产超广谱β—内酰胺酶肺炎克雷伯菌的检测及耐药性分析
2017-07-01李丽刘丹王佳贺
李丽+刘丹+王佳贺
[摘要] 目的 调查中国医科大学附属盛京医院(以下简称“我院”)住院患者产超广谱β-内酰胺酶(ESBLs)肺炎克雷伯菌的临床分布及耐药性,为临床医师抗感染治疗提供依据。 方法 收集2015年1~12月我院住院患者送检的各类标本,采用VITEK 2 Compact进行细菌鉴定和药敏试验,按照CLSI推荐的方法进行ESBLs初步筛选和表型确证试验,并对阳性患者耐药性进行分析。 结果 共检出产ESBLs肺炎克雷伯菌302株,其中痰液标本中检出最多,占38.74%,其次是全血和尿液,分别占28.81%和13.91%;科室分布以儿科和普通外科为主,分别占53.97%和7.95%。产ESBLs肺炎克雷伯菌对氨苄西林、头孢唑啉、哌拉西林、头孢曲松、头孢噻肟的耐药率均在95%以上,而对碳青霉烯类药物的耐药率较低,低于3%。 结论 住院患者产ESBLs肺炎克雷伯菌的耐药率高,治疗难度大,医师应根据药敏试验结果加强对抗生素的合理使用。
[关键词] 肺炎克雷伯菌;超广谱β-内酰胺酶;耐药性;病原菌
[中图分类号] R969.3 [文献标识码] A [文章编号] 1673-7210(2017)05(b)-0103-04
[Abstract] Objective To analyze the clinical distribution and drug resistance of extended-spectrum beta-lactamase (ESBLs)-producing Klebsiella pneumoniae in hospitalized patients in Shengjing Hospital Affiliated to China Medical University ("our hospital" for short), in order to provide references for therapy of infections. Methods ESBLs-producing Klebsiella pneumoniae isolated in our hospital from January to December 2015 were collected. The bacteria identification and drug sensitivity test were performed by the VITEK 2 Compact. The ESBLs preliminary screening and the phenotypic confirmatory test were taken according to the guideline of CLSI, and at the same time, the results of the drug sensitivity test were analyzed. Results 302 strains of ESBLs-producing Klebsiella pneumoniae were isolated, which were mostly isolated from sputum samples (38.74%), followed by blood (28.81%) and urine (13.91%). The bacteria were mainly distributed in Paediatrics Department (53.97%) and General Surgery Department (7.95%). The drug resistances of ESBLs-producing Klebsiella pneumoniae to Ampicillin, Cefazolin, Piperacillin, Ceftriaxone, Cefotaxime in hospitalized patients were more than 95%, and the resistance rate to carbapenemes was lower, less than 3%. Conclusion The isolated ESBLs-producing Klebsiella pneumoniae in hospitalized patients are highly resistant to the commonly used antibiotics, and the treatment is difficult. Therefore, the drug sensitive test should be strengthened to direct clinical rational use of antibiotics.
[Key words] Klebsiella pneumoniae; Extended spectrum beta-lactamases; Drug resistance; Pathogens
肺炎克雷伯菌廣泛分布于自然界,是引起呼吸道感染重要的条件致病菌,其临床分离率在革兰阴性杆菌中居第3位[1-2]。产生超广谱β-内酰胺酶(extended-spectrum beta-lactamase,ESBLs)是肺炎克雷伯菌的主要耐药机制之一[3],由其引起的感染在儿童及老年患者、免疫力低下的患者以及接受各种侵入性诊疗操作的重症患者中发病率高[4]。随着抗菌药物的广泛使用,尤其是第三代头孢菌素类药物在临床上的大量使用,使得产ESBLs肺炎克雷伯菌的耐药性不断上升[5]。因此,本研究收集2015年1~12月中国医科大学附属盛京医院(以下简称“我院”)住院患者送检的标本的培养结果,对其产ESBLs肺炎克雷伯菌的感染情况及其耐药特点进行回顾性分析,为临床合理选择抗产ESBLs肺炎克雷伯菌的药物提供参考依据,现报道如下:
1 资料与方法
1.1 一般资料
收集我院住院患者的痰液、全血、尿液及分泌物等各类临床感染标本,同一患者相同类型标本中多次分离的同一菌株阳性标本按一例计算。质控菌株为肺炎克雷伯菌ATCC700603,购自原卫生部临床检验中心。
1.2 方法
1.2.1 细菌学鉴定及药敏实验 送检样本均按照《全国临床检验操作规程》[6]的操作要求对各种临床标本进行培养分离,采用法国生物梅里埃公司的全自动细菌鉴定和Vitek2 Compact药敏分析系统进行分析鉴定和药敏试验。操作方法和结果评价严格按照美国临床实验室标准化委员会(CLSI)标准和指南[7]进行。
1.2.2 ESBLs检测 根据CLSI推荐的ESBLs初步筛选和表型确证试验检测[8]。
2 结果
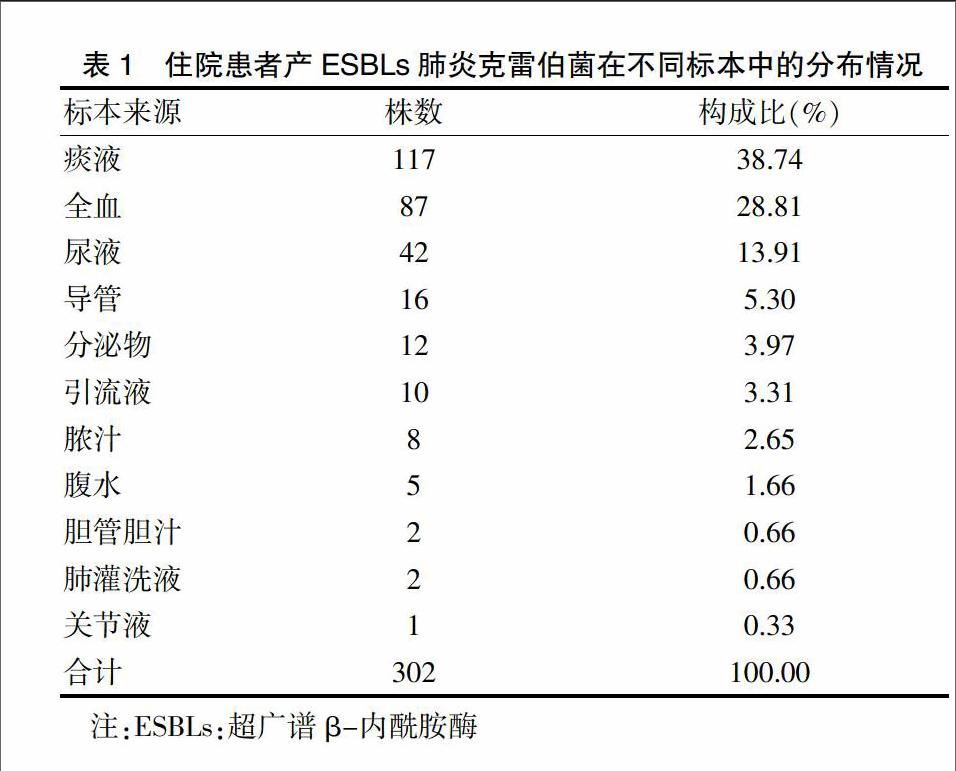
2.1 我院住院患者产ESBLs肺炎克雷伯菌的标本来源分布
经培养共检出产ESBLs肺炎克雷伯菌302株,主要来源于痰液、全血、尿液,分别占38.74%、28.81%、13.91%。见表1。
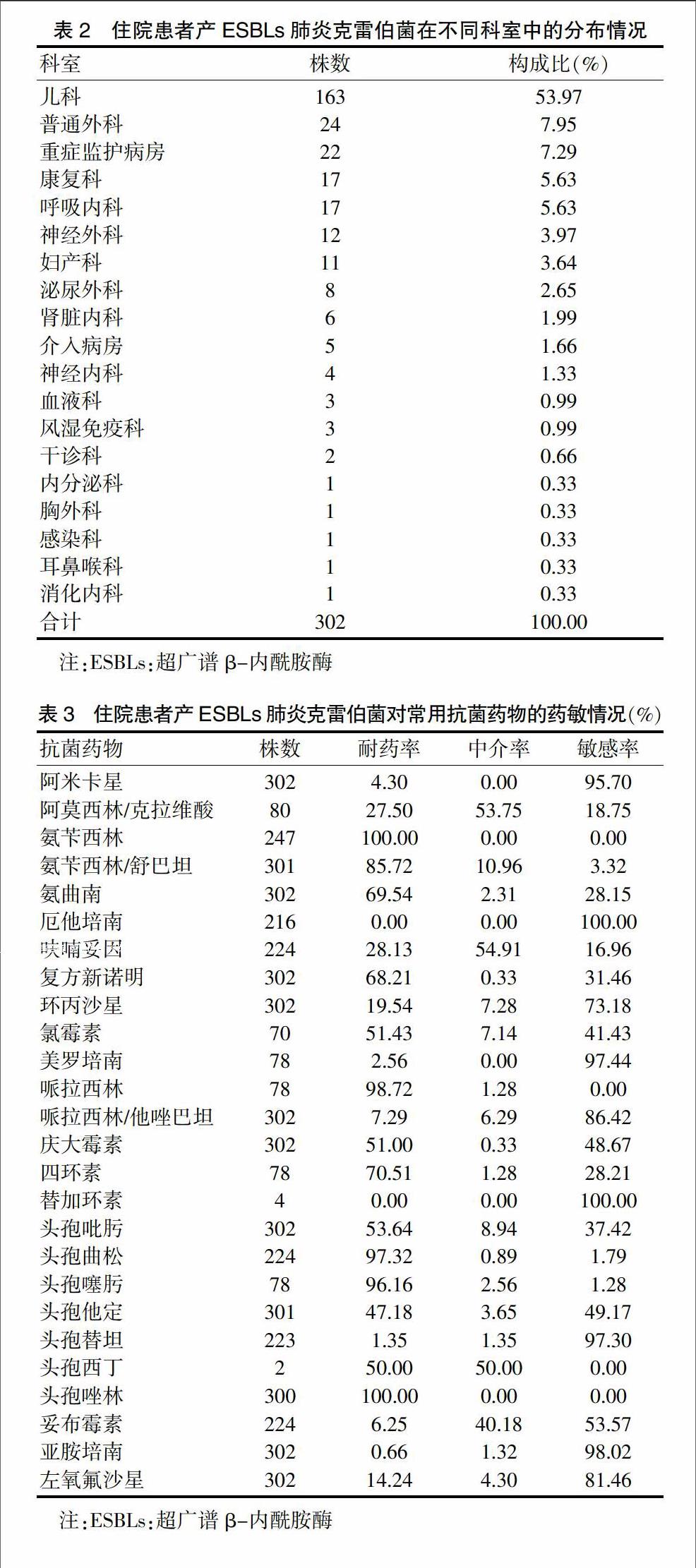
2.2 我院住院患者产ESBLs肺炎克雷伯菌的科室分布
我院住院患者产ESBLs肺炎克雷伯菌主要分布在儿科、普通外科及重症监护病房,分别占53.97%、7.95%、7.29%。見表2。
2.3 我院住院患者产ESBLs肺炎克雷伯菌对常用抗菌药物的耐药性
我院住院患者产ESBLs肺炎克雷伯菌对氨苄西林、头孢唑啉、哌拉西林、头孢曲松、头孢噻肟的耐药率较高,分别为100.00%、100.00%、98.72%、97.32%、96.16%,对厄他培南、亚胺培南、美罗培南、头孢替坦、阿米卡星的敏感率较高,分别为100.00%、98.02%、97.44%、97.30%、95.70%。见表3。
3 讨论
ESBLs由质粒介导,能水解青霉素类、单酰胺类及头孢菌素类等抗菌药物[9],其特点是能使细菌对多种类型的β-内酰胺类抗菌药物产生耐药性[10],具有作用底物广、易播散、数量种类多、个体差异大的特点[11-12]。近年来,随着临床上广泛使用β-内酰胺类抗生素治疗各类感染,使得革兰阴性菌中的许多菌株对抗生素类药物的耐药性越发突出,以产ESBLs菌耐药性最为显著,尤其是产ESBLs肺炎克雷伯菌具有较高的多重耐药性和交叉耐药性,容易引起暴发和流行[13-15],给临床治疗带来极大困扰。
分析本研究我院住院患者中检出的产ESBLs肺炎克雷伯菌标本分布可见,302株肺炎克雷伯菌分离自临床的各类标本,其中以痰液中最多,占38.74%,表明产ESBLs肺炎克雷伯菌主要引起呼吸系统感染;其次为全血和尿液,分别占28.81%和13.91%,说明产ESBLs肺炎克雷伯菌亦容易引起血流感染和尿路感染。科室分布方面,我院住院患者产ESBLs肺炎克雷伯菌主要分布在儿科,占53.97%,说明产ESBLs肺炎克雷伯菌容易引起儿童院内感染,与何丽芸等[16]报道一致;其次为普通外科、重症监护病房、康复科和呼吸内科等科室,分别占7.95%、7.29%、5.63%和5.63%,这些科室患者抵抗力较低,住院时间长,经验性应用三代头孢菌素较多,说明产ESBLs肺炎克雷伯菌是引起院内感染的重要病原菌,应引起医护人员的重视。这与孙红等[17]报道的多见于重症监护病房和感染科病房略有差异,可能与各临床科室感染特点不同、地区差异以及标本的送检等因素有关。
从产ESBLs肺炎克雷伯菌对临床常用的抗菌药物耐药率的统计结果中发现:产ESBLs肺炎克雷伯菌对氨苄西林、哌拉西林等β-内酰胺类药物耐药,而对亚胺培南、美罗培南、厄他培南等碳青霉烯类药物敏感。与2013年孙立群等[18]报道的产ESBLs肺炎克雷伯菌对亚胺培南和美罗培南的耐药率均为0相比,我院产ESBLs肺炎克雷伯菌对亚胺培南和美罗培南的耐药率较高,分别为0.66%和2.56%,应引起临床医生的关注。产ESBLs肺炎克雷伯菌对碳青霉烯类抗菌药物敏感与碳青霉烯类药物特殊的分子结构有关,碳青霉烯类的β-内酰胺环较小,容易进入细菌的微孔蛋白通道,同时,碳青霉烯类药物有特异的反式结构,两者相互作用使其对β-内酰胺酶高度稳定[19-21]。此外,分析结果显示我院产ESBLs肺炎克雷伯菌对β-内酰胺酶抑制剂药物阿莫西林/克拉维酸、氨苄西林/舒巴坦、哌拉西林/他唑巴坦的耐药率分别为27.50%、85.72%、7.29%,说明ESBLs可以被舒巴坦、他唑巴坦等β-内酰胺酶抑制剂所抑制[22]。我院产ESBLs肺炎克雷伯菌对庆大霉素的耐药率为51%,对左氧氟沙星的耐药率为14.24%,说明产ESBLs肺炎克雷伯菌对喹诺酮类和氨基糖苷类抗菌药物亦有一定的耐药性,与其质粒携带的耐药基因的多重耐药性有关[23]。因此,在临床上对产ESBLs肺炎克雷伯菌引起感染的治疗应首选敏感的碳青霉烯类抗菌药物,根据药敏结果慎重选用β-内酰胺酶抑制剂、氨基糖苷类和喹诺酮类,而大多数β-内酰胺类和第一、二代头孢菌素类对其无效。
综上所述,住院患者产ESBLs肺炎克雷伯菌菌株检出率比较高,引起的院内感染不断增加,并且抗菌药物耐药类型众多。在临床研究中,应对产ESBLs肺炎克雷伯菌株进行严密监测,根据细菌培养及药敏试验结果耐药情况,选择合理的抗菌药物,可有效预防医院感染。
[参考文献]
[1] Kazmierczak KM,Lob SH,Hoban DJ,et al. Characterization of extended-spectrum beta-lactamases and antimicrobial resistance of Klebsiella pneumoniae in intra-abdominal infection isolates in Latin America,2008-2012. Results of the Study for Monitoring Antimicrobial Resistance Trends [J]. Diagn Microbiol Infect Dis,2015,82(3):209-214.
[2] Peralta G,Lamelo M,Alvarez-García P,et al. Impact of empirical treatment in extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella spp. bacteremia. A multicentric cohort study [J]. BMC Infect Dis,2012,12(1):245.
[3] Gholipour A,Soleimani N,Shokri D,et al. Phenotypic and Molecular Characterization of Extended-Spectrum β-Lactamase Produced by Escherichia coli,and Klebsiella pneumoniae Isolates in an Educational Hospital [J]. Jundishapur J Microbiol,2014,7(10):e11758.
[4] Mansury D,Motamedifar M,Sarvari J,et al. Antibiotic susceptibility pattern and identification of extended spectrum β-lactamases (ESBLs) in clinical isolates of Klebsiella pneumoniae from Shiraz,Iran [J]. Iran J Microbiol,2016,8(1):55-61.
[5] Somily AM,Habib HA,Absar MM,et al. ESBL-producing Escherichia coli and Klebsiella pneumoniae at a tertiary care hospital in Saudi Arabia.[J]. J Infect Dev Ctries,2014,8(9):1129-1136.
[6] 尚紅,王毓三,申子瑜.全国临床检验操作规程[M].北京:人民卫生出版社,2015.
[7] 李小鹏,王治国.美国临床实验室标准化委员会标准与指南[J].中华检验医学杂志,2001,24(4):251-252.
[8] 张长虹,孟存仁,晓英.产ESBLs大肠埃希菌和肺炎克雷伯菌耐药性分析及TEM、SHV基因检测[J].国际检验医学杂志,2015,36(5):583-585.
[9] Shaikh S,Fatima J,Shakil S,et al. Antibiotic resistance and extended spectrum beta-lactamases:Types,epidemiology and treatment [J]. Saudi J Biol Sci,2015,22(1):90-101.
[10] Van Aken S,Lund N,Ahl J,et al. Risk factors,outcome and impact of empirical antimicrobial treatment in extended-spectrum β-lactamase-producing Escherichia coli bacteraemia [J]. Scand J Infect Dis,2014,46(11):753-762.
[11] Giske CG,Sundsfjord AS,Kahlmeter G,et al. Redefining extended-spectrum beta-lactamases:balancing science and clinical need [J]. J Antimicrob Chemother,2009,63(1):1-4.
[12] 朱瑞琪,张蕴莉,张淑芹,等.2011-2013年某综合性医院产ESBLs 细菌的分布及耐药动态监测[J].现代预防医学,2015,42(18): 3450-3453.
[13] Biedenbach DJ,Bouchillon SK,Hoban DJ,et al. Antimicrobial susceptibility and extended-spectrum beta-lactamase rates in aerobic gram-negative bacteria causing intra-abdominal infections in Vietnam:report from the Study for Monitoring Antimicrobial Resistance Trends(SMART 2009-2011)[J]. Diagn Microbiol Infect Dis,2014,79(4):463-467.
[14] Leistner R,Gürntke S,Sakellariou C,et al. Bloodstream infection due to extended-spectrum beta-lactamase(ESBL)-positive K. pneumoniae and E. coli:an analysis of the disease burden in a large cohort [J]. Infection,2014, 42(6):991-997.
[15] Vibet MA,Roux J,Montassier E,et al. Systematic analysis of the relationship between antibiotic use and extended-spectrum beta-lactamase resistance in Enterobacteriaceae in a French hospital:a time series analysis [J]. Eur J Clin Microbiol Infect Dis,2015,34(10):1957-1963.
[16] 何丽芸,王应建,李季美.婴幼儿社区获得性肺炎克雷伯菌肺炎的臨床特点及耐药分析[J].中国当代儿科杂志,2012,14(11):827-829.
[17] 孙红,乔艳,郭普,等.肺炎克雷伯菌产ESBLs的检测及耐药性分析[J].中华全科医学,2011,9(5):797-798.
[18] 孙立群,梁金花,李荣辉.大肠埃希菌与肺炎克雷伯菌耐药性及产ESBLs菌株的分析[J].中华医院感染学杂志,2013,23(2):455-457.
[19] 李忠,曾金红,李亚,等.基层医院肺炎克雷伯菌的临床感染分布和耐药谱分析[J].中国医药科学,2015,5(3):66-69.
[20] Udomsantisuk N,Nunthapisud P,Tirawatanapong T,et al. Molecular characterization of extended spectrum beta-lactamase among clinical isolates Escherichia coli and Klebsiella pneumoniae [J]. J Med Assoc Thai,2011,94(12):1504-1512.
[21] 唐景云,秦晓林.ESBLs在大肠埃希菌、肺炎克雷伯菌和阴沟肠杆菌中的检出率及耐药情况比较[J].中国医药科学,2016,6(3):175-178.
[22] Kaftandzieva A,Trajkovska-Dokic E,Panovski N. Prevalence and molecular characterization of Extended Spectrum Beta-Lactamases(ESBLs)producing Escherichia Coli and Klebsiella Pneumoniae.[J]. Prilozi,2011,32(2):129-141.
[23] Yadav KK,Adhikari N,Khadka R,et al. Multidrug resistant Enterobacteriaceae and extended spectrum β-lactamase producing Escherichia coli:a cross-sectional study in National Kidney Center,Nepal [J]. Antimicrob Resist Infect Control,2015,4(1):42.
(收稿日期:2017-01-10 本文编辑:程 铭)
