Castleman disease in the hepatic-gastric space: A case report
2019-04-25XiaoYunXuXueQingLiuHongWeiDuJianHuaLiu
Xiao-Yun Xu, Xue-Qing Liu, Hong-Wei Du, Jian-Hua Liu
Xiao-Yun Xu, Hong-Wei Du, Department of Gastroenterology, Second Hospital of Hebei Medical University, Shijiazhuang 050000, Hebei Province, China
Xue-Qing Liu, Jian-Hua Liu, Department of Hepatobiliary Surgery, Second Hospital of Hebei Medical University, Shijiazhuang 050000, Hebei Province, China
Corresponding author: Jian-Hua Liu, PhD, Professor, Department of Hepatobiliary Surgery,Second Hospital of Hebei Medical University, 215 West Heping Road, Shijiazhuang 050000,Hebei Province, China. dr.ljh@outlook.com
Abstract
Key words: Castleman disease; Hepatic-gastric space; Endoscopic ultrasound; Endoscopic ultrasound guided fine needle aspiration; Rapid on-site evaluation; Case report
INTRODUCTION
Castleman disease (CD), also known as giant lymph node hyperplasia, was first reported by Castleman et al[1]in 1956. It is a rare benign proliferative pathological change of the lymph nodes, which maintains the basic morphology of lymph nodes with envelope formation and clear borders with adjacent structures[2]. The cause is unknown and may be related to a chronic inflammatory reaction, medications,autoimmune abnormalities or other factors[3]. CD can occur in any part of the body containing lymph nodes and is most common in the chest (accounting for about 70%),followed by the neck (14%), abdomen (12%) and axillae (4%)[4-6].
The main pathological change observed in CD is the hyperplasia of small blood vessel-like tissue and lymphoid tissue. It is pathologically classified into the hyaline vascular type, plasma cell type and mixed hyaline vascular and plasma cell type. The hyaline vascular type is the most common, accounting for about 80% to 90% with the pathological manifestation being intrafollicular or interfollicular lymphoid tissue hyperplasia. The follicular center contains many hyalinized capillaries, and the lymphoid tissue contains eosinophils and immunoblasts. The lesions are mostly focal and usually do not manifest any clinical symptoms. The main treatment adopted is surgery. The incidence of plasma cell type is relatively low, accounting for about 10%.Pathologically, it mostly presents as large follicles and interfollicular plasma cell infiltration, vascular proliferation being uncommon and a common diffuse distribution with about 50% of the cases exhibiting clinical symptoms, including superficial lymph node enlargement, anemia, weight loss and hepatosplenomegaly. It has a malignant tendency and requires comprehensive treatment. The mixed type has the characteristics of both the hyaline vascular type and plasma cell type[7,8].
CASE PRESENTATION
Chief complaints
The patient, a 33-year-old woman, had epigastric distension for half a year.
例 假设有u1、u2两名用户对i1~i3三部电影做出评分的矩阵R和R′,其中R包含了u1对i1、u2对i2的评分,R′除了这两个评分外,还包含了u1对i3的评分,则R和R′是相邻的.
Imaging examination
Examinations were performed in a local hospital. Gastroscopy revealed erythema exudative gastritis, and computed tomography (CT) scan showed round soft tissue nodules, about 5.45 cm in diameter, in the hepatic-gastric space (Figure 1). The patient was referred to our hospital for an enhanced CT examination. The CT values for the plain scan, arterial phase and venous phase were 42.9 HU, 109.6 HU and 82.4 HU,respectively (Figure 2). The disease was suspected to be CD according to enhanced CT scan findings. Endoscopic ultrasound (EUS) was performed on the patient using a linear array EUS EG530UT with the host Fujin Su-8000. The EUS findings demonstrated low echoes in the hepatic-gastric space, and scattered star-like hyperechoes were observed inside. The color Doppler indicated that there was no blood flow signal. In order to clarify the nature of the lesion, EUS guided fine needle aspiration (EUS-FNA), (puncture needle COOK-ECHO 19G) was used (Figure 3).
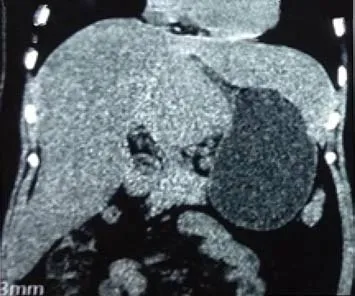
Figure 1 Computed tomography image showing circular soft tissue nodule in the hepatic-gastric space.
FINAL DIAGNOSIS AND TREATMENT
The puncture smear was subjected to Diff-Quik staining. Rapid on-site evaluation(ROSE) was performed, which showed a large number of scattered lymphocytes with normal morphology under a background of red blood cells (Figure 4). Hematoxylin eosin staining of the puncture smear showed scattered lymphocytes with normal morphology. Histopathology showed a large number of lymphocytes with normal morphology with B cells predominating. Immunohistochemistry results were as follows: CD117 (-), CD20 (+), CD3 (scattered +), CD30 (-), CD68 (scattered +), desmin(+), Ki-67 (+ < 30%), S-100 (-), SMA (+) and vimentin (+) (Figure 5). The possibility of CD was high.
After sufficient preoperative evaluation, resection of the hepatic-gastric space mass and proximal stomach was performed. Surgical resection pathology revealed a 9 cm ×5 cm × 4.5 cm mass outside the serosa of the gastric wall, and the cut surface was gray and crisp (Figure 6). Based on immunohistochemistry, in situ hybridization and genetic testing, postoperative diagnosis was atypical hyperplasia of lymphoid tissue,consistent with CD (hyaline vascular type, Figure 7).
OUTCOME AND FOLLOW-UP
The general condition of the patient was acceptable after surgery. A review CT scan will be performed once a year.
DISCUSSION
Abdominal CD is a rare pathological change that is often misdiagnosed as other tumors before surgery. Enhanced CT scan usually shows a solid mass with clear boundaries and uniform density. Progressive enhancement and continuous enhancement in enhanced CT scans have certain guiding significance for CD diagnosis[9]. In magnetic resonance imaging scans, signals on T1W1 are mostly uniform and low, and signals on T2W1 are relatively variable with equal, slightly higher or higher signal, indicating that magnetic resonance imaging scans can show fiber and collagen components in the center of the lesion better than CT scans[10].Although enhanced CT and magnetic resonance imaging scans have some characteristic manifestations, they still lack specificity. A gold standard for the pathological diagnosis is still required. EUS-FNA can extract internal tissues of the tumor for histological and cytological examinations and provide accurate diagnosis as much as possible before surgery, thereby playing a crucial role in the development of tumor treatment schemes[11-16].
Localized mass type CD should be distinguished from the following diseases in terms of pathology. First, lymphoma should be excluded. Abdominal localized tumors are mostly non-Hodgkin lymphoma in which the lymph node structure is almost completely destroyed and dysplasia of lymphocytes can be observed. The diagnosis should be confirmed using immunohistochemistry, in situ hybridization and genetic testing. Second, gastrointestinal stromal tumor should be excluded.Immunohistochemistry will show positive results for CD34, CD117 and DOG1. Third,schwannomas should be excluded. Immunohistochemistry will show 100% positive rate for S-100, which is diffuse strong positive. Fourth, ectopic pheochromocytoma should be excluded. Immunohistochemistry will show positive results for chromogranin, neuronspecific enolase and synaptophysin. Finally, intra-abdominal invasive fibromatosis should be excluded. Immunohistochemistry will show a positive result for β-catenin.
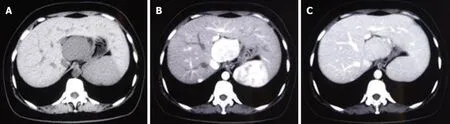
Figure 2 Enhanced computed tomography images of the patient. A: Plain scan; B: Arterial phase; C: Venous phase.
In this case, Diff-Quik staining was used for ROSE. Zhao et al[17]believed that generally samples should be obtained using 22G-27G needles for cell morphology analysis. In this case, the lesion was located in the hepatic-gastric space. The EUS was placed on the side of lesser gastric curvature, inferior to the cardia, to scan the lesion and guide the puncture. The EUS was not bent, the needle passage was straight and the lesion had no obvious blood flow signal. In order to obtain more tissue and reduce the number of punctures, COOK-ECHO 19G was used for puncturing. Regarding the value of ROSE for specimens obtained by EUS-FNA, scholars had different opinions in recent years. Koul et al[18]believed that EUS-FNA with ROSE significantly improves the sufficiency of the sample and is associated with high diagnostic accuracy. In FNA guided by EUS for pancreatic masses, the use of ROSE can improve the diagnostic rate.
CONCLUSION
In this case, according to the Diff-Quik staining and hematoxylin eosin staining results of preoperative EUS-FNA puncture smears as well as the immunohistochemistry results, CD was highly suspected. A sufficient preoperative evaluation was made and a precise surgical plan was developed. Postoperative pathology confirmed CD.
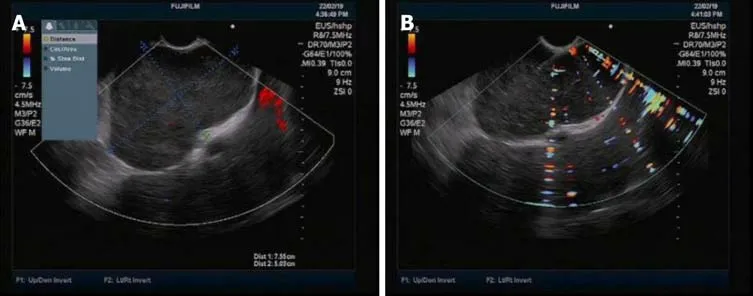
Figure 3 Endoscopic ultrasound images of the patient. A: Endoscopic ultrasound revealed low echoes in the hepatic-gastric space with scattered star-shaped high echoes. Color Doppler revealed absence of blood flow signal; B: Endoscopic ultrasound guided fine needle aspiration.

Figure 4 Diff-Quik staining showed a large number of scattered lymphocytes with normal morphology under the background of red blood cells.
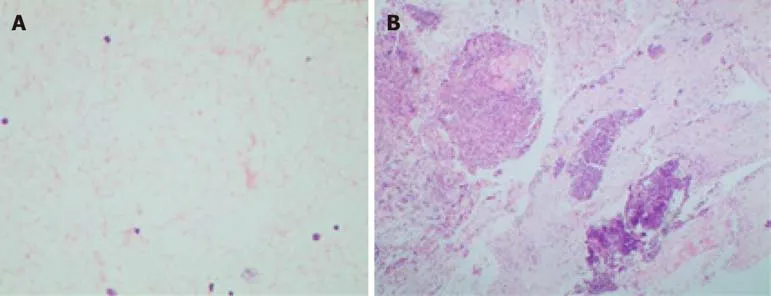
Figure 5 Hematoxylin eosin staining of the smear and tissue. A: Hematoxylin eosin staining of the smear: Scattered lymphocytes with normal morphology; B:Hematoxylin eosin staining of the tissue: A large number of lymphocytes with normal morphology, dominated by B cells.

Figure 6 Surgical specimens.
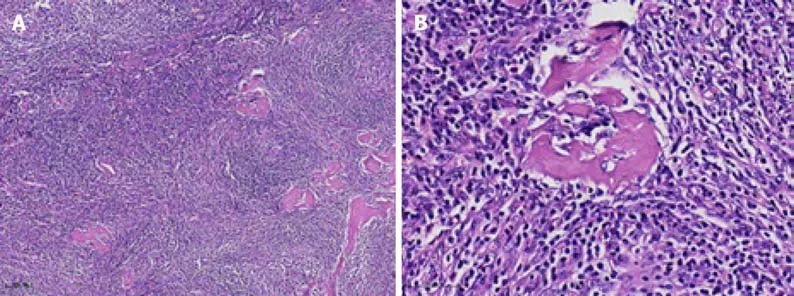
Figure 7 Postoperative pathological hematoxylin eosin staining. A: × 100; B: × 400.
猜你喜欢
杂志排行

World Journal of Clinical Cases的其它文章
- Polyunsaturated fatty acids and DNA methylation in colorectal cancer
- lmpact of resection margins on long-term survival after pancreaticoduodenectomy for pancreatic head carcinoma
- Arthroscopy combined with unicondylar knee arthroplasty for treatment of isolated unicompartmental knee arthritis: A long-term comparison
- lntact, pie-crusting and repairing the posterior cruciate ligament in posterior cruciate ligament-retaining total knee arthroplasty: A 5-year follow-up
- Community-acquired pneumonia complicated by rhabdomyolysis: A clinical analysis of 11 cases
- Dissection and ligation of the lateral circumflex femoral artery is not necessary when using the direct anterior approach for total hip arthroplasty