逆行自体血预充对围术期临床结果影响的荟萃分析
2014-03-13吉冰洋孙燕华刘晋萍
孙 鹏,吉冰洋,孙燕华,朱 贤,刘晋萍,龙 村
·临床研究·
逆行自体血预充对围术期临床结果影响的荟萃分析
孙 鹏,吉冰洋,孙燕华,朱 贤,刘晋萍,龙 村
目的对逆行自体血预充(RAP)对围术期临床结果的影响进行荟萃分析。方法 对PubMed、Embase、Cochrane Library、Google Scholar、万方、维普以及中国知网数据库中关于在成人患者中应用RAP的随机对照试验(RCT)进行全面检索,观察的临床指标包括体外循环(CPB)中最低红细胞比容(Hct)、术中输血的病例数、围术期输血的病例数、总的红细胞用量、术后24 h胸液引流量、拔管时间、ICU留观时间和总住院时间。结果共10篇RCT入选。RAP组与对照组比较,CPB中最低Hct(P<0.01)和术后24 h胸液引流量(P<0.01)优于对照组,而总住院时间(P>0.05)无统计学差异,但因异质性较大(I2>50%),其临床效果无法评估。RAP组术中输血的患者数(P<0.01)、围术期输血的患者数(P<0.01)及红细胞用量(P<0.01)均显著低于对照组,而两组患者的拔管时间(P>0.05)和ICU留观时间(P>0.05)无统计学差异。结论RAP可显著减少成人患者围术期输血,其对患者预后的影响,较传统预充方法无统计学差异。
逆行自体血预充;预充量;输血;临床结果;体外循环
目前在体外循环(cardiopulmonary bypass,CPB)中减少患者输血的方式包括使用血液回收、血液超滤、减少预充量等。Rosengart等于1998年首次提出“逆行自体血预充”(retrograde autologous prim⁃ing,RAP)的理念,即在CPB开始前通过引流患者自身血液,置换CPB动静脉管路、动脉微栓过滤器、静脉储血室及氧合器内的晶体预充液,有效的降低预充量,减轻血液稀释,提高转流中红细胞比容(Hct),减少术中和整个围术期输血患者的比例[1]。但在实施RAP时,存在患者部分容量丧失而导致患者血流动力学不稳定、增加静脉端进气和血液破坏的可能性等风险,故对在成人患者中应用RAP的随机对照试验(randomized controlled trial,RCT)文献进行荟萃分析,评估其对患者输血和预后的影响。
1 材料和方法
1.1 研究设计 本荟萃分析所关注的临床终点是使用和未使用RAP对成人CPB心脏手术患者的输血需求及术后恢复情况的影响。研究设计均遵循系统评价和荟萃分析优化报告的PRISMA声明[2]。
1.2 检索和入选标准 对PubMed、Embase、Co⁃chrane Library、Google Scholar、万方、维普以及中国知网等中、英文数据库中关于RAP的RCT文献进行检索。使用的检索关键词包括“retrograde autolo⁃gous priming/逆行自体血预充”、“cardiac surgery/心脏手术”、“cardiopulmonary bypass/体外循环”、“ex⁃tracorporeal circulation/体外循环”、“prime/预充”及“priming/预充”。检索过程对语言、发表日期和发表状态均无限制。比较使用和未使用RAP对成人心脏手术患者围术期输血及预后影响的RCT文献入选本荟萃分析。入选研究的质量评价依据Jadad评分进行[3]。
1.3 文献和数据采集 通过阅读标题和摘要,从1 953篇可能与RAP相关的研究中检索到58篇在CPB中应用RAP的相关研究。阅读全文后排除8篇非成人心脏手术,2篇无相关临床终点,6篇联合RAP和其他干预手段(如急性等容性血液稀释、术中自体放血、缩短管道等)以及32篇非RCT研究,最后得到10篇符合入选标准的研究,共计1 123例患者纳入本荟萃分析[17-15]。入选RCT的主要信息见表1,其中Jadad评分的平均值为1.6分(1到3分)。
将10篇RCT文献中使用RAP(RAP组)和未使用RAP(对照组)所得到的CPB中最低Hct值、输血病例数、围术期输血例数、红细胞用量、术后24 h胸液引流量、拔管时间、ICU停留时间、总住院时间等数据进行合并比较。
1.4 统计分析 使用的统计软件为 RevMan5.1 (version 5.1.Copenhagen:The Nordic Cochrane Cen⁃tre,The Cochrane Collaboration,2011)。合并数据的效应量时,二分类变量使用相对危险度(relative risk,RR)及95%可信区间(confidence interval,CI),连续变量使用标准化均数差(standardised mean difference,SMD)及95%CI。合并统计量时,根据异质性决定统计模型的类型。各研究间的异质性使用I2和Q检验进行评估。异质性较小(I2<50%或P >0.1)时使用固定效应模型(fixed effect model),反之使用随机效应模型(random effect model)。P<0.05认为有统计学意义。
2 结 果
各文献中报道的两组采集的数据合并效应量后的比较结果见表2。
6篇文献报道了666例患者CPB中最低Hct,RAP组CPB中最低Hct要显著高于对照组,各研究间异质性较大。
7篇研究报道了779例患者有151例在术中输血,RAP组输血例数显著少于对照组,各研究间异质性无统计学差异。
4篇研究报道了394例患者中有192例在围术期输血,RAP组病例数显著少于对照组,各研究间异质性无统计学差异。
5篇研究报道了414例患者的红细胞用量,RAP组总的红细胞用量显著少于对照组,各研究间异质性无统计学差异。
表1 入选研究文献的主要信息(±s)
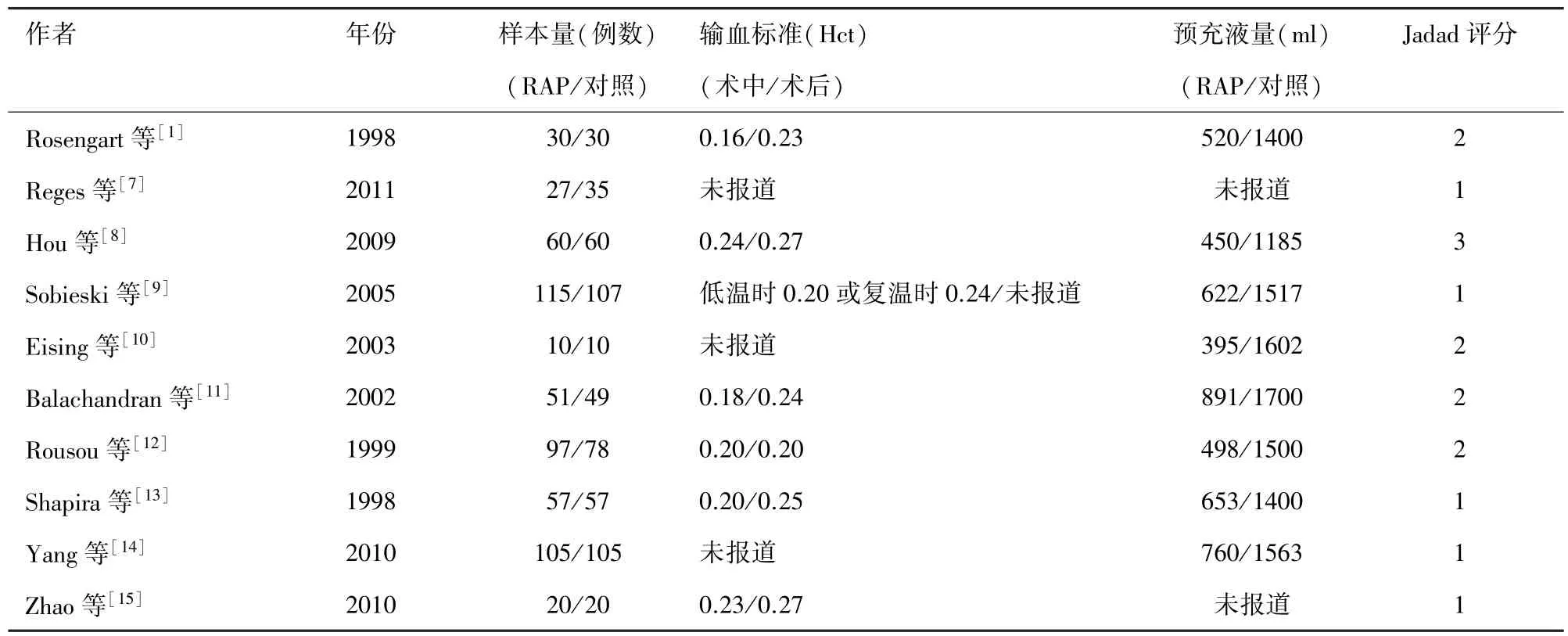
表1 入选研究文献的主要信息(±s)
作者 年份 样本量(例数) 输血标准(Hct) 预充液量(ml) Jadad评分(RAP/对照) (术中/术后) (RAP/对照)Rosengart等[1]1998 30/30 0.16/0.23 520/1400 2 Reges等[7]2011 27/35 未报道 未报道 1 Hou等[8]2009 60/60 0.24/0.27 450/1185 3 Sobieski等[9]2005 115/107 低温时0.20或复温时0.24/未报道 622/1517 1 Eising等[10]2003 10/10 未报道 395/1602 2 Balachandran等[11]2002 51/49 0.18/0.24 891/1700 2 Rousou等[12]1999 97/78 0.20/0.20 498/1500 2 Shapira等[13]1998 57/57 0.20/0.25 653/1400 1 Yang等[14]2010 105/105 未报道 760/1563 1 Zhao等[15]2010 20/20 0.23/0.27 未报道 1
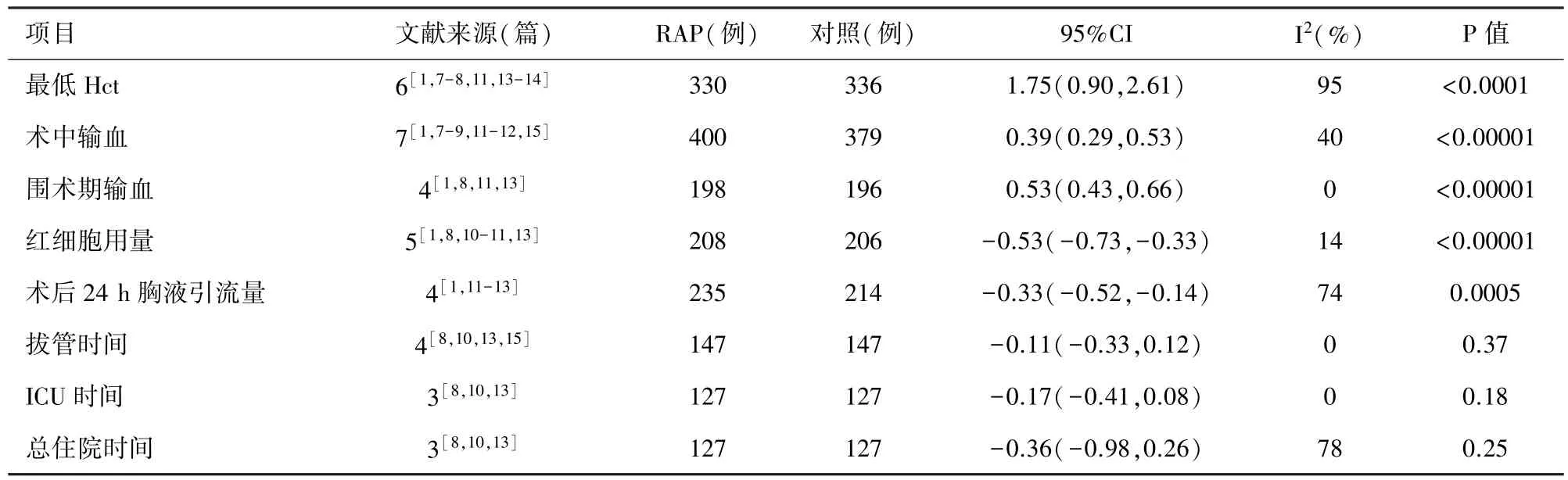
表2 文献来源两组数据比较结果
4篇研究报道了449例患者的术后24 h胸液引流量,RAP组显著少于对照组,各研究间异质性较大。
4篇研究报道了294例患者拔管时间,两组患者的拔管时间无显著差异,各研究间异质性无统计学差异。
3篇研究报道了254例患者ICU留观时间和总住院时间,两组间患者的均无显著差异。ICU留观时间各研究间异质性无统计学差异,总住院时间各研究间异质性较大。
3 讨 论
输血作为外科手术中重要的补充血红蛋白增加机体氧供和补充凝血因子的有效手段应用于临床已经拯救了数以万计的患者,但输血同时也会使患者面临诸多风险,如发生血源性传染病的播散、感染、肾衰、肺损伤、通气时间延长、住院时间延长以及死亡率增加等[4-6]。输血导致的这些并发症会进一步增加患者住院期间的费用[16]。因此,如何减少输血是目前临床工作中的一个重点。
2009年Saczkowski等就RAP对患者CPB中用血情况的影响进行了荟萃分析[17]。共入选了6篇研究,结论是RAP可减少输血的病例数及红细胞用量,但未分析RAP对患者预后的影响。本荟萃分析在包含Saczkowski入选的6篇研究的基础上,增加之后发表的4篇RCT文献,荟萃分析结果显示,RAP可显著降低患者围术期输血,这与Saczkowski报道的结果一致。有大样本的研究证明减少患者心脏手术围术期的输血,可降低一系列近期和远期并发症,促进预后[4-6]。而本研究结果是两组患者在拔管时间、ICU留观时间和总住院时间无统计学差异,未发现其对患者术后有改善作用,分析导致此现象出现的原因可能是纳入的研究样本量较小,无法观察到RAP对患者术后影响的阳性结果。
在对术中最低Hct、术后24 h胸液引流量和总住院时间进行数据分析时发现,各研究间的异质性均较大(I2>50%),分析其原因可能是RAP时的步骤、RAP中使用血管活性药物的情况、入选和排除标准不同所致。本荟萃分析纳入的 10篇研究,其Jadad评分平均仅为1.6分,缺乏高质量、大样本量的双盲RCT文献。说明单一应用RAP的研究还较少,可能与实施RAP时存在的诸多限制有关:①RAP过程中可能存在的血流动力学不稳定。RAP使用患者自体血对CPB环路进行预充,使得患者自身血容量减少,血压下降,此时可适当使用血管收缩药物以维持血压。进行RAP操作时血压应维持在多少目前还没有统一标准;②患者体内血容量较少。RAP实施后开始转流时会导致静脉回流室内血液平面较低,静脉系统可能出现祛除气泡不完全,增加进气的风险。有学者推荐实施RAP后,转流过程中静脉回流室内的液平面应维持在400 ml以上[1];③患者术前Hct较高。这会导致转流中患者Hct较高,增加CPB对血液造成的破坏。
Murphy等在一项大样本的回顾性研究中发现单纯应用RAP对使用红细胞的患者比例仅存在非显著性的降低(P=0.083)[18]。因此,在术中应综合考虑患者的整体情况,RAP联合其他血液保护方式,而非机械性的单纯使用RAP,以达到最佳的血液保护效果,改善患者的预后。有报道称,可通过应用RAP和其他的省血手段,对不接受输血的耶和华见证者成功实施心脏手术[19-20]。
联合使用RAP和急性等容性血液稀释或术中自体放血可平衡患者体内容量,维持转流中Hct在较理想水平,减轻血液破坏,减少患者输血,改善预后[21-22]。通过改变主泵和静脉回流室及氧合器位置,使其更靠近患者,缩短不必要的CPB管路长度和尺寸,可进一步减小CPB预充量,达到更佳的血液保护效果[23-24]。抬高CPB系统和使用小尺寸管路会影响静脉系统的重力引流,同时可联合使用负压辅助静脉引流系统,以保证足够的静脉引流[25-26]。有研究者在联合使用RAP和迷你CPB时,亦达到了较理想的省血效果[27-29]。
总之,本荟萃分析显示应用RAP可减少成人患者围术期输血,但未发现其可促进患者术后恢复,可能与入选RCT文献的Jadad评分较低以及样本量较小有关,因此,还需开展大样本的双盲RCT以综合评估其临床效果。
[1] Rosengart TK,DeBois W,O'Hara M,et al.Retrograde autolo⁃gous priming for cardiopulmonary bypass:A safe and effective means of decreasing hemodilution and transfusion requirements [J].J Thorac Cardiovasc Surg,1998,115(2):426-38;discus⁃sion 438-9.
[2] Moher D,Liberati A,Tetzlaff J,et al.Preferred reporting items for systematic reviews and meta-analyses:the PRISMA state⁃ment[J].PLoS Med,2009,21;6(7):e1000097.
[3] Jadad AR,Moore RA,Carroll D,et al.Assessing the quality of reports of randomized clinical trials:is blinding necessary[J]?Control Clin Trials,1996,17(1):1-12.
[4] Society of Thoracic Surgeons Blood Conservation Guideline Task Force,Ferraris VA,Brown JR,et al.2011 update to the society of thoracic surgeons and the society of cardiovascular anesthesiol⁃ogists blood conservation clinical practice guidelines[J].Ann Thorac Surg,2011,91(3):944-982.
[5] Koch CG,Li L,Sessler DI,et al.Duration of red-cell storage and complications after cardiac surgery[J].N Engl J Med,2008,358(12):1229-1239.
[6] Engoren MC,Habib RH,Zacharias A,et al.Effect of blood transfusion on long-term survival after cardiac operation[J].Ann Thorac Surg,2002,74(4):1180-1186.
[7] Reges RV,Vicente WVA,Rodrigues AJ,et al.Retrograde au⁃tologous priming in cardiopulmonary bypass in adult patients:Effects on blood transfusion and hemodilution[J].Rev Bras Cir Cardiovasc,2011,26(4):609-616.
[8] Hou X,Yang F,Liu R,et al.Retrograde autologous priming of the cardiopulmonary bypass circuit reduces blood transfusion in small adults:A prospective,randomized trial[J].Eur J Anaes⁃thesiol,2009,26(12):1061-1066.
[9] Sobieski MA 2nd,Slaughter MS,Hart DE,et al.Prospective study on cardiopulmonary bypass prime reduction and its effect on intraoperative blood product and hemoconcentrator use[J].Perfusion,2005,20(1):31-37.
[10] Eising GP,Pfauder M,Niemeyer M,et al.Retrograde autolo⁃gous priming:Is it useful in elective on-pump coronary artery bypass surgery[J]?.Ann Thorac Surg,2003,75(1):23-27.
[11] Balachandran S,Cross MH,Karthikeyan S,et al.Retrograde autologous priming of the cardiopulmonary bypass circuit re⁃duces blood transfusion after coronary artery surgery[J].Ann Thorac Surg,2002,73(6):1912-1918.
[12] Rousou JA,Engelman RM,Flack JE 3rd,et al.The'prime⁃less pump':A novel technique for intraoperative blood conser⁃vation[J].Cardiovasc Surg,1999,7(2):228-235.
[13] Shapira OM,Aldea GS,Treanor PR,et al.Reduction of allo⁃geneic blood transfusions after open heart operations by lowering cardiopulmonary bypass prime volume[J].Ann Thorac Surg, 1998,65(3):724-730.
[14] 杨璟,何美玲,赵岩岩,等.自体血逆行预充在体外循环中应用的探讨[J].中国体外循环杂志,2010,8(2):83-85.
[15] 赵岩岩,杨璟,董培青.自体血逆行预充对体外循环期间血液有形成分影响的观察[J].中国体外循环杂志,2010,8 (2):86-89.
[16] Stokes ME,Ye X,Shah M,et al.Impact of bleeding-related complications and/or blood product transfusions on hospital costs in inpatient surgical patients[J].BMC Health Services Research,2011,11(1):135.
[17] Saczkowski R,Bernier PL,Tchervenkov CI,et al.Retrograde autologous priming and allogeneic blood transfusions:A metaanalysis[J].Interact Cardiovasc Thorac Surg,2008,8(3):373-376.
[18] Murphy GS,Szokol JW,Nitsun M,et al.The failure of retro⁃grade autologous priming of the cardiopulmonary bypass circuit to reduce blood use after cardiac surgical procedures[J].Anesth Analg,2004,98(5):1201-1207.
[19] Sutton SW,Duncan MA,Chase VA,et al.Leukocyte filtration and miniature perfusion during arrested heart cabg on a jehovah 's witness patient[J].Perfusion,2004,19(6):375-379.
[20] Brest van Kempen AB,Gasiorek JM,Bloemendaal K,et al.Low-prime perfusion circuit and autologous priming in cabg surgery on a jehova's witness:A case report[J].Perfusion,2002,17(1):69-72.
[21] Saxena P,Saxena N,Jain A,et al.Intraoperative autologous blood donation and retrograde autologous priming for cardiopul⁃monary bypass:A safe and effective technique for blood conser⁃vation[J].Ann Card Anaesth,2003,6(1):47-51.
[22] Srinivas K,Singh K.Combination of autologous transfusion and retrograde autologous priming decreases blood requirements [J].Ann Card Anaesth,2001,4(1):28-32.
[23] Zelinka ES,Ryan P,McDonald J,et al.Retrograde autologous prime with shortened bypass circuits decreases blood transfusion in high-risk coronary artery surgery patients[J].J Extra Cor⁃por Technol,2004,36(4):343-347.
[24] Kulat B,Zingle N.Optimizing circuit design using a remotemounted perfusion system[J].J Extra Corpor Technol,2009,41(1):28-31.
[25] Pappalardo F,Corno C,Franco A,et al.Reduction of hemodilu⁃tion in small adults undergoing open heart surgery:A prospective,randomized trial[J].Perfusion,2007,22(5):317-322.
[26] Durandy Y.The impact of vacuum-assisted venous drainage and miniaturized bypass circuits on blood transfusion in pediat⁃ric cardiac surgery[J].ASAIO J,2009,55(1):117-120.
[27] Dreizler T,Herbrechtsmeier T,Born F,et al.Effects of opti⁃mized bypass systems with retrograde autologous priming during extracorporeal circulation in high-risk patients[J].Kardio⁃technik,2010,19(1):6-10.
[28] Lisy M,Schmid E,Schmid R,et al.On-pump coronary artery bypass surgery without allogenic blood product transfusion[J].Thoracic and Cardiovascular Surgeon,2011,58,SUPPL.1.
[29] Lisy M,Schmid E,Nagy Z,et al.On-pump aortic valve re⁃placement without allogeneic blood product transfusion[J].Thoracic and Cardiovascular Surgeon,2011,59,SUPPL.1.
Effects of retrograde autologous priming on perioperative clinical results in a⁃dult:a meta-analysis
Sun Peng,Ji Bing-yang,Sun Yan-hua,Zhu Xian,Liu Jin-ping,Long Cun
Department of Cardiopulmonary Bypass,Cardiovascular Institute&Fuwai Heart Hospital,Beijing 100037,China
Ji Bing-yang,Email:dr.ji.cpb@gmail.com
ObjectiveTo undertake a meta-analysis of the effects of retrograde autologous priming(RAP)on perioperative results.MethodsA comprehensive search was conducted for randomized controlled trials(RCT)relevant to RAP using PubMed,Embase,Cochrane Library,Google Scholar,WangFang,WeiPu and CNKI literature databases.Clinical parameters and outcomes were focused on lowest hematocrit(Hct)during cardiopulmonary bypass(CPB),number of patients transfused blood intraoperatively,num⁃ber of patients transfused blood perioperatively,number of blood units transfused,24 houra chest tube drainage,hours to extubation,length of ICU stay and length of total hospital stay.ResultsTen studies were included.The lowest Hct during CPB(P<0.0001)and 24 hours chest tube drainage(P=0.0005)in RAP group had advantages over control group when the length of total hospital stay(P =0.28)was not apparently influenced.With significant heterogeneity(I2>50%),the effects of RAP could not be evaluated.The num⁃ber of patients transfused blood intraoperatively(P<0.00001),perioperatively(P<0.00001)and the number of blood units trans⁃fused(P<0.00001)were all significantly reduced in RAP group.No differences in the hours to extubation(P=0.37)and the length of ICU stay(P=0.18)were observed between the two groups.ConclusionRAP can reduce blood transfusion in adult significantly,but has no effect on patient's clinical outcomes comparing to conventional priming.
Retrograde autologous priming;Priming volume;Blood transfusion;Clinical results;Cardiopulmonary bypass
2013⁃09⁃10)
2013⁃10⁃23)
10.13498/j.cnki.chin.j.ecc.2014.01.10
100037北京,中国医学科学院 北京协和医学院阜外心血管病医院体外循环科
吉冰洋,E-mail:dr.ji.cpb@gmail.com