分叉下颌神经管的研究概述
2017-02-02李庭庭刘亚林李长义
李庭庭 刘亚林 李长义
分叉下颌神经管(Bifid mandibular canal)认为是由于胚胎时期下颌骨性管道未充分融合形成的一种变异结构[4,11,12],是下颌神经管常见变异的一种,在临床工作中常被忽略。因此了解其发生率、位置、走向、分布等对下颌第三阻生齿拔除、自体骨移植、种植体植入术、外伤固定、下颌升支矢状劈开术、根管治疗术等操作有重要的临床意义。下面对分叉下颌神经管的国内外研究作一综述。
1.分叉下颌神经管概述
1.1 分叉下颌神经管的形成原因 下颌神经管是位于下颌骨骨松质内的骨性管道,而分叉下颌神经管(Bifid mandibular canal)可看作是下颌神经管的分支结构。目前学者们普遍认为分叉下颌管是下颌管的一种结构变异,是下颌管的不全融合所致。1996年,chávez-Lomeli等[11]对302例产前期胎儿的下颌骨标本进行研究,发现下颌神经管是由三个独立的神经小管融合而成,在发育过程中,如发生独立神经小管的不全融合,则会形成分叉下颌管。
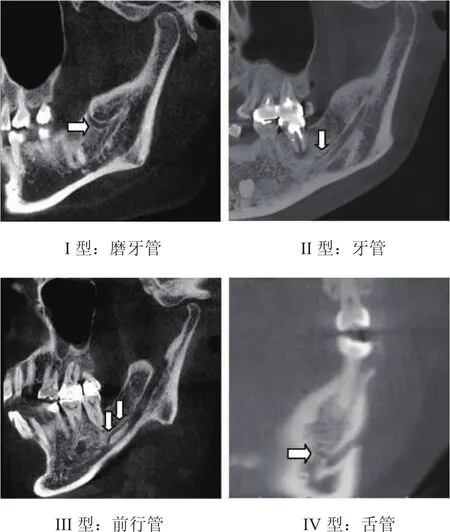
1.2 分叉下颌神经管的分型 Naitoh等[1]通过锥形束CT对分叉下颌神经管进行分析,根据其分叉部位及位置进行分类,将其分为4种类型。2005年,Auluck等[13]通过曲面断层片首次发现三分支下颌管,之后越来越多的学者研究发现其存在[9,14-16],因此,目前可将分叉下颌管分成五型:I型:又称磨牙管(Retromolar canal),下颌管发出分支后开口于磨牙后区骨表面。II型:又称牙管(Dental canal),下颌管发出分支后分支末端位于第一、第二或第三磨牙根尖,根据接触牙位不同分为三个亚型:A亚型:与下颌第一磨牙接触;B亚型:与下颌第二磨牙接触;C亚型:与下颌第三磨牙接触。III型:又称前行管(Forward canal),在下颌神经管上壁发出分叉后,分支与主干在下颌骨体部前行。根据分支与主干是否汇合而分两个亚型:A亚型:分叉后分支与主干无汇合;B亚型:分叉后分支与主干有汇合。IV型:又称颊舌管(Buccolingual canal),分两型,A亚型:分支在分叉下颌管主干的颊侧走行;B亚型:分支在分叉下颌管主干的舌侧走行。V型:三分支下颌管(trifid mandibular)或其他类型。分支类型如下图(图片源于天津医科大学口腔医院影像科)
2.分叉下颌神经管的发生率

V型:其他
一般认为,解剖标本可准确检测分叉下颌神经管的存在。Bogdan等[12]对46例下颌骨解剖标本进行研究,其中发现双叉下颌管8例,三分支下颌管1例,分叉下颌管的发生率约为19.6%,与此同时,研究人员对1000例曲面体层片进行分析发现2例双叉下颌管,可见曲面断层片对于分叉下颌管的显影率较低。Bilecenoglu等[17]对40例下颌骨标本进行研究,发现10例存在分叉下颌管之磨牙管,发生率约为25%,而Scheijtman等[18]在18例头颅标本中发现13例存在磨牙管,发生率为72%。综上显示分叉下颌神经管的发生率差异较大。
随着影像学技术的发展,CBCT在口腔颌面部疾病诊断中被广泛应用[19]。Muinelo-Lorenzo等[7]对225名智利人进行研究,分别对其进行CBCT及曲面断层片扫描,CBCT中分叉下颌管发生率为36.8%,男性发生率高于女性,前行管发生率最高为16.8%,磨牙管次之为12%,而曲面断层片中分叉下颌管发生率为16.8%,研究显示CBCT中111例分叉下颌管仅42例在曲面断层片中显影,可见CBCT中分叉下颌管的显影率高于曲面断层片。Maria等[20]运用CBCT对30名巴西人下颌骨进行研究,分叉下颌管发生率为26.67%。Naitoh等[1]运用CBCT对122名日本人下颌骨进行研究,分叉下颌管发生率为65%,其中前行管发生率为44.3%,磨牙管发生率为25.4%。Rashsuren等[9]发现500名韩国人中有113例存在分叉下颌管,发生率为22.6%,其中磨牙管发生率为71.3%,牙管发生率为18.8%,前行管发生率为4.1%,三叉下颌管发生率为5.8%。叶立等[21]研究发现500名四川地区成年人中69例存在分叉下颌管,发生率为13.8%。研究分析表明分叉下颌神经管发生率不尽相同,男女也有一定差异,这可能与基因、环境等因素相关[22]。
3.分叉下颌神经管的检测手段
1973年以来,学者们通过多种方法观察分析分叉下颌管,其中影像学方法主要有曲面断层和锥形束CT。
关于分叉下颌管的研究,早期只是局限于个别的病例报道[6,23]。而在曲面断层片中Kalantar、Sanchis、Bogdan等[24,25,12]研究发现其发生率分别为1.2%、0.35%、0.2%,发生率偏低,这是因为曲面断层片是二维图像,分辨率较低,分叉下颌管有可能受到气道、软腭等生理解剖结构的影响,因此曲面断层诊断分叉下颌管准确性较差。此外,分叉下颌管分支的类型,颊舌管的方向[2]以及下颌管分支直径的大小等[26,27],都可能影响其正确的诊断。
随着CBCT在口腔领域的广泛应用,因其具有图像精确,高分辨率等特点,同时能够提供冠状位、矢状位、水平位的三维重建,可以更为清晰的显示下颌管等颌骨细微结构图像[28]。研究发现,磨牙孔即是磨牙管于颌骨表面的开口[10,12,17],一般位于磨牙后垫下方,其解剖形态可以在CBCT的截面图中清晰的显示,且形态完全一致[10]。回顾文献发现,解剖标本中分叉下颌管之磨牙管的发生率约5.1%-72%[17,18,22,29],而CBCT中磨牙管发生率约为12.4%-75.43%[7,27,30],具体如下图,通过对比可见CBCT与尸体解剖对于分叉下颌管的诊断率基本一致[10],可见CBCT是诊断分叉下颌神经管的一种准确可行的方法。
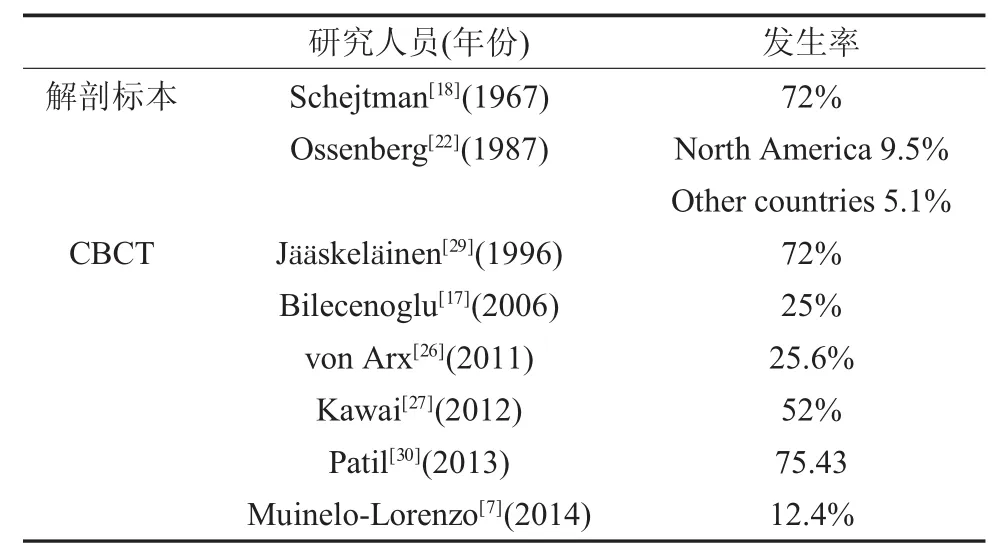
解剖标本与CBCT中磨牙管的发生率比较
4.诊断分叉下颌神经管的临床意义
Aljunid等[31]研究发现,分叉下颌神经管内存在神经血管,Fukami等[10]对下颌骨标本的磨牙管进行组织学研究,同样发现其内含有神经血管束,且其直径与下颌管内神经血管近似,因此,分叉下颌管的损伤与主神经管本身损伤一样,也会出现出血、感觉神经的干扰或形成创伤性神经瘤等并发症[24,26,32,33]。
下牙槽神经损伤90%是由于拔除下颌阻生齿引起的,而拔牙过程中的牙齿移位、舌侧骨板骨折也会损伤到与下颌第三磨牙位置关系密切的分叉下颌管,从而引起出血及术后感觉异常等并发症。而分叉下颌管主要位于磨牙区及下颌骨升支,此位置是磨牙区种植术、取骨术及下颌骨升支矢状劈开术的手术位置,国内外均有病例报道发现磨牙区种植位点存在分叉下颌管[31,34],可见术前通过CBCT进行影像学分析,对其进行三维定位,确定下颌神经管及其分支的位置以决定安全手术区域,模拟手术过程[21,35],从而有效规避临床操作风险,避免术中、术后并发症。
此外,根管治疗术引起的下牙槽神经损伤也有报道,Knowles等[36]研究显示其发生率仅为0.96%,其原因主要是与下颌前磨牙、磨牙的根管内容物超出根尖孔,压迫下牙槽神经有关,因为分叉下颌管部分与磨牙根尖有接触,在根管治疗术中内容物超充则可能损伤分叉下颌管引起神经损伤。
5.展望
随着CBCT的发展,提高图像分辨率可以更加直观、准确的对细微结构的三维图像进行诊断,同时将CBCT作为临床医师对磨牙区、磨牙后区及下颌骨升支等区域相关疾病治疗前的必要检查手段之一,对分叉下颌管进行三维定位分析,从而减少临床操作中分叉下颌管的损伤。
[1] Naitoh M,Hiraiwa Y,Aimiya H,et al.Observation of bifid mandibular canal using cone-beam computerized tomography[J].The International journal of oral&maxillofacial implants,2009,24(1):155-159
[2] Kuribayashi A,Watanabe H,Imaizumi A,et al.Bifid mandibular canals:cone beam computed tomography evaluation[J].Dento maxillo facial radiology,2010,39(4):235-239
[3] DeOliveira-SantosC,Souza PHC,DeAzambuja Berti-Couto S,et al.Assessment of variations of the mandibular canal through cone beam computed tomography[J].Clinical Oral Investigations,2012,16(2):387-393
[4] Fu E,Peng M,Chiang C-Y,et al.Bifid mandibular canals and the factors associated with their presence:a medical computed tomography evaluation in a Taiwanese population[J].Clinical Oral Implants Research,2014,25(2):e64-e67
[5] Kang J-H,Lee K-S,Oh M-G,et al.The incidence and configuration of the bifid mandibular canal in Koreans by using cone-beam computed tomography[J].Imaging science in dentistry,2014,44(1):53-60
[6] Kiersch TA,Jordan JE.Duplication of the mandibular canal[J].Oral surgery,oral medicine,and oral pathology,1973,35(1):133-134
[7] Muinelo-Lorenzo J,Suarez-Quintanilla JA,Fernandez-Alonso A,et al.Descriptive study of the bifid mandibular canals and retromolar foramina:cone beam CT vs panoramic radiography[J].Dento maxillo facial radiology,2014,43(5):20140090
[8] Orhan K,Aksoy S,Bilecenoglu B,et al.Evaluation of bifid mandibular canals with cone-beam computed tomography in a Turkish adult population:a retrospective study[J].Surgical and radiologic anatomy:SRA,2011,33(6):501-507
[9] Rashsuren O,Choi JW,Han WJ,et al.Assessment of bifid and trifid mandibular canals using cone-beam computed tomography[J].Imaging science in dentistry,2014,44(3):229-236
[10]Fukami K,Shiozaki K,Mishima A,et al.Bifid mandibular canal:confirmation of limited cone beam CT findings by gross anatomical and histological investigations[J].Dentomaxillofacial Radiology,2012,41(6):460-465
[11]Chavez-Lomeli ME,Mansilla Lory J,Pompa JA,et al.The human mandibular canal arises from three separate canals innervating different tooth groups[J].Journal of dental research,1996,75(8):1540-1544
[12]Bogdan S,Pataky L,Barabas J,et al.Atypical courses of the mandibularcanal:comparative examination of dry mandiblesand x-rays[J].The Journal of craniofacial surgery,2006,17(3):487-491
[13]Auluck A,Pai KM.Trifid mandibular nerve canal[J].Dento maxillo facial radiology,2005,34(4):259
[14]Mizbah K,Gerlach N,Maal TJ,et al.The clinical relevance of bifid and trifid mandibular canals[J].Oral and Maxillofacial Surgery,2012,16(1):147-151
[15]Auluck A,PaiKM,Mupparapu M.Multiplemandibular nerve canals:radiographic observations and clinical relevance.Report of 6 cases[J].Quintessence international(Berlin,Germany:1985),2007,38(9):781-787
[16]Wadhwani P,Mathur RM,Kohli M,et al.Mandibular canal variant:a casereport[J].Journalof oralpathology&medicine:official publication of the International Association of Oral Pathologists and the American Academy of Oral Pathology,2008,37(2):122-124
[17]Bilecenoglu B,Tuncer N.Clinical and Anatomical Study of Retromolar Foramen and Canal[J].Journal of Oral and Maxillofacial Surgery,2006,64(10):1493-1497
[18]Schejtman R,Devoto FC,Arias NH.The origin and distribution of the elements of the human mandibular retromolar canal[J].Archives of oral biology,1967,12(11):1261-1268
[19]李 艳,赵 今.锥形束CT在口腔颌面部疾病诊治中的临床应用[J].中华老年口腔医学杂志,2009,7(4):253-255
[20]Villaça-Carvalho MFL,Manhães LRC,de Moraes MEL,et al.Prevalence of bifid mandibular canals by cone beam computed tomography[J].Oral and Maxillofacial Surgery,2016,20(3):289-294
[21]叶 立,陈娅飞,裴 君,等.四川地区成年人群中分叉下颌管的锥形束CT研究[J].华西口腔医学杂志,2017,35(1):82-88
[22]Ossenberg NS.Retromolar foramen of the human mandible[J].American Journal of Physical Anthropology,1987,73(1):119-128
[23]Patterson JE,Funke FW.Bifid inferior alveolar canal[J].O-ral surgery,oral medicine,and oral pathology,1973,36(2):287-288
[24]Kalantar Motamedi MH,Navi F,Sarabi N.Bifid Mandibular Canals:Prevalence and Implications[J].Journal of Oral and Maxillofacial Surgery,2015,73(3):387-390
[25]Sanchis JM,Penarrocha M,Soler F.Bifid mandibular canal[J].Journal of oral and maxillofacial surgery:official journal of the American Association of Oral and Maxillofacial Surgeons,2003,61(4):422-424
[26]von Arx T,Hänni A,Sendi P,et al.Radiographic Study of the Mandibular Retromolar Canal:An Anatomic Structure with Clinical Importance[J].Journal of Endodontics,2011,37(12):1630-1635
[27]Kawai T,Asaumi R,Sato I,et al.Observation of the retromolar foramen and canal of the mandible:a CBCT and macroscopic study[J].Oral Radiology,2012,28(1):10-14
[28]Loubele M,Guerrero ME,Jacobs R,et al.A comparison of jaw dimensional and quality assessments of bone characteristics with cone-beam CT,spiral tomography,and multi-slice spiral CT[J].The International journal of oral&maxillofacial implants,2007,22(3):446-454
[29]Jääskeläinen SK,Peltola JK,Lehtinen R.The mental nerve blink reflex in the diagnosis of lesions of the inferior alveolar nerve following orthognathic surgery of the mandible[J].British Journal of Oral and Maxillofacial Surgery,1996,34(1):87-95
[30]Patil S,Matsuda Y,Nakajima K,et al.Retromolar canals as observed on cone-beam computed tomography:their incidence,course,and characteristics[J].Oral Surg Oral Med Oral Pathol Oral Radiol,2013,115(5):692-699
[31]Aljunid S,AlSiweedi S,Nambiar P,et al.The Management of Persistent Pain From a Branch of the Trifid Mandibular Canal due to Implant Impingement[J].The Journal of oral implantology,2016,42(4):349-352
[32]Kuczynski A,Kucharski W,Franco A,et al.Prevalence of bifid mandibular canals in panoramic radiographs:a maxillofacial surgical scope[J].Surgical and Radiologic Anatomy,2014,36(9):847-850
[33]Claeys V,Wackens G.Bifid mandibular canal:literature review and case report[J].Dentomaxillofacial Radiology,2005,34(1):55-58
[34]郭苏伟,高承志.下颌神经管变异的种植修复1例[J].口腔颌面修复学杂志,2015,16(5):293-295
[35]张 翀,刘 明,赵宝红,等.CBCT和曲面断层在下颌后牙区种植中的应用价值分析[J].口腔颌面修复学杂志,2012(4):228-231
[36]Knowles KI,Jergenson MA,Howard JH.Paresthesia associated with endodontic treatment of mandibular premolars[J].Journal of endodontics,2003,29(11):768-770
