耐碳青霉烯类铜绿假单胞菌分布方式以及耐药性研究
2019-05-15周妃妃许磊
周妃妃 许磊

[摘要] 目的 研究耐碳青霉烯类铜绿假单胞菌分布方式以及耐药性。 方法 随机选取2016年6月~2018年6月我院收治的住院患者的铜绿假单胞菌2288株,其中耐碳青霉烯類铜绿假单胞菌60株,占总数的2.6%。进行菌株培养和鉴定、药敏试验,然后分析耐碳青霉烯类铜绿假单胞菌的科室分布及耐药性。 结果 耐碳青霉烯类铜绿假单胞菌主要分布在重症监护室,占总数的50.0%;其次为神经外科,占总数的26.7%;再次为神经内科,占总数的13.4%;最后为呼吸科、骨科、普外科,均占总数的3.3%。耐碳青霉烯类铜绿假单胞菌对美罗培南、亚胺培南、氨曲南、哌拉西林、左氧氟沙星、庆大霉素的耐药性最高,均为100.0%;其次为妥布霉素、哌拉西林/他唑巴坦,耐药性均为96.7%;再次为头孢吡肟、头孢他啶、头孢哌酮/舒巴坦、环丙沙星,耐药性分别为93.3%、90.0%、90.0%、83.3%,最后为阿米卡星,耐药性为16.7%;对多黏菌素B不耐药,耐药性为0。 结论 耐碳青霉烯类铜绿假单胞菌分布较为集中,高度耐药于常见抗菌药物,实时监控耐碳青霉烯类铜绿假单胞菌感染患者能够对其在医院内传播进行有效预防。
[关键词] 耐碳青霉烯类铜绿假单胞菌;药敏试验;分布方式;耐药性
[中图分类号] R378.9 [文献标识码] B [文章编号] 1673-9701(2019)08-0092-03
[Abstract] Objective To study the distribution pattern and drug resistance of carbapenem-resistant Pseudomonas aeruginosa. Methods 2288 strains of Pseudomonas aeruginosa were randomly selected from hospitalized patients admitted to our hospital from June 2016 to June 2018. Among them, there were 60 strains of carbapenem-resistant Pseudomonas aeruginosa, accounting for 2.6% of the total. The strain culture, identification, and drug sensitivity test were carried out, and the department distribution and drug resistance of carbapenem-resistant Pseudomonas aeruginosa were analyzed. Results The carbapenem-resistant Pseudomonas aeruginosa was mainly distributed in the intensive care unit, accounting for 50.0% of the total, followed by the department of neurosurgery, accounting for 26.7% of the total, again followed by the department of neurology, accounting for 13.4% of the total; it was least distributed in the departments of respiratory medicine, orthopedics, and general surgery, accounting for 3.3% of the total. The carbapenem-resistant Pseudomonas aeruginosa showed the highest resistance to meropenem, imipenem, aztreonam, piperacillin, levofloxacin and gentamicin,with the drug resistance of 100.0%, followed by tobramycin, piperacillin/tazobactam, with the drug resistance of 96.7%, again followed by cefepime, ceftazidime,cefoperazone/sulbactam, ciprofloxacin, with the drug resistance of 93.3%, 90.0%, 90.0%, 83.3%, respectively; it showed the least resistance to amikacin, with the drug resistance of 16.7%; it was not resistant to polymyxin B, with the drug resistance of 0. Conclusion The distribution of carbapenem-resistant Pseudomonas aeruginosa is concentrated, which is highly drug resistant to common antibacterial drugs. Real-time monitoring of patients with carbapenem-resistant Pseudomonas aeruginosa infections can effectively prevent their transmission in hospitals.
[Key words] Carbapenem-resistant pseudomonas aeruginosa; Drug sensitivity test; Distribution pattern; Drug resistance
在临床分离的病原菌中,铜绿假单胞菌占有极为重要的地位,而在铜绿假单胞菌感染的治疗中,碳青霉烯类抗菌药物是临床通常采用的治疗药物[1]。但是,近年来,耐碳青霉烯类铜绿假单胞菌在日益广泛应用的该类抗菌药物的作用下日益增多[2]。本研究对2016年6月~2018年6月我院收治的住院患者的铜绿假单胞菌2288株中耐碳青霉烯类铜绿假单胞菌60株的临床资料进行了统计分析,分析了耐碳青霉烯类铜绿假单胞菌分布方式以及耐药性,现报道如下。
1 材料与方法
1.1 一般材料
随机选取2016年6月~2018年6月我院收治的住院患者的铜绿假单胞菌2288株,其中耐碳青霉烯类铜绿假单胞菌60株,占总数的2.6%。纳入标准:所有标本均完整;排除标准:将同一患者相同部位的重复菌株排除在外。在标本类型方面,痰液标本40例,尿液标本8例,血液标本6例,其他6例。
1.2 方法
1.2.1 菌株培养和鉴定 依据常规方法进行细菌培养,采用细胞鉴定仪(VITEK-32型,法国生物梅里埃公司)及其配套NFC卡鉴定细菌。
1.2.2 药敏试验 采用英国Oxoid公司生产的抗菌药物纸片,运用纸片扩散法(K-B)进行药敏试验,将铜绿假单胞菌设定为质控菌株,其ATCC为27853。
1.3 观察指标
分析耐碳青霉烯类铜绿假单胞菌的科室分布。同时分析耐碳青霉烯类铜绿假单胞菌的耐药性。
1.4 统计学方法
采用WHONET5.4软件(世界卫生组织细菌耐药监测网)对所得数据进行统计分析。
2 结果
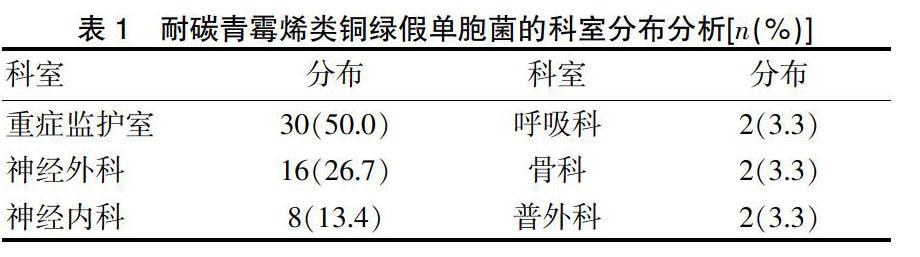
2.1 耐碳青霉烯类铜绿假单胞菌的科室分布分析
耐碳青霉烯类铜绿假单胞菌主要分布在重症监护室,占总数的50.0%;其次为神经外科,占总数的26.7%;再次为神经内科,占总数的13.4%;最后为呼吸科、骨科、普外科,均占總数的3.3%。见表1。
2.2 耐碳青霉烯类铜绿假单胞菌的耐药性分析
耐碳青霉烯类铜绿假单胞菌对美罗培南、亚胺培南、氨曲南、哌拉西林、左氧氟沙星、庆大霉素的耐药性最高,均为100.0%;其次为妥布霉素、哌拉西林/他唑巴坦,耐药性均为96.7%;再次为头孢吡肟、头孢他啶、头孢哌酮/舒巴坦、环丙沙星,耐药性分别为93.3%、90.0%、90.0%、83.3%,最后为阿米卡星,耐药性为16.7%;对多粘菌素B不耐药,耐药性为0。见表2。
3 讨论
铜绿假单胞菌广泛存在于自然界中,属于条件致病菌。相关医学研究表明[3],易感人群为年老体弱具有较为低下的免疫力的患者,占总数的84.7%。从患者脓与创面分泌物标本中来源的铜绿假单胞菌占总数的6.8%,对患者创面进行有效保护,对创伤手术无菌操作进行强化,对洁净的伤口进行有效保持均能够对铜绿假单胞菌感染进行积极有效的预防。碳青霉烯类抗菌药物对铜绿假单胞菌等常见革兰阴性菌的抗菌作用极好,但是近年来,其耐药性在临床大量应用该类药物的作用下日益增强[4]。
相关医学研究表明[5-8],66.2%的铜绿假单胞菌耐药于碳青霉烯类抗菌药物,主要为同时耐药于美罗培南与亚胺培南的菌株。如果铜绿假单胞菌敏感于碳青霉烯类,那么其对其他抗菌药物也具有较低的耐药率,尤其是氨曲南、环丙沙星、哌拉西林/他唑巴坦等。在临床经验治疗中,碳青霉烯类药物及这些药物均可以作为首选抗菌药物。本研究结果表明,耐碳青霉烯类铜绿假单胞菌主要分布在重症监护室,占总数的50.0%;其次为神经外科,占总数的26.7%;再次为神经内科,占总数的13.4%;最后为呼吸科、骨科、普外科,均占总数的3.3%。耐碳青霉烯类铜绿假单胞菌对美罗培南、亚胺培南、氨曲南、哌拉西林、左氧氟沙星、庆大霉素的耐药性最高,均为100.0%;其次为妥布霉素、哌拉西林/他唑巴坦,耐药性均为96.7%;再次为头孢吡肟、头孢他啶、头孢哌酮/舒巴坦、环丙沙星,耐药性分别为93.3%、90.0%、90.0%、83.3%,最后为阿米卡星,耐药性为16.7%;对多黏菌素B不耐药,耐药性为0,和上述相关医学研究结果一致,说明如果铜绿假单胞菌耐药于碳青霉烯类抗菌药物,那么其就具有极为严重的耐药性,极有可能无法治疗。
铜绿假单胞菌耐药于碳青霉烯类抗菌药物的机制主要为膜上缺失ProD2蛋白,增强非特异的外排泵表达,降低外膜通透性,将更多的碳青霉烯酶及AmPC酶产生出来[9-12]。相关医学研究表明[13-16],碳青霉烯酶达到了31.7%的检出率,以此认为铜绿假单胞菌耐药于碳青霉烯类抗菌药物的主要原因并不是产碳青霉烯酶。但是,碳青霉烯酶属于B型金属酶,由于有编码获得性MBL基因存在于耐药菌中,同时MBL能够对几乎所有β内酰胺类抗菌药物进行水解,单环类抗菌药物除外,因此使细菌耐药于碳青霉烯类、青霉素类、头孢菌素类。该基因扩散的途径为通过转座子、Ⅰ类整合子或质粒等,促进铜绿假单胞菌耐药性的增强,同时极易造成医院感染暴发流行[17-20]。因此,要想对医院感染的暴发流行进行有效控制,关键是要对合理应用抗菌药物的力度进行强化,将耐药菌株的产生减少到最低限度。
总之,耐碳青霉烯类铜绿假单胞菌分布较为集中,高度耐药于常见抗菌药物,实时监控耐碳青霉烯类铜绿假单胞菌感染患者能够对其在医院内传播进行有效预防。
[参考文献]
[1] 袁莉莉,丁百兴,沈震,等.耐碳青霉烯类铜绿假单胞菌的耐药性及分子流行病学研究[J].中国感染与化疗杂志,2017,17(3):289-292.
[2] 袁翊,葉帮芬,万小涛,等.耐碳青霉烯类铜绿假单胞菌的耐药机制[J].检验医学与临床,2017,14(11):1602-1604.
[3] 卢雯君,李健,李情操,等.ICU耐碳青霉烯类铜绿假单胞菌检出及同源性分析[J].浙江临床医学,2017,19(5):957-958.
[4] 邸秀珍,王睿.耐碳青霉烯类铜绿假单胞菌耐药机制的研究现状[J].中国临床药理学杂志,2015,31(8):669-672.
[5] 袁利,徐羽中,程明刚,等.耐碳青霉烯类铜绿假单胞菌耐药现状及整合子耐药基因分析[J].中国医学装备,2018,15(4):80-83.
[6] 李情操,姚芳芳,吴巧萍,等.宁波市某医院耐碳青霉烯类铜绿假单胞菌中第一类整合子的分布及来源[J].上海预防医学,2017,29(7):545-547.
[7] 石庆新,吕小萍,於青峰,等.盐酸小檗碱和亚胺培南联合作用耐碳青酶烯类铜绿假单胞菌的体外药敏实验研究[J].中国现代医生,2017,55(1):114-117.
[8] 孙景熙,王福斌,陈剑明,等.手外伤感染患者伤口病原菌分布及耐药性分析[J].中国现代医生,2018,56(4):111-115.
[9] Shortridge D,Pfaller MA,Castanheira M,et al.Antimicrobial activity of ceftolozane-tazobactam tested against Enterobacteriaceae and Pseudomonas aeruginosa collected from patients with bloodstream infections isolated in United States hospitals (2013-2015) as part of the Program to Assess Ceftolozane-Tazobactam Susceptibility (PACTS) surveillance program[J].Diagn Microbiol Infect Dis,2018, 18(18):30168-30168.
[10] Lim CLL,Chua AQ,Teo JQM,et al.Importance of control groups when delineating antibiotic use as risk factors for carbapenem-resistance,extreme-drug and pan-drug resistance in acinetobacter baumannii and pseudomonas aeruginosa:A systematic review and meta-analysis[J].Int J Infect Dis. 2018,2(18)34427-34428.
[11] Karampatakis T,Tsergouli K,Iosifidis E,et al.Impact of active surveillance and infection control measures on carbapenem-resistant Gram-negative bacterial colonization and infections in intensive care[J].J Hosp Infect, 2018,99(4):396-404.
[12] Yeo CK,Vikhe YS,Li P,et al.Hydrogel effects rapid biofilm debridement with ex situ contact-kill to eliminate multidrug resistant bacteria in vivo[J].ACS Appl Mater Interfaces,2018,10(24):20356-20367.
[13] Kuti JL,Wang Q,Chen H,et al.Defining the potency of amikacin against escherichia coli,klebsiella pneumoniae,pseudomonas aeruginosa,and acinetobacter baumannii derived from Chinese hospitals using CLSI and inhalation-based breakpoints[J].Infect Drug Resist,2018, 11(10):783-790.
[14] Dogonchi AA,Ghaemi EA,Ardebili A,et al.Metallo-β-lactamase-mediated resistance among clinical carbapenem-resistant Pseudomonas aeruginosa isolates in northern Iran:A potential threat to clinical therapeutics[J].Ci Ji Yi Xue Za Zhi,2018,30(2):90-96.
[15] Fritzenwanker M,Imirzalioglu C,Herold S,et al.Treatment options for carbapenem-resistant gram-negative infections[J].Dtsch Arztebl Int,2018,115(20-21):345-352.
[16] Gofman N,To K,Whitman M,et al.Successful treatment of ventriculitis caused by Pseudomonas aeruginosa and carbapenem-resistant Klebsiella pneumoniae with i.v. ceftazidime-avibactam and intrathecal amikacin[J]. Am J Health Syst Pharm, 2018,75(13):953-957.
[17] Cho HH,Kwon KC,Kim S,et al.Association between biofilm formation and antimicrobial resistance in carbapenem-resistant pseudomonas aeruginosa[J]. Ann Clin Lab Sci,2018,48(3):363-368.
[18] Jabalameli F,Taki E,Emaneini M,et al.Prevalence of metallo-β-lactamase-encoding genes among carbapenem-resistant Pseudomonas aeruginosa strains isolated from burn patients in Iran[J].Rev Soc Bras Med Trop,2018, 51(3):270-276.
[19] Ismail SJ,Mahmoud SS,First detection of New Delhi metallo-β-lactamases variants(NDM-1,NDM-2) among Pseudomonas aeruginosa isolated from Iraqi hospitals[J]. Iran J Microbiol,2018,10(2):98-103.
[20] Tang X,Xiao M,Zhuo C,et al.Multi-level analysis of bacteria isolated from inpatients in respiratory departments in China[J].J Thorac Dis,2018,10(5):2666-2675.
