ottawa quality scale[28].This scale assesses each study in three domains,including the:(1)Representativeness of the subjects;(2)Comparability between the study groups;and(3)Ascertainment of the exposure of interest for the case-control study and the outcome of interest for the cohort study.The modified version of the Newcastle-Ottawa scale as described by Herzoget al[29]was used for cross-sectional studies.
Review process and data extraction
The two study investigators independently reviewed the titles and abstracts of all retrieved articles.Articles that apparently did not fulfill the inclusion criteria were excluded.Only potentially relevant articles underwent full-text review to determine eligibility.A standardized data collection form was used to extract the following information from the included studies:First author’s name,year of publication,year of study,country where the study was conducted,study design,source of population,number of subjects,baseline characteristics of the subjects,and effect estimates.This data extraction process was performed by both investigators to ensure accuracy.
Statistical analysis
All statistical analyses were performed using Comprehensive Meta-analysis version 3 software(Eaglewood,NJ,United States).The pooled RRs of acute rejection,graft loss,hypomagnesemia,and overall mortality in kidney transplant recipients on PPIs compared with subjects not on PPIs were calculated using the generic inverse method of DerSimonian and Laird[30].The random-effects model was used,given the high likelihood of between-study variance due to the difference in underlying population and methodology.Cochran's Q-test,which was supplemented byI2statistics,was used to evaluate statistical heterogeneity.I2statistics quantify the proportion of the total variation across studies,that is,due to true heterogeneity rather than chance.AnI2value of 0% to 25% represents insignificant heterogeneity,>25% to≤50% represents low heterogeneity,>50% to≤75% represents moderate heterogeneity,and >75%represents high heterogeneity[31].
RESULTS
The initial search yielded 838 articles,all of which underwent title and abstract review(Figure 1).Most of the articles were excluded at this step because they were case reports,letters to the editor,review articles,or interventional studies,which clearly did not fulfill our inclusion criteria.Eighteen studies underwent full-length article review,and four were excluded because they did not include controls or did not report the outcome of interest.Therefore,14 studies met our inclusion criteria[20-24,32-40]and were included in the meta-analysis.The baseline characteristics of the included studies are summarized in Table 1.These 14 observational studies consisted of 6786 kidney transplant recipients(>1907 with PPI exposure and 2528 without PPI exposure).
Acute biopsy-proven rejection and graft loss
Table 2 summarizes the findings across the studies that reported allograft outcomes.Definitions of biopsy-proven acute rejection and presumed rejection across included studies are also shown in Supplementary Table S1.Pooled data for acute rejection at≥1 year were available from six studies with 2427 kidney transplant recipients(980 with PPI exposure and 1447 without PPI exposure).No significant association was found between PPI exposure and the risk of biopsy-proven acute rejection at≥1 year(pooled OR=1.25,95%CI:0.82-1.91,I2=55%,Figure 2).At 3 mo,acute rejection risk was also not significantly different between the two groups(pooled OR=1.54,95%CI:0.64-3.82).Acute cellular rejection was more common than antibody-mediated rejection(AMR)and the rejection rates were similar between the two groups,except in studies by Coursonet al[21]and Rouseet al[24]which demonstrated higher rates of AMR among the PPI group.The median time to rejection was reported to be similar between the two groups across four studies(approximately 3-4 mo post-transplant).Graft loss at 1 year was also not different between those with and without PPI exposure(pooled OR=1.30,95%CI:0.75-2.24,I2=0%,Figure 3).
Renal function
All but one study reported no significant short term(3 mo to 1 year)difference in renal function,as summarized in Table 3.Uludaget al[37],which had the most extended follow-up period of all included studies(median,109 mo;interquartile range,82-156 mo),however demonstrated that the serum creatinine level in the PPI group was higher than that in the non-PPI group(1.44 ± 0.99vs1.24 ± 0.46 mg/dL).
Hypomagnesemia
Table 4 summarizes data across eight studies.The risk of hypomagnesemia in the PPI group was significantly higher than in the non-PPI group(pooled OR=1.56,95%CI:1.19-2.05,I2=27%,Figure 4)based on three studies.Sezeret al[35],Van Endeet al[33],and Uludaget al[37]did not report a significant difference in the magnesium level between those with and without PPI exposure,whereas Alhosainiet al[34]reported a significant difference between the two groups(magnesium:1.70 ± 0.12vs1.79 ± 0.17 for those with PPI and without PPI exposure;P=0.006).Gomes-Netoet al[38]and Douweset al[40](who analyzed data from an overlapping set of patients)reported a significant inverse correlation between PPI use and plasma magnesium level.The proportion of hypomagnesemia also did not differ between the two groups,but a study by Shabakaet al[36]noted that those with PPI exposure seemed to develop significantly more severe hypomagnesemia(defined as magnesium level < 1.3 mg/dL)compared with those without PPI exposure(21%vs5%).
Overall mortality

Table 1 Characteristics of included studies

1Data expressed as mean ± SD;2Data expressed as Median(Range);3According to the NOS(Newcastle-Ottawa Scale)classification.NR:Not reported;CNI:Calcineurin inhibitor;MMF:Mycophenolate mofetil;MPS:Mycophenolate sodium;MPA:Mycophenolate;rATG:Rabbit antithymocyte globulin;PPI:Proton pump inhibitors.
All-cause mortality data were available from five studies(Table 5),with three studies reporting 1-year survival and two reporting longer-term all-cause mortality.One-year mortality did not significantly differ between PPI and non-PPI use(pooled OR=1.30,95%CI:0.51-3.29,I2=41.4%;Figure 5).The two studies that reported long-term mortality outcomes(Douweset al[40]and Gomes-Netoet al[38])seemed to analyze data from a highly overlapping set of patients(n=706vs703);hence,pooled HR was not calculated.With a median follow-up duration of 5.4 years(range,4.8-6.1 years)in both studies,the adjusted HRs for all-cause mortality was significantly associated with PPI use(HR=1.94,95%CI:1.32-2.88,and HR=2.01,95%CI:1.43-2.83,respectively).
Evaluation for publication bias
The funnel plots(Supplementary Figure S1 to Figure S4)and Egger’s regression asymmetry test were performed and showed no significant publication bias(P>0.05 for all outcomes).
Sensitivity analysis
Sensitivity analysis was performed by excluding one study at a time to investigate the effect of each study on the pooled OR for each outcome assessed.The pooled effect estimate from this sensitivity analysis remained essentially unchanged.
重蔬食:“吾谓饮食之道,脍不如肉,肉不如蔬,亦以其渐近自然也。”李渔认为“重蔬食”有益人体健康,应该发扬上古“重蔬食,远肥腻”的遗风,方能崇俭以养生。
DISCUSSION
This meta-analysis showed no significant association between exposure to PPIs and higher risk of acute biopsy-proven rejection,graft loss,or overall mortality,but a significantly higher risk of hypomagnesemia among those with PPI exposure was noted.No short-term difference in renal function was found between the two groups.
Despite several pharmacokinetic studies that have clearly showed significantly reduced MPA exposure following concomitant administration of PPIs and MMF in both healthy volunteers[12,41]and in immediate post-transplant kidney transplant recipients[10,11],there was no significant association between PPI use and increased risk of acute rejection in our study,suggesting that the effect may not be large enough to be clinically significant.Because none of the included studies reported MPA drug level or direct gastric pH measurement,it is difficult to ascertain whether a significant interaction between PPIs and MMF exists in the real-world setting.Three studies(van Boekelet al[22],Coursonet al[21],and Patelet al[23])reported the total cumulative MMF exposure or mean daily dose between the two groups.In all three studies,despite the PPI group receiving a slightly lower cumulative MMF dose compared to the non-PPI group(non-significant in the study by van Boekelet al[22]and Patelet al[23];significant in the study by Coursonet al[21]),no significant difference in acute rejection was found.Interestingly,in black patients,PPI was found to be significantly associated with a higher risk of acute rejection in one study[20].
Another potential reason for the lack of a significant association between PPI use and acute biopsy-proven rejection is that the majority of the kidney transplant recipients enrolled in the included studies were on tacrolimus,with none or only a small percentage of recipients on cyclosporine.The use of tacrolimus as the calcineurin inhibitor instead of cyclosporine may help lower the risk of reduced MPA exposure with PPI use.Cyclosporine,unlike tacrolimus,can reduce the enterohepatic recirculation of MPA in the gastrointestinal tract[42,43],thus further lowering total MPA exposure.The enteric-coated mycophenolate sodium does not appear to have a significant interaction with PPI[8,41,44],unlike MMF.
We did not demonstrate a significant difference in renal function as measured by estimated glomerular filtration rate or serum creatinine between the PPI and the non-PPI group in the short term(3 mo to 1 year).Extrapolating from observational studies in the general population,this is not unexpected as the risk of kidney dysfunction seems to be associated with more prolonged PPI use and may have a long latent period[1,45].Uludaget al[37]also confirmed this observation by noting a significantly higher serum creatinine level in PPI users compared with non-users at a longer median follow-up of 109 mo.
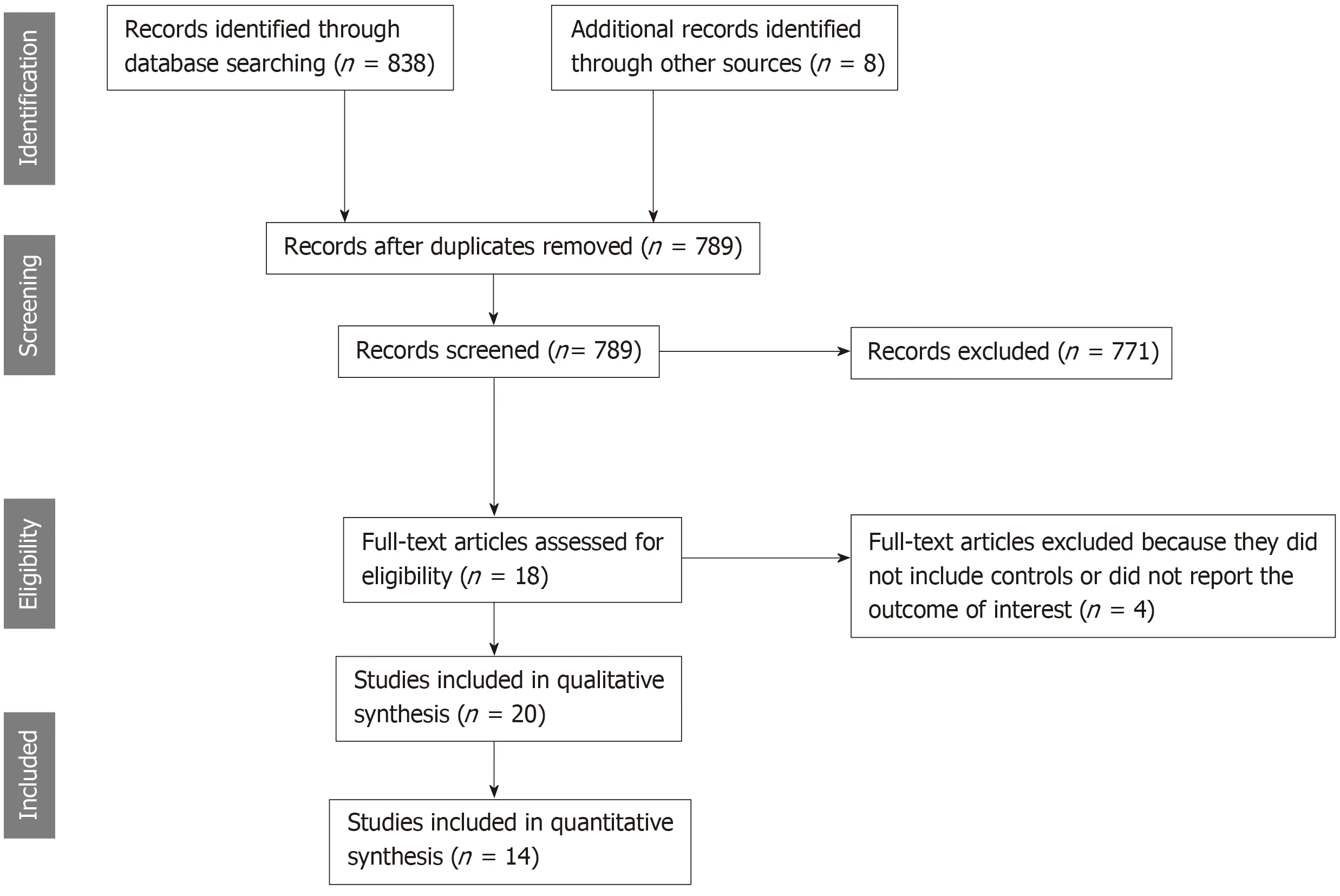
Figure 1 Study selection.
The risk of hypomagnesemia in the PPI group was significantly higher than that in the non-PPI group in our study.This is consistent with studies in the general population that report hypomagnesemia with prolonged PPI use[3].The exact mechanism of PPI-induced hypomagnesemia is unknown.Urinary magnesium excretion has been shown to be low in patients with hypomagnesemia related to PPI use[46],suggesting that reduced absorption from the gastrointestinal tract is the main cause.It is hypothesized that the TRMP6(transient receptor potential melastatin)pathway in gut epithelial cells,which mediates magnesium absorption,is inhibited by the high pH milieu caused by PPI use[47].This inhibition is more pronounced in certain individuals with additional polymorphisms of the related cellular pathway proteins or other risk factors,which explains why the incidence and degree of hypomagnesemia vary among PPI users[47].Some studies have also reported that high-dose oral magnesium supplementation can correct hypomagnesemia associated with PPI[48],suggesting that the paracellular passive absorption in the bowel remains intact.
In kidney transplant recipients,hypomagnesemia has been shown to be associated with various adverse consequences[49].Low magnesium level has been associated with accelerated decline of allograft function and a higher rate of graft loss in patients with cyclosporine-induced nephropathy[50],consistent with animal studies showing a higher degree of renal tissue fibrosis associated with low magnesium[51]that appears to be partially correctable with magnesium supplementation[51,52].Hypomagnesemia may also lead to a higher incidence of new-onset diabetes after transplant[53],which is a separate risk factor for allograft loss and overall mortality.
Our study did not show a significant difference in the 1-year overall mortality,as expected,because the risks of acute rejection,graft loss,and kidney dysfunction did not significantly differ between the PPI and non-PPI groups.Only hypomagnesemia was found to be significantly associated with PPI use;hence,this may not be clinically significant to drive a mortality difference at least in the short term.However,Douweset al[40]and Gomes-Netoet al[38]reported a significant association between PPI use and long-term all-cause mortality despite adjustment for confounders.Furthermore,both studies also showed a significant interaction between PPI use and hypomagnesemia.As noted previously,Uludaget al[37]has also reported significantly worse kidney function in the PPI group with longer follow-up(median,109 mo).Hypomagnesemia or renal dysfunction may be a late manifestation associated with prolonged exposure to PPIs,which may eventually be clinically significant enough to cause higher mortality.Further studies are needed to clarify this question.
Although we believe the literature review process was rigorous and the included studies were of high quality,this meta-analysis has some limitations.Therefore,the interpretation of the results needs to be performed with caution.First,this metaanalysis is based solely on observational studies.Although this is appropriate for our clinical question,it may be inherently subject to selection bias and unadjusted confounders.Second,certain important baseline characteristics could not be obtained or compared across all studies.Of interest to transplant recipients,comparison of different immunosuppressive regimens,drug level,dosage,and adherence to both immunosuppressive drugs or acid suppressive therapy between the two groups was not possible in most included studies due to either their observational or retrospective design.Third,the definitions of various outcomes of interest varied across studies,such as the cut-off value for hypomagnesemia,definition of severe rejection,or the use of different criteria for the classification of AMR and cell-mediated rejection.Finally,most of the included studies only reported follow-up data for a relatively short-term period(approximately 1 year).Therefore,we cannot rule out the possibility that prolonged exposure of PPIs(longer than a year)may lead to adverse outcomes.Further study is needed to address whether long-term PPI exposure in kidney transplant recipients is associated with worse outcomes.
In conclusion,PPI use was not associated with significant risks of higher acute rejection,graft loss,or 1-year mortality.However,the risk of hypomagnesemia was significantly increased with PPI use.
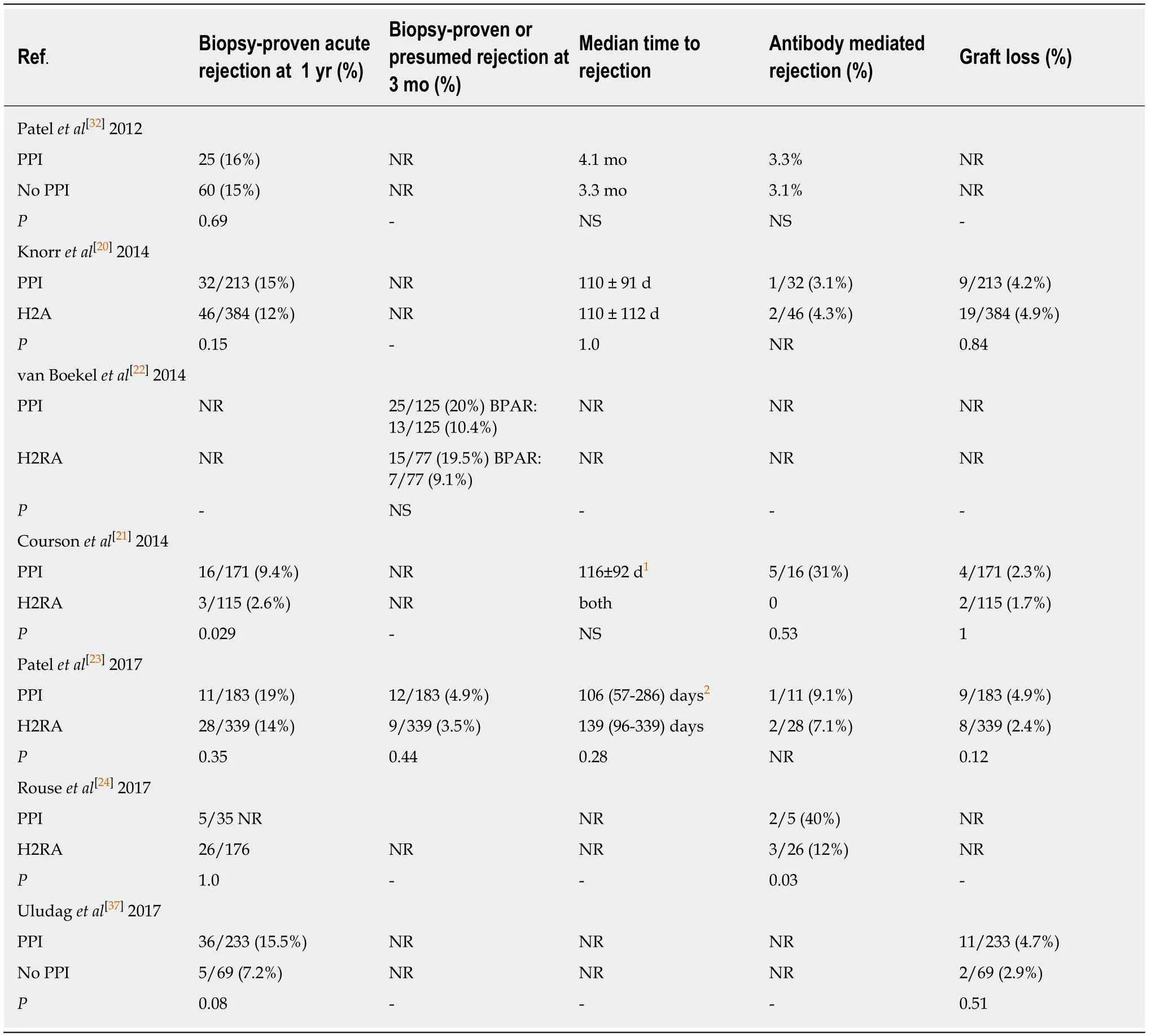
Table 2 Acute rejection and graft loss

Table 3 Renal function
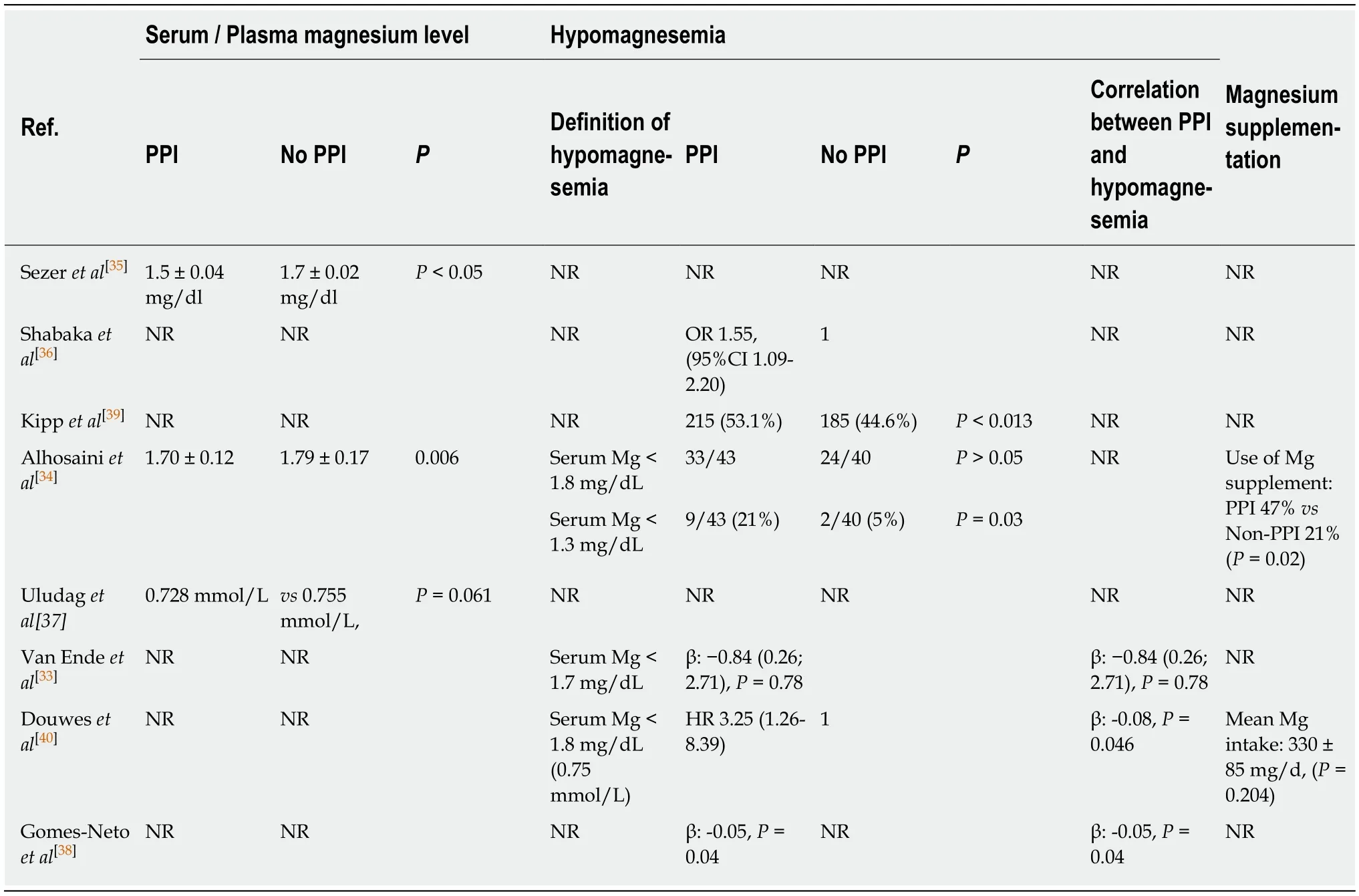
Table 4 Hypomagnesemia

Table 5 Mortality
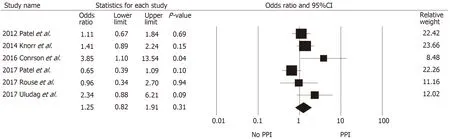
Figure 2 Forest plot of all included studies evaluating the risk of biopsy-proven rejection at one year or more in proton pump inhibitors users compared with non-users.
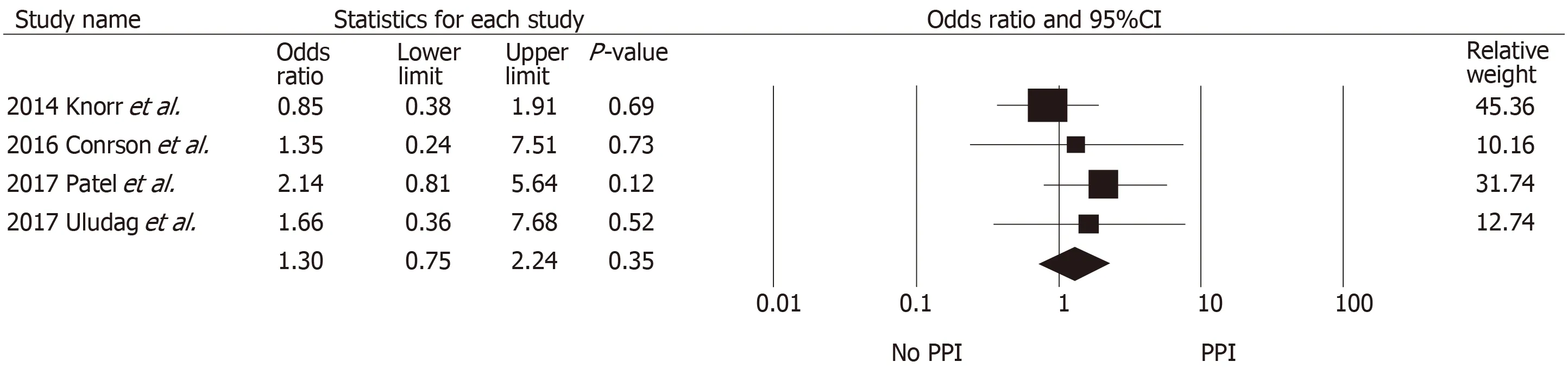
Figure 3 Forest plot of all included studies evaluating the risk of graft loss in proton pump inhibitors users compared with non-users.

Figure 4 Forest plot of all included studies evaluating the risk of hypomagnesemia in PPl users compared with non-users.
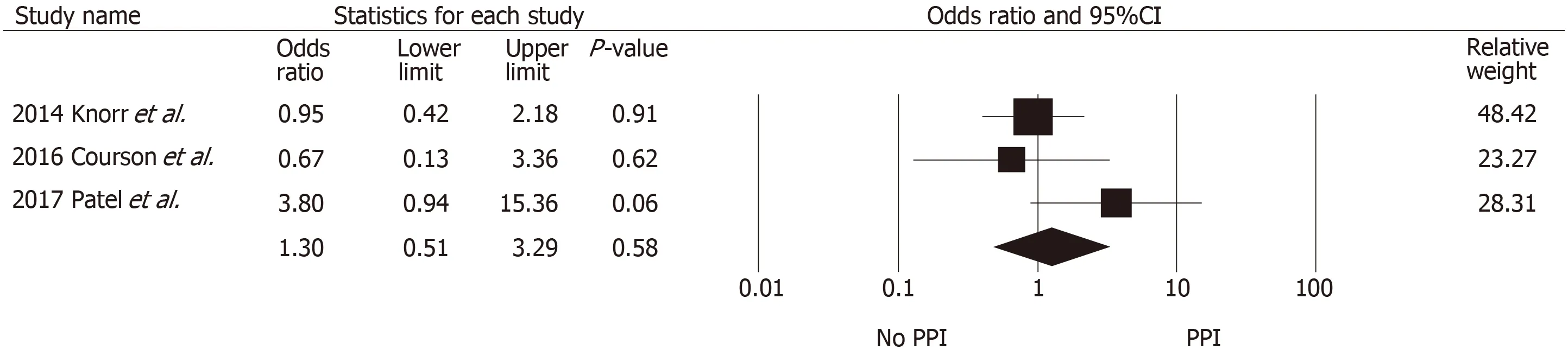
Figure 5 Forest plot of all included studies evaluating the risk of one-year mortality in PPl users compared with non-users.
ARTICLE HIGHLIGHTS
Research background
Adverse renal effects of PPls are increasingly recognized in clinical practice.Pharmacokinetic studies have also raised concerns regarding the interaction between PPIs and immuno suppressive drugs in transplant patients.Whether the adverse effects of PPIs have a clinical significance in kidney transplant recipients remains unclear.
Research motivation
Proton pump inhibitors are commonly used after transplantation for prophylaxis against peptic ulcer disease and for treatment of gastro-esophageal reflux disease or dyspepsia.Prolonged exposure to this class of medication has been shown to be associated with kidney dysfunction,as well as other non-renal adverse outcomes,including hypomagnesemia,fracture,or dementia in the general population.The clinical significance of this drug interaction in kidney transplant recipients is unknown.Several studies have shown a possible increased risk of acute rejection with PPI exposure whereas others have not.
Research objectives
We performed this systematic review and meta-analysis to investigate the adverse outcomes in kidney transplant recipients on PPI compared with those without PPI exposure.
Research methods
A systematic review was conducted in MEDLINE,EMBASE,and Cochrane databases from inception to October 2018 to identify studies that evaluated adverse effects of PPIs in kidney transplant recipients.The outcomes of interest include biopsy-proven acute rejection,graft loss,kidney dysfunction,hypomagnesemia,and overall mortality.The protocol for this meta-analysis is registered with PROSPERO,No.CRD42018115676.
Research results
The authors found no significant association between exposure to PPIs and higher risk of acute biopsy-proven rejection,graft loss,or overall mortality,but a significantly 1.56-fold higher risk of hypomagnesemia among those with PPI exposure was noted.No short-term difference in renal function was found between the two groups.
Research conclusions
PPI use was not associated with significant risks of higher acute rejection,graft loss,or 1-year mortality.However,the risk of hypomagnesemia was significantly increased with PPI use.In the long-term,PPI use may also be associated with kidney dysfunction and increased overall mortality.
Research perspectives
This study demonstrated significant hypomagnesemia in kidney transplant recipients who received PPIs.Since hypomagnesemia is associated with new onset diabetes new-onset diabetes after transplantation,future large-scale clinical studies are needed to assess the impact of PPIs on long-term outcomes.
