儿童及青年预激综合征患者的临床及电生理特点分析
2014-05-03钱炜春张丰富丁竞竞贾海波
钱炜春,张丰富,丁竞竞,贾海波
(1.南京医科大学附属南京医院南京市第一医院心脏内科,江苏 南京 210006;2.南京医科大学公共卫生学院,江苏 南京 210000)
儿童及青年预激综合征患者的临床及电生理特点分析
钱炜春1,张丰富1,丁竞竞2,贾海波1
(1.南京医科大学附属南京医院南京市第一医院心脏内科,江苏 南京 210006;2.南京医科大学公共卫生学院,江苏 南京 210000)
目的评价小于30岁的预激综合征(WPW)特别是小于18岁患者的电生理特性及射频消融的效果。方法300例预激综合征患者入选,按照年龄分为三组,A组6~17岁,B组18~29岁,C组30~75岁。通过回顾医疗记录的方法分别评价三组的临床特点、电生理特性及治疗效果。结果在所有的预激综合征患者中,110例(36.67%)小于30岁。B组中男性多于女性(男:女=50:13),A组中性别差异无统计学意义(男:女=24:23)。左侧旁道在A组(25.5%,12/47)中的比例小于B组(50.8%,32/63)及C组(55.8%,106/190),差异有统计学意义(χ2=14.3,P=0.03)。三组患者的射频消融手术成功率为A组87.2%(41/47),B组92.1%(58/63),C组94.2%(179/190),A组低于B组和C组,差异有统计学意义(χ2=11.6,P=0.02)。结论此研究阐述了儿童及青年预激综合征患者不同的临床及电生理特性,儿童左侧旁道发病率较低,且手术成功率相对较低。
预激综合征;旁道;电生理;导管射频消融
预激综合征的人群发病率为0.1%~0.3%[1]。预激综合征易发生阵发性室上性心动过速,发生率大于40%将极大降低患者的生活质量。射频消融术是针对预激综合征一个安全而有效的根治方法,其成功率达95.0%以上[2-5]。通过电生理检查的方法可以明确预激综合征患者的旁路电生理特性,如旁路的位置,从而指导射频消融术[6-8]。已有研究提示不同年龄的患者表现出不同的临床及电生理特点[9-15]。本研究的目的是阐述小于30岁,特别是小于18岁的预激综合征患儿的电生理特性及其射频消融的效果。
1 资料与方法
1.1 一般资料 选取2009-2012年在南京市第一医院行电生理检查及射频消融术的年龄为7~75岁的300例预激综合征患者。
1.2 方法 患者按年龄分为三组,A组6~17岁,共47例;B组18~29岁,共63例;C组30~75岁,共190例。所有患者均行电生理检查明确旁路的位置,其中一部分患者同时测定旁道的有效不应期。旁道的有效不应期(ERP)定义为通过递增起搏法得出的使旁道出现室房分离的最长联律间期。通过连续性、递增起搏心房或者心室刺激诱发房室折返性心动过速及房颤。本研究中所有患者经电生理检查明确旁道的位置后,出现手术指征(心动过速、房颤发作等),或此患者要求消除预激波恢复正常心电图,均行标准射频消融术。射频消融成功定义为预激波消失,通过心房顺行刺激及心室逆行刺激无偏心性传导出现至少30 min以上。
1.3 统计学方法 采用SPSS11.0统计学软件完成数据分析,三组患者的年龄比较选用One-Way ANOVA检验,临床及电生理频数数据使用χ2检验,ERP的相关性分析使用Pearson相关检验,以P<0.05表示差异有统计学意义。
2 结果
2.1 三组患者的临床资料比较 所有患者的临床数据见表1。A组男性24例,女性23例;B组中男性50例,女性13例;C组中男性126例,女性64例。B组及C组中的男性多于女性,A组中男女比例差异无统计学意义。此次研究随访时间均为(12.0±2.1)个月。
表1 不同组间的临床数据比较[,例(%)]
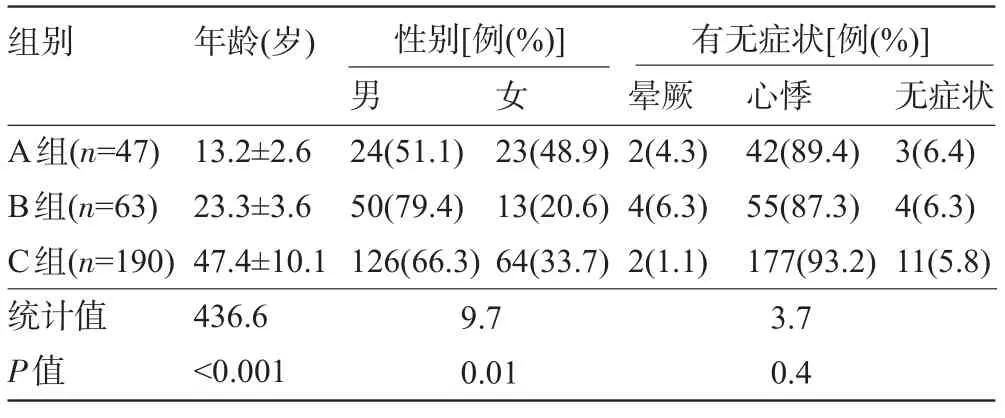
表1 不同组间的临床数据比较[,例(%)]
24(51.1) 50(79.4) 126(66.3) 23(48.9) 13(20.6) 64(33.7) 2(4.3) 4(6.3) 2(1.1) 42(89.4) 55(87.3) 177(93.2) 3(6.4) 4(6.3) 11(5.8) A组(n=47) B组(n=63) C组(n=190)统计值P值13.2±2.6 23.3±3.6 47.4±10.1 436.6<0.001 9.7 0.01 3.7 0.4
2.2 三组患者的电生理数据比较 患者的电生理数据见表2。通过电生理检查可以发现,A组发生心房纤颤的比例低于B组和C组,差异具有统计学意义(χ2=12.9,P=0.01)。三组患者中,前间隔旁道患者在各组中所占比例非常接近。而左侧旁道患者在各组中所占比例:A组明显低于B组及C组,三组患者旁道位置的构成差异具有统计学意义(χ2=14.3,P= 0.03)。三组患者的手术成功率:A组低于B组和C组,差异具有统计学意义(χ2=11.6,P=0.02)。A组中出现5例特殊类型,3例为先天性心脏病,均为埃勃斯坦畸形,2例为扩张性心肌病,而B组及C组中均未见合并特殊类型心脏疾病。本研究共测试了20例患者的ERP,其中B组4例,C组16例。旁道的ERP与年龄的关系经Pearson相关检验,提示可能呈正相关,但差异无统计学意义(r=0.4,P=0.09)。

表2 不同组间电生理及射频消融数据[例(%)]
3 讨论
预激综合征是一种先天性的发育异常[16]。预激综合征在婴儿期常自行消失而在儿童期时可能会再次出现[17-19]。从本研究可以看出,儿童预激综合征的特点有:(1)无性别差异;(2)左侧旁道的发生率比其他年龄组低;(3)手术成功率相对较低。
流行病学研究表明,预激综合征的发病率在不同性别中是有差异的。然而,有研究报道表明14岁以下男性儿童预激综合征的比例为47.0%,女性的比例为53.0%,无性别差异。而随着年龄的增加,男性预激综合征患者的比例逐渐增多。在15~16岁年龄段的男性患者的比例为60.0%,17岁以上患者中该比例为69.0%[20-21]。本研究亦证实在儿童患者中预激综合征无性别差异,而成年预激综合征男性患者比例大于女性。
本研究探讨了多种旁道类型与年龄的关系,发现左侧旁道的发生率与年龄有一定关系。Brembilla-Perrot等[22]研究发现随着预激综合征患者年龄的增大,左侧旁道的发生率亦随之升高。本研究也有相似的结果,大于18岁的左侧旁道患者所占比例高于小于18岁患者。而前间隔旁道的发生率同年龄无明显的相关性。
本研究发现儿童患者中房颤的发生率最小,无论是经体表心电图房颤检出率还是电生理检查中房颤诱发率均低于大于18岁的预激综合征患者,同Brembilla-Perrot等[22]研究结果相似。
多个研究证实,旁道的有效不应期随着年龄的增长而延长[8-13]。但针对预激综合征的电生理检查主要是旁道定位,所以我们没有对大多数的患者测定其旁道不应期。我们总共对20例患者的旁道有效不应期进行了检查,发现随着年龄的增长旁道的有效不应期有所延长但差异无统计学意义。
在本研究中,有5例儿童预激综合征的患者合并特殊类型心脏疾病。这5例患者均为右侧旁道,其中3例为埃勃斯坦畸形,另外2例为扩张型心肌病。Delhaas等[23]研究报道儿童预激综合征易合并埃勃斯坦畸形。且埃勃斯坦畸形患者出现右侧旁道的比例较高,其可能同右心系统发育异常相关。
本研究发现儿童预激综合征行射频消融术的失败率较高。考虑为在儿童患者中,右侧旁道所占的比例较高。因为右心系统的结构特点使导管在消融右侧旁道比左侧旁道是更加难以固定,故造成局部消融温度较低而导致消融手术更易失败或者复发。
本研究的局限在于这是一个较为短期的随访研究,而且未对大多数的患者进行旁道的不应期检查。因此,我们还需要更大样本和中长期的随访来研究儿童及青年预激综合征患者的电生理特性及佐证射频消融手术对此类预激综合征患者的安全性及有效性。
[1]Keating L,Morris FP,Brady WJ.Electrocardiongraphic features of Wolff-Parkinson-White syndrome[J].Emerg Med J,2003,20(5): 491-493.
[2]Chen S,姚 焰.阵发性室上性心动过速的射频消融治疗[J].中华心律失常学杂志,1998,2(3):234-235.
[3]Jackman WM,Wang XZ,Friday KJ,et al.Catheter ablation of accessory atrioventricular pathways(Wolff-Parkinson-White syndrome)by radiofrequency current[J].N Engl J Med,1991,324: 1605-1611.
[4] Calkins H,Sousa J,El-Atassi R,et al.Diagnosis and cure of the Wolff-Parkinson-White syndrome or paroxysmal supraventricular tachycardias during a single electrophysiologic test[J].N Engl J Med,1991,324:1612-1618.
[5]Calkins H,Yong P,Miller JM,et al.Catheter ablation of accessory pathways,atrioventricular nodal reentrant tachycardia,and the atrioventricular junction:final results of a prospective,multicenter clinical trial.The Atakr Multicenter Investigators Group[J].Circulation, 1999,99:262-270.
[6]Santinelli V,Radinovic A,Manguso F,et al.The natural history of asymptomatic ventricular pre-excitation a long-term prospective follow-up study of 184 asymptomatic children[J].J Am Coll Cardiol, 2009,53:275-280.
[7]Pappone C,Manguso F,Santinelli R,et al.Radiofrequency ablation in children with asymptomatic Wolff-Parkinson White syndrome [J].N Engl J Med,2004,351:1197-205.
[8]Pappone C,Santinelli V,Manguso F,et al.A randomized study of prophylactic catheter ablation in asymptomatic patients with the Wolff-Parkinson-White syndrome[J].N Engl J Med,2009,349: 1803-1811.
[9]Chiu SN,Wang JK,Wu MH,et al.Cardiac conduction disturbance detected from a large-scale pediatric population electrocardiographic screening:prevalence and implications[J].J Pediatr,2008,152: 85-89.
[10]Magalski A,Mccoy M,Zabel M,et al.Cardiovascular screening with electrocardiography and echocardiography in collegiate athletes[J].Am J Med,2011,124:511-518.
[11]Udink ten cate FE Udink,Kruessell MA,Wagnerk,et al.Dilated cardiomyopathy in children with ventricular preexcitation:the location of the accessory pathway is predictive of this association[J].J Electrocardiol,2010,43:146-154.
[12]Chiu SN,Chang CW,Lu CW,et al.Restored cardiac function after successful resynchronization by right anterior and anteroseptal accessory pathway ablation in Wolff-Parkinson-White syndrome associated dilated cardiomyopathy[J].Int J Cardiol,2013,163:19-20.
[13]黄 敏,华仰德,王健怡,等.射频消融治疗儿童室上性心动过速的应用体会[J].中国介入心脏病学杂志,2001,9(1):6-7.
[14]Huttin O,Brembilla-Perrot B.Relationships between age and accessory pathway location in Wolff-Parkinson-White syndrome[J].Ann CardiolAngeiol(Paris),2008,57:225-230.
[15]Rodriguez LM,de Chillou C,Schläpfer J,et al.Age at onset and gender of patients with different types of supraventricular tachycardias[J].Am J Cardiol,1992,70:1213-1215.
[16]Wu MH,Chen HC,Lu CW,et al.Prevalence of congenital heart disease at live birth in Taiwan[J].J Pediatr,2010,156:782-785.
[17]Mosaed P,Dalili M,Emkanjoo Z.Interventional electrophysiology in children:a single-center experience[J].Iran J Pediatr,2012,22: 333-338.
[18]Santinelli V,Radinovic A,Pappone C,et al.The natural history of asymptomatic ventricular preexcitation:a long-term prospective follow-up study of 184 asymptomatic children[J].J Am Coll Cardiol, 2009,53:275-280.
[19]Wackel P,Irving C,Webber S,et al.Risk stratification in Wolff-Parkinson-White syndrome:the correlation between noninvasive and invasive testing in pediatric patients[J].PACE,2012,35: 1451-1457.
[20]Sano S,Komori S,Amano T,et al.Prevalence of ventricular preexcitation in Japanese school children[J].Heart,1998,79:374-378.
[21]Liu S,Yuan S,Hertervig E,et al.Gender and atrioventricular conduction properties of patients with symptomatic atrioventricular nodal reentrant tachycardia and Wolff-Parkinson-White syndrome [J].J Electrocardiol,2001,34:295-301.
[22]Brembilla-Perrot B,YangniN'da O,Huttin O,et al.Wolff-Parkinson-White syndrome in the elderly:clinical and electrophysiological findings[J].Arch Cardiovasc Dis,2008,101:18-22.
[23]Delhaas T,Sarvaas GJ,Rijlaarsdam ME,et al.A multicenter,long-term study on arrhythmias in children with Ebstein anomaly[J].Pediatr Cardiol,2010,31:229-233.
Clinical and electrophysiological characteristics in children and adolescence with Wolff-Parkinson-White
syndrome.
QIAN Wei-chun1,ZHANG Feng-fu1,DING Jing-jing2,JIA Hai-bo1.
1.Department of Cardiology,NanjingFirst Hospital,Nanjing Hospital Affiliated to Nanjing Medical University,Nanjing 210006,Jiangsu,CHINA;2.Public Health College of Nanjing Medical University,Nanjing 210000,Jiangsu,CHINA
ObjectiveTo evaluate the characteristics of electrophysiologic studies(EPS)and radiofrequency ablation(RFA)performed in subjects aged less than 30 years with Wolff-Parkinson White(WPW)syndrome,particularly pediatric patients under 18 years of age,based on our experience.MethodsThree hundred consecutive patients with WPW syndrome were recruited and divided to three groups according to age:group A(6~17 years old),group B (18~29 years old),group C(30~75 years old).The clinical,electrophysiological,and therapeutic data for these patients were evaluated by a retrospective medical record review.ResultsA total of 110(36.67%)of these patients were<30 years of age.There were significantly more males than females in group B(male:female,50:13),and there was no significant difference in gender in group A(male:female,24:23).Left accessory pathway was detected less frequently in group A(25.53%,12/47)than in group B(50.79%,32/63)and group C(55.79%,106/190),χ2=14.31, P=0.03.The surgical success rate of radiofrequency ablation was 87.2%(41/47)in group A,92.1%(58/63)in group B,and 94.2%(179/190)in group C,which was significantly lower in group A than group B and group C(χ2=11.6, P=0.02).ConclusionThis study describes several different electrophysiological characteristics in children and adolescents with WPW syndrome.Children have lower incidence of left side accessory pathway,and the surgery successful rate of them are lower.
Wolff-Parkinson-White syndrome;Accessory pathway;Electrophysiology;Radiofrequency ablation(RFA)
R442.8
A
1003—6350(2014)24—3646—03
10.3969/j.issn.1003-6350.2014.24.1421
2014-07-15)
江苏省临床医学科技专项(编号:BL2013001)
贾海波。E-mail:qccdjj12345@aliyun.com