肺栓塞患者血栓定位与伴随疾病、危险因素、D二聚体、红细胞分布宽度的关系
2020-09-02郑卉
郑卉


【摘要】 目的 明確肺栓塞(PE)患者血栓定位与伴随疾病、危险因素、D二聚体、红细胞分布宽度(RDW)的关系。方法 148例已确诊的肺栓塞患者, 通过肺动脉CT血管造影技术(CTPA)评估血栓的存在和结构定位, 分析血栓定位与伴随疾病、危险因素、D二聚体、红细胞分布宽度的关系。
结果 148例患者中, 血栓定位于右肺主动脉的患者有56例(37.8%), 定位于左肺主动脉的患者有26例(17.6%), 定位于双侧肺主动脉的患者有66例(44.6%)。不同血栓定位患者的性别、恶性肿瘤、近期手术情况比较, 差异具有统计学意义 (P<0.05)。使用CTPA技术发现血栓定位于主肺动脉的患者有46例(31.1%), 血栓定位于肺叶、节段或亚段血管动脉的患者有102例(68.9%)。主肺动脉及肺叶、节段或亚段血管动脉栓塞患者的固定、近期手术、D二聚体、红细胞分布宽度情况比较, 差异具有统计学意义 (P<0.05)。主肺动脉栓塞红细胞分布宽度的ROC曲线下面积为0.72, 95%置信区间为(0.63, 0.81)。无主肺动脉栓塞红细胞分布宽度截断值为15.25%, 该截断值展示的敏感性为69.6%, 特异性为62.7%。
结论 血栓定位与手术固定、D二聚体水平、红细胞分布宽度具有显著相关性。
【关键词】 肺栓塞;肺动脉CT血管造影技术;D二聚体;红细胞分布宽度
DOI:10.14163/j.cnki.11-5547/r.2020.22.005
Correlation between thrombus location and concomitant diseases, risk factors, D-dimer, red blood cell distribution width in patients with pulmonary embolism ZHENG Hui. Department of Clinical Laboratory, Qingdao Fifthe Peoples Hospital, Qingdao 266000, China
【Abstract】 Objective To investigate the correlation between thrombus location and concomitant diseases, risk factors, D-dimer, red blood cell distribution width (RDW) in patients with pulmonary embolism (PE). Methods There were 148 patients diagnosed with pulmonary embolism, and the presence and anatomical localization of the thrombus were assessed via CT pulmonary angiography. The correlation between thrombus location and concomitant diseases, risk factors, D-dimer, red blood cell distribution width was analyzed. Results Of the 148 patients, thrombus of 56 patients (37.8%) were located in the right pulmonary aorta, 26 patients (17.6%) in the left pulmonary aorta, and 66 patients (44.6%) in the bilateral pulmonary aorta. There was statistically significant difference in gender, malignant tumor and recent surgery of patients with different thrombus locations (P<0.05). Using CTPA technique, 46 patients (31.1%) with thrombus localized to the main pulmonary artery, and 102 patients (68.9%) with thrombus to the pulmonary lobe, segment, or sub-segment vascular artery. There were statistically significant differences in fixation, recent surgery, D-dimer and red blood cell distribution width in patients with thrombus localized to main pulmonary artery and pulmonary lobe, segment or sub-segmental vascular artery (P< 0.05). The area under the ROC curve of the distribution width of red blood cells without thrombus localized to main pulmonary artery was 0.72, and the 95% confidence interval was (0.63, 0.81). The cut-off value of the distribution width of red blood cells without thrombus localized to main pulmonary artery was 15.25%. The cut-off value showed a sensitivity of 69.6% and a specificity of 62.7%. Conclusion The thrombus location was significantly correlated with surgical fixation, D-dimer level and red blood cell distribution width.
【Key words】 Pulmonary embolism; CT pulmonary angiography; D-dimer; Red blood cell distribution width
肺栓塞是由于血栓在血管中形成可部分或完全阻塞肺动脉循环的一种十分严重的心肺疾病[1-3]。肺栓塞的发生被认为是与各种危险因素具有密不可分的关系。对于怀疑肺栓塞的患者, 临床上、实验室和影像学结果都应该仔细研究。因为肺栓塞患者的临床诊断特异性差, 客观地诊断性检验结果被要求应用于肺栓塞的诊断[4]。CTPA越来越多的应用于怀疑肺栓塞的一线研究诊断工具。肺栓塞的程度通过受血栓影响最邻近血管的结构水平普遍展现出来[5]。对于一个明确诊断的疑似肺栓塞的患者, D二聚体是一个应该被评估和确定的指标。血清D二聚体的检测提供纤维蛋白溶解片段的信息。D二聚体分析特异性较低, 但对于大部分疑似血栓栓塞的患者具有较高的灵敏度和阴性预测值[6]。红细胞分布宽度是红细胞大小变异性的定量指标。这个参数早期从全血计数获得而来, 后来被公认为是无效红细胞生成的指标[7]。一些研究也建议红细胞分布宽度与心血管和肺疾病, 如肺栓塞有关[8-13]。该研究主要目的是评估肺栓塞患者血栓定位与危险因素、伴随疾病、D二聚体水平和红细胞分布宽度关系。
1 资料与方法
1. 1 一般资料 回顾性选取本院2017年7月~2018年6月就诊使用CTPA法确诊肺栓塞的患者148例。同时收集和检测患者的伴随疾病、危险因素、D二聚体水平、CTPA和红细胞分布宽度。纳入标准:近期手术、肺炎、感染、布鲁氏菌病、脑炎、偏瘫、手术后长时间(>72 h)固定患者。
1. 2 CTPA 使用16排多截面CT(Somatom Emotion 16-slice; CT2012E-Siemens AG, Berlin and Munchen, Germany)扫描患者胸廓, 患者静脉注射造影剂但不影响呼吸。
1. 3 D二聚体检测 血样样本移送到医院检验科。D二聚体含量使用全自动化学发光免疫分析检测, 试剂由深圳市新产业生物公司提供。
1. 4 红细胞分布宽度 使用全血检测确定。血液分析使用LH750 全血计数仪(Beckman Coulter, Fullerton, CA, USA)检测。
1. 5 统计学方法 采用SPSS18.0统计学软件进行统计分析。计量资料以均数±标准差( x-±s)表示, 采用t检验;计数资料以率(%)表示, 组间比较采用Mann-Whitney U检验, 非正态分布采用χ2检验;采用ROC曲线描述主肺动脉栓塞红细胞分布宽度的最佳截断值水平。P<0.05表示差异具有统计学意义。
2 结果
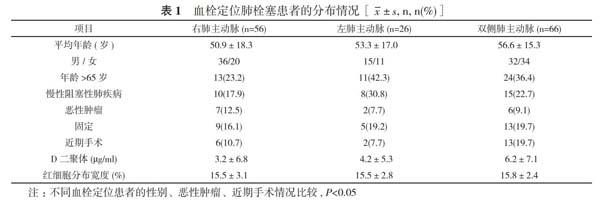
2. 1 血栓定位肺栓塞患者的分布情况 148例患者中, 男83例(56.1%), 女65例(43.9%);年龄18~81岁, 平均年龄(53.8±16.8)岁。固定(18.2%, 27/148)和近期手术(14.2%, 21/148)是最常见的危险因素。慢性阻塞性肺疾病(22.3%, 33/148)是最常见的伴随疾病。血栓定位于右肺主动脉的患者有56例(37.8%), 定位于左肺主动脉的患者有26例(17.6%), 定位于双侧肺主动脉的患者有66例(44.6%)。不同血栓定位患者的性别、恶性肿瘤、近期手术情况比较, 差异具有统计学意义 (P<0.05) ;平均年龄、年龄>65岁、慢性阻塞性肺疾病、固定、D二聚体、红细胞分布宽度情况比较, 差异无统计学意义(P>0.05)。见表1。
2. 2 CTPA确诊的主肺动脉和肺叶、节段或亚段血管动脉栓塞患者的分布情况 由于血栓影响最邻近血管的解剖学水平, 使用CTPA技术发现血栓定位于主肺动脉的患者有46例(31.1%), 血栓定位于肺叶、节段或亚段血管动脉的患者有102例(68.9%)。16例(34.8%)主肺动脉栓塞患者和32例(31.4%)肺葉、节段或亚段血管动脉栓塞患者的年龄>65岁。主肺动脉及肺叶、节段或亚段血管动脉栓塞患者的固定、近期手术、D二聚体、红细胞分布宽度情况比较, 差异具有统计学意义 (P<0.05) ;平均年龄、性别、年龄>65岁、慢性阻塞性肺疾病、恶性肿瘤情况比较, 差异无统计学意义(P>0.05)。见表2。
2. 3 主肺动脉栓塞红细胞分布宽度值的ROC曲线情况 主肺动脉栓塞红细胞分布宽度的ROC曲线下面积为0.72, 95%置信区间为(0.63, 0.81)。无主肺动脉栓塞红细胞分布宽度截断值为15.25%, 该截断值展示的敏感性为69.6%, 特异性为62.7%。见表3。
3 讨论
肺栓塞通常是由于系统血管形成血栓, 部分或者完全阻塞肺主动脉, 影响血液流动导致的。肺栓塞发生的范围较大, 从大量无症状血栓[14]到大量血栓导致的休克或心脏骤停均会出现[15]。
根据血栓解剖学定位的研究, 血栓定位在右肺、左肺和两侧均有, 分别占36%、18%和45%[16, 17]。关于血栓的数量, 65%的患者展示出多样性[3-6]血栓[17]。Simsek等[18]报道血栓定位于两侧主肺动脉占70.7%, 而单侧主肺动脉血栓占29.3%。男性单侧主肺动脉血栓定位于右肺占60.5%。根据作者的研究, 血栓定位于右主肺动脉占37.8%, 而双侧主肺动脉血栓占44.6%。
根据作者的研究, 关于血栓邻近定位, 血栓定位于主肺动脉患者有46例(31.1%), 肺叶、节段或亚段血管动脉的患者有102例(68.9%)。Gülcü等[19]检查31例患者, 通过CTPA确认血栓定位于主肺动脉占30.8%。Sen等[20]检测主肺动脉定位血栓占172例患者的30%。Perrier等[21]报道主肺动脉定位血栓占研究患者的32%。
根據国际合作肺栓塞登记表[22], 肺栓塞相关预后因素包括年龄70岁以上、恶性肿瘤、充血性心力衰竭和慢性呼吸功能不全。根据作者的研究, 最经常遇到的伴随疾病是慢性阻塞性肺疾病(22.2%)和恶性肿瘤(10.1%)。
肺栓塞被发现与促使患者形成血栓的老年性疾病, 如充血性心力衰竭、髋部骨折、休克、增加凝血潜在因素和限制性血液流动息息相关[23, 24]。根据作者的研究, 48患者(32.4%)年龄>65岁, 但年龄和血栓定位无必然联系。主肺动脉血栓患者年龄均值相对较高, 但差异无统计学意义(P>0.05)。在危险因素中, 长时间固定和近期手术的患者可显著增加肺栓塞风险。关于肺栓塞危险因素, Gülcü等[19]报道固定(41.9%)和近期手术(32.3%)。根据作者的研究, 作者的鉴定危险因素中固定占18.2%, 而近期手术占14.2%。血栓通常定位于稳定性患者的肺主动脉, 通常发现在具有近期手术史的右侧肺部。据报道D二聚体水平与血栓定位存在相关性, D二聚体水平在部分和大血栓与亚段血管血栓存在差异[25]。另有研究报道邻近定位血栓患者血清D二聚体水平比远端定位血栓更高, 但差异无统计学意义(P>0.05)[26]。Ghanima等[27]报道血清D二聚体水平和最近段血栓定位存在一定联系。根据作者的研究, 发现血栓定位和D二聚体水平具有明显关联。另外, 作者认为主肺动脉定位血栓D二聚体均值明显高于其他动脉分支血栓的患者。
大量研究认为红细胞分布宽度可能与心血管疾病[8-11]和肺部疾病[12, 13]存在联系。两个研究已经证实红细胞分布宽度与肺栓塞有联系。研究发现升高的红细胞分布宽度是一个独立的早期肺栓塞相关死亡率的预测指标[13, 28]。最近, 在两个病例对照研究中发现静脉血栓与红细胞分布宽度存在一定联系[29, 30]。在作者的研究中, 发现红细胞分布宽度在肺栓塞患者中显著升高, 而且红细胞分布宽度和血栓定位存在明显关联。主肺动脉定位血栓患者红细胞分布宽度均值显著升高。作者的结果认为红细胞分布宽度在主肺动脉定位血栓和其他动脉分支血栓存在差异。
作者的研究存在一定局限。这是一个回顾性研究, 选取的患者是通过医院计算机系统筛选的住院肺栓塞患者。对于某些患者数据存在不足, 那是由于研究患者数量存在限制的原因。另外限制的因素是CTPA阳性肺栓塞患者的选取, 排除其他途径而非CTPA方法确诊的肺栓塞患者。
最后, 作者发现主肺动脉血栓栓塞的患者占肺栓塞患者的31.1%。另外, 作者认为近端血栓定位与D二聚体水平和红细胞分布宽度存在显著的关联。
参考文献
[1] Alikhan R, Peters F, Wilmott R, et al. Fatal pulmonary embolism in hospitalised patients: a necropsy review. J Clin Pathol, 2004, 57(12):1254-1257.
[2] Heit JA, OFallon WM, Petterson TM, et al. Relative impact of risk factors for deep vein thrombosisand pulmonary embolism a population-based study. Arch Intern Med, 2002, 162(11):1245-1248.
[3] Torbicki A, Perrier A, Konstantinides S, et al. Guidelines on the diagnosis and management of acute pulmonary embolism the Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). Eur Heart J, 2008, 29(18): 2276-2315.
[4] Nielsen HK. Pathophysiology of venous thromboembolism. Semin Thromb Hemost, 1991(17 Suppl 3):250-253.
[5] Ghanima W, Abdelnoor M. The association between the proximal extension of the clot and the severity of pulmonary embolism (PE): A proposal for a new radiological score for PE. J Int Med, 2007, 261(1):74-81.
[6] Ginsberg JS, Wells PS, Kearon C, et al. Sensitivity and specificity of a rapid whole blood assay for D-dimer in the diagnosis of pulmonary embolism. Ann Intern Med, 1998, 129(12):1006-1011.
[7] Karnad A, Poskitt TR. The automated complete blood cell count. Use of the red blood cell volume distribution width and mean platelet volume in evaluating anemia and thrombocytopenia. Arch Intern Med, 1985, 145(7):1270-1272.
[8] Felker GM, Allen LA, Pocock SJ, et al. Red cell distribution width as a novel prognostic marker in heart failure: data from the CHARM Program and the Duke Databank. J Am Coll Cardiol, 2007, 50(1):40-47.
[9] Tonelli M, Sacks F, Arnold M, et al. Relation between red blood cell distribution width and cardiovascular event rate in people with coronary disease. Circulation, 2008, 117(2):163-168.
[10] Fukuta H, Ohte N, Mukai S, et al. Elevated plasma levels of B-type natriuretic peptide but not C-reactive protein are associated with higher red cell distribution width in patients with coronary artery disease. Int Heart J, 2009, 50(3): 301-312.
[11] Dabbah S, Hammerman H, Markiewicz W, et al. Relation between red cell distribution width and clinical outcomes after acute myocardial infarction. Am J Cardiol, 2010, 105(3):312-317.
[12] Hampole CV, Mehrotra AK, Thenappan T, et al. Usefulness of red cell distribution width as a prognostic marker in pulmonary hypertension. Am J Cardiol, 2009, 104(6):868-872.
[13] Zorlu A, Bektasoglu G, Guven FM, et al. Usefulness of admission red cell distribution width as a predictor of early mortality in patients with acute pulmonary embolism. Am J Cardiol, 2012, 109(1):128-134.
[14] Arseven O, Sevinc C, Alatas F, et al. The report for the diagnosis and therapeutical consensus of pulmonary thromboembolism. Tur Toraks Der, 2009, 10(11):7-47.
[15] Tapson VF, Witty LA. Massive pulmonary embolism. Clin Chest Med, 1995, 16(2):329-340.
[16] Dahnert W. Pulmonary thromboembolism disease//Dahnert WF. Radiology Review Manual. Philadelphia: Lippincott Williams & Wilkins, 1999:431-432.
[17] Oser RF, Zuckerman DA, Gutierrez FR, et al. Anatomic distribution of pulmonary trombus at pulmonary angiography: Implications for crosssectional imaging. Radiology, 1996, 199(1):31-35.
[18] Simsek A, Turkkan O, Melek K, et al. Assessment of Patients with Pulmonary Thromboembolism (PTE) Diagnosed in Our Clinic: 5 Years Experience. Turkish Thoracic Journal/turk Toraks Dergisi, 2010, 11(4):149-154.
[19] Gülcü A, Akko?lu A, Yilmaz E, et al. Comparison of clinical assessments with computerized tomography pulmonary angiography results in the diagnosis of pulmonary embolism. Tüberküloz Ve Toraks, 2007, 55(2):174-181.
[20] Sen E, Arslan F, Yurt SE, et al. Clinical and radiological findings in patients diagnosed pulmonary thromboembolism by pulmonary computerized tomography angiography. Tüberküloz Ve Toraks, 2009, 57(1):5-13.
[21] Perrier A, Roy PM, Sanchez O, et al. Multidetector-row computed tomography in suspected pulmonary embolism. N Engl J Med, 2005, 352(17):1760-1768.
[22] Goldhaber SZ, Visani L, De Rosa M. Acute pulmonary embolism clinical outcomes in the International Cooperative Pulmonary embolism Registry (ICOPER). Lancet, 1999, 353(9162):1386-1389.
[23] Timmons S, Kingston M, Hussain M, et al. Pulmonary embolism differences in presentation between older and younger patients. Age Ageing, 2003, 32(6):601-605.
[24] Gal GL, Righini M, Roy PM, et al. Differential value of risk factors and clinical signs for diagnosing pulmonary embolism according to age. Journal of Thrombosis & Haemostasis, 2010, 3(11):2457-2464.
[25] Monye WD, Sanson BJ, Gillavry MRM, et al. Embolus location affects the sensitivity of a rapid quantitative D-dimer assay in the diagnosis of pulmonary embolism. Am J Respir Crit Care Med, 2002, 165(3):345-348.
[26] Sen N, Ermis H, Altinkaya N, et al. Pulmonary Embolism in Young and Elderly Patients: Clinical Characteristics, Laboratory and Instrumental Findings and Differences Between Age Groups. Turk Toraks Dergisi, 2010, 11(4):160-166.
[27] Ghanima W, Abdelnoor M, Holmen LO, et al. D-dimer level is associated with the extent ofpulmonary embolism. Thromb Res, 2007, 120(2):281-288.
[28] Ozsu S, Abul Y, Gunaydin S, et al. Prognostic Value of Red Cell Distribution Width in Patients With Pulmonary embolism. Clin Appl Thromb Hemost, 2014, 20(4):365-370.
[29] Cay N, Unal O, Kartal MG, et al. Increased level of red blood cell distribution width is associated with deep venous thrombosis. Blood Coagul Fibrinolysis, 2013, 24(7):727-731.
[30] Rezende SM, Lijfering WM, Rosendaal FR, et al. Hematological variables and venous thrombosis: red cell distribution width and blood monocytes are associated with an increased risk. Haematologica, 2014, 99(1):194-200.
[收稿日期:2020-02-12]
作者單位: 266000 青岛市第五人民医院检验科
通讯作者:尹飞