永久性I125植入近距离放射联合内分泌治疗中-高危前列腺癌
2016-09-09朱伊祎樊静朱再生刘江刘全启陈良佑
朱伊祎 樊静 朱再生 刘江 刘全启 陈良佑
永久性I125植入近距离放射联合内分泌治疗中-高危前列腺癌
朱伊祎 樊静 朱再生 刘江 刘全启 陈良佑
目的 分析永久性I125植入近距离放射治疗局限性前列腺癌的治疗效果。方法 回顾性分析61例永久性I125植入近距离放疗联合辅助内分泌治疗局限性中-高危前列腺癌患者临床及随访资料。生化复发定义为前列腺特异性抗原最低点加2.0ng/ml。结果 61例患者中,年龄59~87岁,平均 75.3岁。治疗前平均PSA19.6ng/ml。37例中危和24例高危。术后均行辅助内分泌治疗。平均随访39个月,5年总生存率,无生化复发率和肿瘤相关生存率分别为72.9%,73.1%,和92.2%。并发症:需手术治疗(经尿道前列腺切除术)4例(6.6%);心血管并发症2例(3.3%)。结论 永久性I125植入近距离放疗联合辅助内分泌治疗中-高危前列腺肿瘤疗效可靠,并发症低。
前列腺癌 近距离放射治疗 辅助内分泌治疗 外放疗
永久性I125植入近距离放射治疗(I125-PIB)局限性前列腺癌是目前公认的有效治疗方法,其疗效佳﹑并发症发生率低[1~4]。近年来,我国I125-PIB前列腺癌也发展迅速[1,5]。作者应用永久性I125近距离放疗联合辅助内分泌治疗中-高危前列腺癌患者61例,疗效满意,现报道如下。
1 临床资料
1.1一般资料 2008年6月和2015年6月浙江大学金华医院与浙江省中医院收治永久性I125植入近距离放疗联合辅助内分泌治疗局限性中-高危前列腺癌患者61例。年龄59~87岁,平均75.3岁。所有患者均行PSA﹑直肠指诊﹑X线胸片﹑经直肠B超﹑腹部B超﹑前列腺M RI平扫﹑全身骨扫描检查。治疗前平均PSA为19.6ng/ml。临床分期:根据TNM分期系统[6]为T2N0M0为45例,T3N0M016例。合并有严重冠心病(已置入冠状动脉支架>2个)伴高血压21例,严重COPD13例,严重糖尿病7例,慢性肾功能不全3例,多次腹腔手术2例,多种合并症﹑麻醉ASA评分为4分的极危险患者3例。全部患者经前列腺穿刺活检明确为前列腺癌。肿瘤Gleason评分:≤6﹑7﹑≥8分别为25﹑29﹑7例。危险因素分级:根据D'Amico的分组[6,7]:中危和高危分别为37﹑24例。治疗前患者知情并签署同意书。
1.2仪器设备 放射性粒子三维治疗计划系统:前列腺穿刺固定器﹑模板﹑推进器﹑18G粒子植入针和辅助设备为美国MickRadio-Nuclear公司产品。配有直肠探头的超声诊断仪为丹麦B-K公司产品。放射性I125粒子由中国原子能研究院生产,0.8mm×0.45mm,镍钛合金包壳,放射性活度为0.35~0.5mGi。
1.3手术方法 所有患者均采用超声引导技术治疗[8]。采用标准I125粒子植入技术。使用修改外围加载模式。连续硬膜外或全身麻醉下,截石位,先留置Foley尿管,经直肠B超以5mm层厚扫描前列腺基底至尖部横断面图像,传送至计算机治疗计划系统,按照外周配制技术,调整尿道和直肠周围放射剂量。将植入套管针经模板引导系统经会阴穿刺入前列腺,通过超声引导植入针送至前列腺准确部位,使用植入枪将粒子植入针尖部位,在植入枪后退过程中纵向释入粒子,一枚针位释放完毕后,重复植入其他针位粒子。I125治疗生物学剂量在140~160GY范围﹑一般是145GY。术后均进行辅助内分泌治疗。
1.4内分泌治疗(HT) 采用最大限度雄激素阻断(MAB):每个月注射LHRH激动剂(醋酸亮丙瑞林3.75mg,或醋酸戈舍瑞林3.6mg)和抗雄激素(比卡鲁胺80mg/d)用于MAB。辅助内分泌治疗6~8个月。
作者单位:310053 浙江省中医药大学第一临床医学院(朱伊祎)310006 浙江省中医院 超声诊疗科(樊静)321000 浙江大学金华医院 泌尿外科(朱再生 刘江刘全启 陈良佑)
1.5随访 生化复发定义[8,9]:为PSA最低值加2ng/ ml,即当PSA值超过最低PSA加上2ng/ml,被认为是生化复发。疾病进展定义为[9]:原发部位局部肿瘤的再次出现。多种影像学检查包括胸部X线片,CT扫描(胸部,腹部),骨显像和盆腔磁共振成像,分别用于生化复发转变为临床复发的诊断。从术后1个月开始,每月复查PSA,了解排尿情况及相关不良反应,每3个月B超检查。
1.6统计学方法 采用SPSS.16软件包。生存率﹑无生化复发率和肿瘤相关生存率用Kaplan-Meier法。
2 结果
61例患者植入粒子59~111粒,平均78粒。全部患者获得随访,随访时间12~82个月,平均39.7个月。3﹑5﹑7年总生存率分别为89.6%,72.9%,33.4%,无生化复发率分别为:89.2%﹑73.1%﹑67.9%;肿瘤相关生存率分别95.6%﹑92.2%﹑92.2%(见图1)。发生临床复发3例(4.92%),发生肺部转移1例;2例发生盆腔淋巴结及骨骼多发转移。并发症:术后近期尿路刺激征15例(24.6%),急性尿潴留9例(17.8%);多于术后6个月逐渐缓解。4例(6.6%)I125-PIB后7﹑13﹑22﹑26个月发生尿潴留,需要经尿道前列腺切除术(TURP)。直肠刺激征5例(8.2%)﹑血便3例(4.9%),均对症治疗6~12个月后逐渐缓解。心血管并发症2例(3.3%),分别于I125-PIB后29个月(并加MAB治疗8个月)和33个月(未行MAB治疗)发生急性心肌梗死,均行冠状动脉支架置入术治愈。
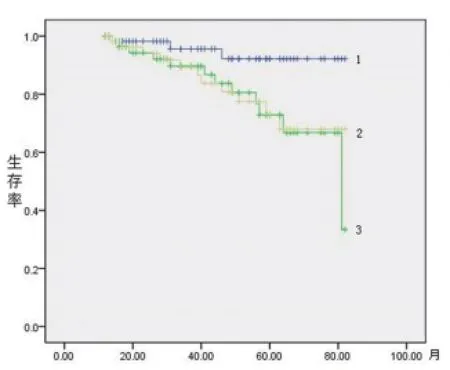
图1 生存率:1.肿瘤相关生存率,2.无生化复发率,3.总生存率
3 讨论
I125-PIB对局限性前列腺癌治疗,通过经直肠超声及计算机治疗计划系统,精确植入粒子,可实现三维适行内放疗,取得良好的效果,相比外放疗,其不良反应较低,患者易于接受[10~13]。Konaka等[14]相关研究:对于中-高危前列腺癌单独使用放疗对于肿瘤的治疗不充分,联合内分泌治疗能明显改善治疗效果。本组中-高风险患者是常规进行辅助HT治疗。本组总体5年总生存率,无生化复发率和肿瘤相关生存率分别为86.7%,76.7%和96.5%。相应的中危和高危患者无生化复发率为67.5%和65.2%。这些结果较文献报道[10~12]低。这可能与本组临床分期较高;术前未进行新辅助内分泌治疗等有关。作者认为:随着人口寿命延长﹑人口老龄化,患者多高龄或合并多种较严重的内科疾病,本组59%(36/61),为避免前列腺癌根治术带来的手术风险及术后的并发症,安全微创的近距离放疗在临床的应用将会越来越多。在我国,前列腺癌确诊时属于较高临床分期的患者较多,对于不愿手术或手术风险较大的中-高危前列腺癌患者,可选择近距离放疗联合辅助内分泌治疗。
文献报道I125-PIB术后泌尿生殖系统并发症较多[15]。本组患者术后近期尿路刺激征24.6%,急性尿潴留17.8%;6.6%排尿困难需行TURP手术。可见,近距离放疗术后患者以尿频等为主要不良反应,且多于术后6个月逐渐缓解。本组4例TURP患者年龄分别是71﹑73﹑79﹑76岁,前列腺长>5cm;术前3例有急性尿潴留需要留置导尿病史。其中71岁患者,于I125-PIB后7个月进行TURP手术,术后发生反复多次前列腺部出血和急迫性尿失禁,经多次内科保守治疗5个月,才逐渐好转。其余3例均>12个月再进行TUR-P手术,恢复较快。可见,对该类患者,I125-PIB术后易发生排尿困难并发症,应先进行TURP后再I125-PIB为佳;对I125-PIB术后须要TURP手术患者,建议I125-PIB术后>12个月再进行TURP手术。文献报道:直肠出血的发生率7%~20%[16]。本组直肠刺激征8.2%﹑血便4.9%,均对症治疗6~12个月后逐渐缓解。随访发现:多数I125-PIB术后的直肠出血是痔疮,与I125-PIB相关较少。可见,大多数的近距离放射治疗后直肠出血无需手术干预治疗。心血管并发症:有学者认为是与HT治疗相关,即使患者未合并心血管疾病和糖尿病,仍会增加心血管事件的风险[17]。本组中-高危患者,联合辅助HT占45%,但心血管并发症为3.31%,较西方报道[18]低。作者认为:心脑血管并发症与种族有关(黄种人缺血性心脏疾病病死率较白种人低已被证明[19]),与辅助HT关系不密切。可见,对于我国(黄种人)的中-高危前列腺癌,近距离放疗联合辅助HT可能是一个较合适的选择,不仅疗效明显,并发症较低,而且患者多能耐受,与根治术比较,能明显改善患者生活质量。
1张峰波,杜源,邵强,等.低剂量率近距离放射治疗局限性低/中危前列腺癌133例报告, 北京大学学报(医学版),2015,47(4):611~614.
2Stone NN, Stone MM, Rosenstein BS, et al. Influence of pretreatment and treatment factors on intermediate to long-term outcome after prostate brachytherapy. J. Urol,2011,185: 495~500.
3Sylvester JE, Grimm PD, Wong J, et al. Fifteen-year biochemical relapse-free survival, cause-specific survival, and overall survival following I125prostate brachytherapy in clinically localized prostate cancer: Seattle experience. Int. J. Radiat. Oncol. Biol. Phys,2011,81:376~381.
4 Taira AV, Merrick GS, Butler WM ,et al. Long-term outcome for clinically localized prostate cancer treated with permanent interstitial brachytherapy. Int. J. Radiat Oncol Biol Phys,2011,79: 1336~1342.
5罗勇, 韦能宝, 赵佳晖,等. 近距离放射治疗对前列腺癌患者生存预后的影响, 中华医学杂志.2013,93(42):3351~3354.
6那彦群,孙颖浩.前列腺癌诊断治疗指南.那彦群,叶章群,孙颖浩,等.2014版中国泌尿外科疾病诊断治疗指南.北京:人民卫生出版社,2014:61~89. 7 D'Amico AV, Desjardin A, Chung A, et al. Assessment of outcome prediction models for patients with localized prostate carcinoma managed with radical prostatectomy or external beam radiation therapy. Cancer,1998, 82: 1887~1896.
8Kittel JA, Reddy CA, Kristin L. Smith,et al. Long-Term Efficacy and Toxicity of Low-Dose-Rate 125 I Prostate Brachytherapy as Monotherapy in Low-, Intermediate-, and High-Risk Prostate Cancer . Int J Radiation Oncol Biol Phys, 2015, 92(4): 884~893.
9Reis LO, Sanches BCF, Zani EL,et al.PSA-nadir at 1 year as a sound contemporary prognostic factor for low-dose-rate iodine-125 seeds brachytherapy. World J Urol 2014, 32:753~759.
10Morris WJ, Keyes M, Spadinger I, et al. Population-based 10-year oncologic outcomes after low-dose-rate brachytherapy for low-risk and intermediate-risk prostate cancer. Cancer 2013,119:1537~1546.
11Zelefsky MJ, Chou JF, Pei X, et al. Predicting biochemical tumor control after brachytherapy for clinically localized prostate cancer: The Memorial Sloan-Kettering Cancer Center experience. Brachytherapy,2012,11:245~249.
12Stone NN, Stock RG. 15-year cause specific and all-cause survival following brachytherapy for prostate cancer: Negative impact of longterm hormonal therapy. J Urol, 2014,192:754~759.
13Dickinson PD, Malik J, Mandall P, et al: Five-year outcomes after iodine-125 seed brachytherapy for low-risk prostate cancer at three cancer centres in the UK. BJU Int,2014,113(5 ):748~753.
14Konaka H, Egawa S, Saito S,et al. Tri-modality therapy with i-125 brachytherapy, external beam radiation therapy, and short- or longterm hormone therapy for high-risk localized prostate cancer (trip):study protocol for a phase iii, multicenter, randomized, controlled trial. BMC Cancer , 2012(12):110.
15Mock S, Leapman M, Stock RG, et al. Risk of urinary incontinence following post-brachytherapy transurethral resection of the prostate and correlation with clinical and treatment parameters. J Urol ,2013,190:1805~1810.
16Mohammed N, Kestin L, Ghilezan M, et al. Comparison of acute and late toxicities for three modern high-dose radiation treatment techniques or localized prostate cancer. Int J Radiat Oncol Biol Phys ,2012,82:204~212.
17Keating NL, O'Malley AJ, Freedland SJ, et al. Does comorbidity influence the risk of myocardial infarction or diabetes during androgendeprivation therapy for prostate cancer? Eur. Uro,2013, 64: 159~166.
18Hunter GK, Reddy CA, Klein EA et al. Long-term (10-year)gastrointestinal and genitourinary toxicity after treatment with external beam radiotherapy, radical prostatectomy, or brachytherapy for prostate cancer. Prostate Cancer ,2012, 2012: 853487.
19Arai Y, Egawa S, Tobisu K et al. Radical retropubic prostatectomy:time trends, morbidity and mortality in Japan. BJU Int, 2000, 85:287~294.
Objectives To analyze the oncological outcomes of iodine-125 permanent implant brachytherapy in clinically localized prostate cancer. Methods Between 2008 and 2015,61 patients with clinically localized prostate cancer were treated with the iodine-125 permanent implant brachytherapy. Results Of the 61 patients,Age was average 75.3(rang 59 to 87)years old,The average PSA was 19.6 ng / mL. 37 cases were intermediate risk and 24 had high-risk disease. All patients were treated with adjuvant hormonal therapy. The biologically effective dose was 145 Gy. Median follow up was 39 months. Of these patients,At 5 years,overall survival,biochemical recurrence-free survival and cancer-specifi c survival were 72.9%,73.1% and 92.2%,respectively. Complications Required surgery (transurethral resection of the prostate)4(6.6%); cardiovascular complications in 2cases (3.3%).Conclusions The iodine-125 permanent implant brachytherapy with adjuvant endocrine results in excellent oncological outcomes and acceptable complications in the intermediate-risk and high-risk patients.
Prostate cancer brachytherapy Adjuvant hormonal therapy External beam Radiation therapy
