N末端B型利钠肽原、中心动脉压与冠状动脉病变的相关性研究
2016-12-14黄冠华张顺祥冯美云
黄冠华,王 丛,张顺祥,冯美云
·论著·
N末端B型利钠肽原、中心动脉压与冠状动脉病变的相关性研究
黄冠华,王 丛,张顺祥,冯美云
目的 探讨N末端B型利钠肽原(NT-proBNP)、中心动脉压(CAP)与冠状动脉病变的相关性。方法 选取2012年12月—2014年12月在包头医学院第二附属医院心内科行冠状动脉造影者150例,根据SYNTAX积分分为冠状动脉正常组(0分,n=50)和冠状动脉病变组(≥1分,n=100),其中冠状动脉病变组又分为:低危组(1~22分,n=40)、中危组(23~32分,n=35)和高危组(≥33分,n=25)。收集所有受试者的一般资料(包括性别、年龄、BMI、血压、血糖、血脂等),采用美国罗氏2010电化学发光免疫分析仪测定血浆NT-proBNP水平,采用日本欧姆龙公司的无创桡动脉脉波检测装置(HEM9000AI)测量CAP。结果 4组年龄、BMI、收缩压(SBP)、空腹血糖(FPG)、总胆固醇(TC)、三酰甘油(TG)、低密度脂蛋白胆固醇(LDL-C)间差异有统计学意义(P<0.05);而性别、舒张压(DBP)、高密度脂蛋白胆固醇(HDL-C)间差异无统计学意义(P>0.05)。4组NT-proBNP、中心动脉收缩压(CSP)间差异有统计学意义(P<0.05),而中心动脉舒张压(CDP)间差异无统计学意义(P>0.05)。NT-proBNP、CSP水平与SYNTAX积分均呈直线正相关(r值分别为0.870、0.743,P<0.001)。结论 NT-proBNP、CSP均与冠状动脉病变有关,随着NT-proBNP、CSP水平上升,冠状动脉病变程度加重。
N末端B型利钠肽原;中心动脉压;冠状动脉疾病
黄冠华,王丛,张顺祥,等.N末端B型利钠肽原、中心动脉压与冠状动脉病变的相关性研究[J].中国全科医学,2016,19(34):4208-4212.[www.chinagp.net]
HUANG G H,WANG C,ZHANG S X,et al.Correlation of NT-proBNP and central aortic pressure levels with the severity of coronary artery disease[J].Chinese General Practice,2016,19(34):4208-4212.
随着全球人均生活水平的提高,心脑血管疾病尤其是冠状动脉粥样硬化性心脏病(冠心病)已经在全球尤其在发展中国家蔓延,且成为世界第一位的死亡原因[1]。在冠状动脉粥样硬化的发生发展过程中,血脂异常、高血压、糖尿病、营养与不良的饮食习惯、肥胖或超重、吸烟、过度饮酒、年龄、性别以及久坐的生活方式是密切相关的危险因素,这些因素造成了冠状动脉内皮的损伤,为粥样斑块的形成埋下隐患[2-3]。除了一些传统的危险因素以外,近年来有些学者提出冠心病可能存在其他危险因素,如N末端B型利钠肽原(NT-proBNP)、中心动脉压(CAP)等[4-5]。本研究旨在探讨NT-proBNP、CAP与冠状动脉病变的关系。
1 资料与方法
1.1 一般资料 选取2012年12月—2014年12月在包头医学院第二附属医院心内科行冠状动脉造影者150 例。纳入标准:(1)造影前进行NT-proBNP和无创CAP检查;(2)无心力衰竭。排除标准:既往行经皮冠状动脉介入(PCI)术、陈旧性心肌梗死、呼吸系统疾病、继发性高血压、肾功能不全及内分泌疾病(甲状腺功能亢进症、甲状腺功能减退症、Cushing综合征)。根据 SYNTAX积分将所有患者分为冠状动脉正常组(0分,n=50)和冠状动脉病变组(≥1分,n=100),其中冠状动脉病变组又分为:低危组(1~22分,n=40)、中危组(23~32分,n=35)和高危组(≥33分,n=25)。本研究经包头医学院伦理委员会批准,受试者均知情同意并签署知情同意书。
1.2 方法
1.2.1 资料收集 收集所有受试者的一般资料,包括性别、年龄、BMI、血压、血糖、血脂等。
1.2.2 NT-proBNP检测 所有受试者入院后48 h内抽取清晨空腹肘静脉血1.5 ml,注入非抗凝试管中,在4 ℃下以1 000 r/min离心15 min(离心半径为3 cm),采用美国罗氏2010电化学发光免疫分析仪测定血浆NT-proBNP水平。
1.2.3 CAP测量 采用日本欧姆龙公司的无创桡动脉脉波检测装置(HEM9000AI)测量CAP。受试者左手外展,使手腕与心脏处于同一高度,将多点压力传感探头固定在桡动脉处,探头自动寻找最强的桡动脉搏动点,自动采集桡动脉压力波信号,经电脑软件实时转换成中心动脉压力波形,同步检测肱动脉血压,计算并显示出中心动脉收缩压(CSP)、中心动脉舒张压(CDP)及桡动脉增益指数(rAI)。取连续2次测量相对稳定的值作为最后测量值。
1.2.4 冠状动脉造影 由本院2名具有介入资质的高年资医师严格操作。2%利多卡因局部麻醉后经桡动脉穿刺径路行冠状动脉造影,采用碘海醇注射液(山东鲁抗辰欣药业有限公司)按照350 g/L、4~8 ml/次。使用荷兰飞利浦公司生产的H5000数字减影血管造影仪,行常规体位冠状动脉造影。导管到达冠状动脉相应部位后注入造影剂,观察造影剂充盈情况。根据冠状动脉造影结果,按照SYNTAX积分官方网站(www.syntaxscore.com)所提供的16节段分类法和积分法则,结合患者各自的冠状动脉优势类型、病变的总数、病变累及血管节段及各种病变特征(如完全闭塞、钙化、扭曲、弥漫病变等),每一处病变单独计分,计算SYNTAX积分。

2 结果
2.1 4组一般资料比较 冠状动脉正常组中,男24例,女26例;冠状动脉病变组中,低危组男20例,女20例;中危组男17例,女18例;高危组男12例,女13例。4组性别间差异无统计学意义(χ2=0.042,P=0.998)。4组年龄、BMI、收缩压(SBP)、空腹血糖(FPG)、总胆固醇(TC)、三酰甘油(TG)、低密度脂蛋白胆固醇(LDL-C)间差异有统计学意义(P<0.05);而舒张压(DBP)、高密度脂蛋白胆固醇(HDL-C)间差异无统计学意义(P>0.05,见表1)。
2.2 4组NT-proBNP、CAP比较 4组NT-proBNP、CSP间差异有统计学意义(P<0.05),而CDP间差异无统计学意义(P>0.05,见表2)。
2.3NT-proBNP水平与SYNTAX积分的相关性分析NT-proBNP水平与SYNTAX积分呈直线正相关(r=0.870,P<0.001,见图1)。2.4CSP水平与SYNTAX积分的相关性分析CSP水平与SYNTAX积分呈直线正相关(r=0.743,P<0.001,见图2)。

表1 4组一般资料比较
注:与冠状动脉正常组比较,aP<0.05;与低危组比较,bP<0.05;与中危组比较,cP<0.05;d为Z值;SBP=收缩压,DBP=舒张压,FPG=空腹血糖,TC=总胆固醇,TG=三酰甘油,LDL-C=低密度脂蛋白胆固醇,HDL-C=高密度脂蛋白胆固醇;1 mm Hg=0.133 kPa
表2 4组NT-proBNP、CAP水平比较
注:与冠状动脉正常组比较,aP<0.05;与低危组比较,bP<0.05;与中危组比较,cP<0.05;d为Z值;NT-proBNP=N末端B型利钠肽原,CAP=中心动脉压,CSP=中心动脉收缩压,CDP=中心动脉舒张压
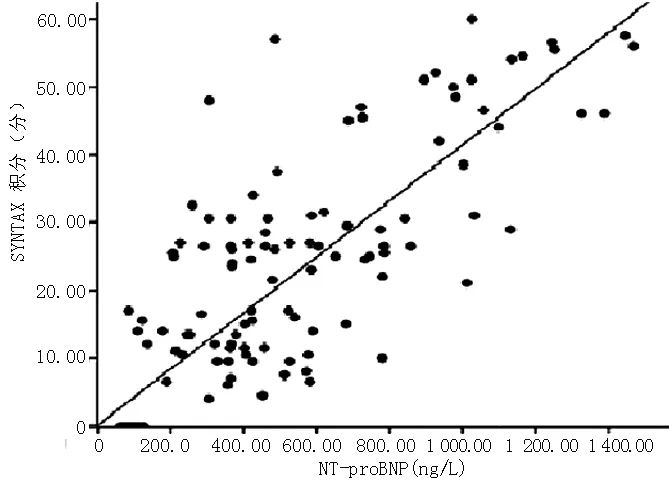
注:NT-proBNP=N末端B型利钠肽原
3 讨论
冠状动脉造影作为临床应用中诊断冠心病的“金标准”,是冠状动脉病变的量化方法。SYNTAX 积分是一种新的根据冠状动脉病变解剖特点(病变位置、严重程度、分叉、钙化等)进行危险分层的积分系统,可定量评价冠状动脉病变的复杂程度[6-8],指导治疗措施的选择。
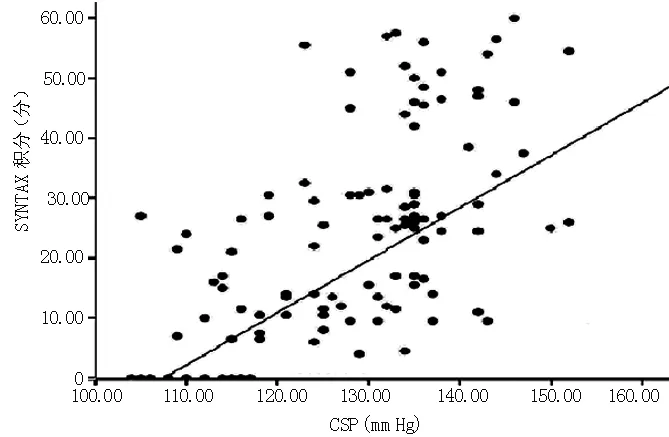
注:CSP=中心动脉收缩压;1 mm Hg=0.133 kPa
B型利钠肽(BNP)是一种在心室肌中合成与分泌的多肽类激素,NT-proBNP是BNP经丝氨酸蛋白酶剪切后形成的,NT-proBNP较BNP t1/2长,含量也相对较高,在正常生理状态下,NT-proBNP在心室肌中很少表达。当心肌缺血,心室容量负荷或压力负荷增加或心室壁应力升高时,其合成与释放陡增[9]。目前临床中已有研究提出冠心病患者血浆NT-proBNP水平与冠状动脉病变程度存在一定的相关性[4]。本研究结果显示,冠状动脉病变越重的患者NT-proBNP水平越高,说明NT-proBNP与心肌缺血坏死的程度有关。相关性分析结果显示,NT-proBNP水平与SYNTAX积分呈直线正相关。不仅如此,在基因微观层面,也有研究发现缺血心肌的周围细胞中NT-proBNP的基因转录明显增加[10-13]。宏观微观二者充分说明心肌缺血是独立诱导NT-proBNP升高的因素。
CAP是指升主动脉根部的血管壁所承受的压力,是左心室收缩射血和血管阻力及血管内血液充盈压共同形成的压力[14]。血管僵硬度越大,外周动脉压与CAP越不完全平行[15-17]。在预测、决定终点事件方面CAP的意义优于外周动脉压[18]。故本研究以冠状动脉造影结果为基础,通过SYNTAX 积分将冠状动脉病变分为低、中、高危组,比较CAP的差异,结果表明,随着冠状动脉病变的加重,CSP逐渐增加,而CDP并无明显变化。相关性分析结果显示,CSP水平与SYNTAX 积分呈直线正相关。
年龄、BMI、SBP、FPG、LDL-C是冠状动脉病变的传统危险因素[19],本研究在此基础上表明,NT-proBNP、CSP可能是冠状动脉病变的相关危险因素,与林艳丽等[13]的研究结果一致。目前,冠状动脉病变诊断技术中,心电图、动态心电图、运动平板试验等都是早期的筛查方法,冠状动脉造影仍是较准确的诊断方法。冠状动脉病变患者预后的评估需要综合年龄、BMI、SBP、FPG、LDL-C、NT-proBNP、CSP等危险因素。
总之,NT-proBNP、CSP与冠状动脉病变有关,随着NT-proBNP、CSP水平的上升,冠状动脉病变程度逐渐加重。NT-proBNP是心力衰竭患者的检测指标[20],CSP对高血压的预后有重要作用[21],同时临床医生也需注意其与冠状动脉病变的相关性。
作者贡献:黄冠华进行试验设计与实施、撰写论文、成文并对文章负责;张顺祥、冯美云进行试验实施、评估、资料收集;王丛进行质量控制与审校。
本文无利益冲突。
[1]黄建萍,茆汉梅,糜跃萍,等.南通市2007—2010年心脑血管疾病死因分析[J].中国卫生统计,2013,30(1):100-101. HUANG J P,MAO H M,MI Y P,et al.Analysis on the cause of death of cardiovascular and cerebrovascular diseases in Nantong City during 2007—2010[J].Chinese Journal of Health Statistics,2013,30(1):100-101.
[2]谭学君.心脑血管疾病的危险因素及预防方法分析[J].现代诊断与治疗,2014,21(7):1604-1605. TAN X J.Analysis on the risk factors and prevention methods of cardiovascular and cerebrovascular diseases[J].Mod Diagn Treat,2014,21(7):1604-1605.
[3]李秀清.心脑血管疾病的危险因素及预防方法分析[J].亚太传统医药,2012,8(1):179-181. LI X Q.Analysis on the risk factors and prevention methods of cardiovascular and cerebrovascular diseases[J].Asia-Pacific Traditional Medicine,2012,8(1):179-181.DOI:10.3969/j.issn.1673-2197.2012.01.098.
[4]AGABITI R E,MANCIA G,O′ROURKE M F,et al.Central blood pressure measurements and antihypertensive therapy:a consensus document[J].Hypertension,2007,50(1):154-160.
[5]SHAHABI V,MOAZENZADEH M,AZIMZADEH B S,et al.Relationship between serum N-terminal pro brain natriuretic peptide(NT-ProBNP) level and the severity of coronary artery involvements[J].J Res Med Sci,2011,16(2):143-148.
[6]中华医学会心血管病学分会介入心脏病学组,中华心血管病杂志编辑委员会.中国经皮冠状动脉介入治疗指南2012[J].中华危重症医学杂志,2012,5(3):169-180. Cardiology Interventional Cardiology Group of Chinese Medical Association,Editorial Committee of Chinese Journal of Cardiology.Guidelines for percutaneous coronary intervention in China 2012[J].Chin J Crit Care Med,2012,5(3):169-180.
[7]FIHN S D,GARDIN J M,ABRAMS J,et al.2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease:executive summary:a report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines,and the American College of Physicians,American Association for Thoracic Surgery,Preventive Cardiovascular Nurses Association,Society for Cardiovascular Angiography and Interventions,and Society of Thoracic Surgeons[J].Circulation,2012,126(25):3097-3137.
[8]Task Force Members,MONTALESCOT G,SECHTEM U,et al.2013 ESC guidelines on the management of stable coronary artery disease:the Task Force on the management of stable coronary artery disease of the European Society of Cardiology[J].Eur Heart J,2013,34(38):2949-3003.
[9]ZHENG J L,LU L,HU J,et al.Increased serum YKL-40 and C-reactive protein levels are associated with angiographic lesion progression in patients with coronary artery disease[J].Atherosclerosis,2010,210(2):590-595.
[10]牛方清,刘伟昌,窦晋景.NT-proBNP与超敏C反应蛋白在心衰患者中的相关性研究[J].医学理论与实践,2013,26(2):143-144. NIU F Q,LIU W C,DOU J J.Investigation about the relativity between N-terminal pro-brain natriuretic peptide and high sensitive C-relative protein in patients with heart failure[J].J Med Theor & Prac,2013,26(2):143-144.
[11]武春燕,王桂红,刘玫,等.BNP联合cTn-I对急性心肌梗死的诊断价值[J].中西医结合心脑血管病杂志,2013,11(1):122. WU C Y,WANG G H,LIU M,et al.Value of BNP combined with cTn-I in the diagnosis of acute myocardial infarction[J].Chinese Journal of Integrative Medicine on Cardio-/Cerebrovascular,2013,11(1):122.DOI:10.3969/j.issn.1672-1349.2013.01.070.
[12]李杰.急性冠脉综合征患者血清BNP水平与冠状动脉病变关系研究[J].中国医药科学,2013,3(2):121. LI J.Study on the relationship between serum BNP levels of patients with acute coronary ayndrome and coronary artery lesions[J].China Medicine and Phamacy,2013,3(2):121.
[13]林艳丽,徐裔婷,傅雷,等.急性心肌梗死患者CRP、NT-proBNP和血脂的变化[J].放射免疫学杂志,2013,26(1):33-34. LIN Y L,XU Y T,FU L,et al.Changes of CRP,NT-proBNP and serum lipids in patients with acute myocardial infarction[J].Journal of Radioimmunology,2013,26(1):33-34.DOI:10.3969/j.issn.108-9810.2013.01.015.
[14]HOLMES R S,VAUGHAN T L.Epidemiology and pathogenesis of esophageal cancer[J].Semin Radiat Oncol,2007,17(1):2-9.
[15]MCENIERY C M,YASMIN M C,DONNELL B,et al.Central pressure:variaility and impact of cardiovascular risk factors:the anglo-cardiff collaborative trial II[J].Hypertension,2008,51(6):1476-1482.
[16]ROMAN M J,DEVEREUX R B,KIZER J R,et al.High central pulse pressure is independently associated with adverse cardiovascular outcome the strong heart study[J].J Am Coll Cardiol,2009,54(18):1730-1734.
[17]ROMAN M J,DEVEREUX R B,KIZER J R,et al.Central pressure more strongly relates to vascular disease and outcome than does brachial pressure:the Strong Heart Study[J].Hypertension,2007,50(1):197-203.
[18]AGABITI R E,MANCIA G,O′ROURKE M F,et al.Central blood pressure measurements and antihypertensive therapy:a consensus document[J].Hypertension,2007,50(1):154-160.
[19]LAWES C M,VANDER H S,RODGERS A.Global burden of blood-pressure-related disease,2001[J].Lancet,2008,371(9623):1513-1518.
[20]王喆.《中国心力衰竭诊断和治疗指南2014》解读[J].中国临床医生杂志,2016,44(5):14-16. WANG Z.Interpretation of guidelines for the diagnosis and treatment of heart failure in China 2014[J].Chin J Clinicians,2016,44(5):14-16.DOI:10.3969/j.issn.2095-8552.2016.05.006.
[21]王恺皞,蒋雄京.年轻单纯收缩期高血压患者中心动脉压测量的特殊意义[J].中华高血压杂志,2016,24(2):132-134. WANG K H,JIANG X J.Special significance of the measurement of central arterial pressure in young patients with simple systolic hypertension[J].Chin J Hypertens,2016,24(2):132-134.
(本文编辑:崔沙沙)
Correlation of NT-proBNP and Central Aortic Pressure Levels with the Severity of Coronary Artery Disease
HUANGGuan-hua,WANGCong,ZHANGShun-xiang,FENGMei-yun.
DepartmentofCardiology,theSecondAffiliatedHospitalofBaotouMedicalCollege,Baotou014030,China
Correspondingauthor:WANGCong,DepartmentofCardiology,theSecondAffiliatedHospitalofBaotouMedicalCollege,Baotou014030,China;E-mail:wangcong65@126.com
Objective To investigate the correlation of NT-proBNP and central aortic pressure(CAP) levels with the severity of coronary artery disease.Methods One hundred and fifty patients undergoing coronary angiography in Department of Cardiology,the Second Affiliated Hospital of Baotou Medical College from December 2012 to December 2014 were selected as the subjects.In accordance with the SYNTAX scores,they were assigned to normal coronary artery group(0 point,n=50) and coronary lesions group(≥1 point,n=100),and the coronary lesions group was further divided into low-risk subgroup(1~22 points,n=40),medium-risk subgroup(23~32 points,n=35) and high-risk subgroup(≥33 points,n=25).The general information was collected,including gender,age,BMI,blood pressure,blood glucose,blood lipids and so on.Plasma NT-proBNP level was measured by American roche 2010 electrochemiluminescence immunoassay analyzer.CAP was measured by Japan′s Omron′s non-invasive radial artery pulse wave detection device(HEM9000AI).Results Compared normal coronary group with low-risk subgroup,medium-risk subgroup and high-risk subgroup,there was statistically significant difference in terms of age,BMI,systolic blood pressure(SBP),fasting plasma glucose(FPG),total cholesterol(TC),triglyceride(TG) and low density lipoprotein cholesterol(LDL-C)(P<0.05) but not in sex,diastolic blood pressure(DBP) and high density lipoprotein cholesterol(HDL-C)(P>0.05),and significant difference was found in terms of the level of NT-proBNP and CSP between the groups(P<0.05),but not in the level of CDP(P>0.05).The level of NT-proBNP had a linear positive correlation with the SYNTAX scores of coronary artery disease(r=0.870,P<0.001).And it showed a linear positive correlation statistically between the level of CSP and the SYNTAX scores of coronary artery disease(r=0.743,P<0.001).Conclusion Both NT-proBNP and CSP levels are positively correlated with coronary artery disease.And with the elevation of NT-proBNP and CSP levels,the severity of coronary artery disease increases.
N-terminal pro-brain natriuretic peptide;Central aortic pressure;Coronary artery disease
014030内蒙古包头市,包头医学院第二附属医院心内科
王丛,014030内蒙古包头市,包头医学院第二附属医院心内科;E-mail:wangcong65@126.com
R 543.3
A
10.3969/j.issn.1007-9572.2016.34.012
2016-07-07;
2016-10-26)
