基于CT图像纹理分析评价结直肠癌肝转移新辅助治疗后疗效的价值
2017-05-15胡飞翔胡婷丹彭卫军
胡飞翔,胡婷丹,童 彤,彭卫军
复旦大学附属肿瘤医院放射诊断科,复旦大学上海医学院肿瘤学系,上海 200032
基于CT图像纹理分析评价结直肠癌肝转移新辅助治疗后疗效的价值
胡飞翔,胡婷丹,童 彤,彭卫军
复旦大学附属肿瘤医院放射诊断科,复旦大学上海医学院肿瘤学系,上海 200032

彭卫军,教授,复旦大学博士研究生导师,现任复旦大学附属肿瘤医院放射诊断科主任,中国抗癌协会肿瘤影像专业委员会候任主任委员,上海医学会放射诊断专科委员会副主任委员,上海市抗癌协会肿瘤影像专业委员会主任委员,中华医学会放射学分会乳腺学组副组长。
目的:探讨治疗前基线CT门静脉期图像的直方图分析预测结直肠癌肝转移(colorectal liver metastasis,CRLM) 新辅助治疗后疗效的价值。方法:选取34例CRLM患者,共计132枚病灶,经FOLFOX(氟尿嘧啶+亚叶酸钙+奥沙利铂)、FOLFIRI (氟尿嘧啶+亚叶酸钙+伊立替康)或CapeOX(奥沙利铂+卡培他滨或卡培他滨单用)方案化疗。所有患者均接受至少两次常规腹部平扫加增强三期CT扫描,于化疗前4周内行CT基线扫描,化疗开始后2~3个月内行第2次扫描以评估疗效。对患者门静脉期CT图像进行直方图分析,依据实体肿瘤疗效评价标准(Response Evaluation Criteria in Solid Tumors,RECIST)(Version 1.1)进行疗效评估,获得相应转移瘤的纹理参数,比较缓解与非缓解组患者治疗前基线CT直方图参数的差异。采用受试者工作特征(receiver operating characteristic,ROC)曲线分析法计算各参数预测缓解的曲线下面积(area under curve,AUC)、灵敏度、特异度、阳性预计值、阴性预计值、准确率及截断值。由两名放射科医师达成一致意见后勾画感兴趣区。结果:34例患者中,缓解组21例,非缓解组13例。缓解组的均值、方差、偏度和百分位数(10%、50%、90%、99%)低于非缓解组,差异有统计学意义(P<0.05);但峰度值和1%百分位数无显著差异(P=0.769、0.06)。90th百分位数在截断值为167时具有较高的准确率(81.82%),此时灵敏度、特异度、阳性预计值、阴性预计值及AUC分别为74.42%、95.65%、96.65%、66.97%和0.854。结论:CT门静脉期直方图分析对预测CRLM患者新辅助疗效具有潜在价值。
纹理分析;直方图;结直肠癌肝转移
目前,结直肠癌(colorectal cancer,CRC)是男性第三高发、女性第二高发的肿瘤[1],且15%~25%的患者在诊断为CRC时已发生肝转移。然而,CRC原发病灶根治性切除手术后仍有15%~25%的患者发生肝转移,其中约85%无法做到根治性切除[2-6],因此CRC肝转移(colorectal liver metastasis,CRLM)也成为CRC患者的最主要死亡原因(60%~71%)[7]。对于无法进行根治性手术切除的CRC患者,往往采用姑息性化疗。对于CRC确诊后合并同期肝转移患者,若原发病灶无出血、无梗阻症状或无穿孔,除外在技术上容易切除的肝转移灶且不存在不良预后的患者,均建议采用新辅助治疗[8-11]。全身化疗方案包括:FOLFOX (氟尿嘧啶+亚叶酸钙+奥沙利铂)、FOLFIRI (氟尿嘧啶+亚叶酸钙+伊立替康)、CapeOX (奥沙利铂+卡培他滨或卡培他滨单用)或FOLFOXIRI (氟尿嘧啶+亚叶酸钙+奥沙利铂+伊立替康)[12-15]。但一线化疗后,仍有约50%的CRC患者表现为无缓解甚至疾病进展[16]。对于这部分患者,临床医师可尝试使用贝伐单抗或西妥昔单抗等靶向治疗药物。为减少化疗对肝脏手术的不利影响,新辅助化疗原则上不超过6个周期[17],一般建议2~3个月内完成并进行手术[18]。
CRLM新辅助化疗后的疗效预测对指导临床制订后续治疗方案至关重要。CT可在形态学上对CRLM进行疗效评价[19]。图像纹理分析是近年来新出现的图像后处理技术,通过量化分析影像图像像素灰度值的局部特征、变化规律及分布模式等纹理特征来反映感兴趣区(region of interest, ROI)内生物组织结构的不均质性[20-21]。在过去有关肝脏辅助诊断的纹理分析研究中,多采用平扫图像[22]。近期CT增强图像纹理分析的应用逐渐广泛,增强扫描可提供病灶的血供情况及病灶内部血流变化特征[23]。影像图像纹理分析可提供更多肉眼无法观察到的图像信息[24]。灰度直方图分析是纹理分析中的一部分,可帮助量化肿瘤内部的异质性,在肿瘤诊断及疗效评价中较常规形态学评估具有更多优势[25-27]。
目前,关于CT增强扫描图像的灰度直方图分析预测CRLM新辅助化疗后疗效的研究鲜有报道。本研究采用门静脉期CT增强图像的灰度直方图分析来判断CRLM患者的近期疗效,以期为临床评估新辅助治疗后疗效并制订后续治疗方案提供有效辅助手段。
1 资料和方法
1.1 患者资料
收集复旦大学附属肿瘤医院2011年6月—2016年8月期间初诊为CRLM的患者共34例,其中>1 cm的可测量病灶132枚。所有患者均接受CT平扫加三期增强检查,并于基线检查结束后进行全身化疗。其中男性20例、女性14例;平均年龄(58.85±9.96)岁。患者的入选标准为:① 基线CT检查时间在新辅助治疗开始前4周内完成;② 患者在基线检查前未接受任何CRC及肝脏病灶相关治疗,包括手术、化疗及放疗等;③无结直肠外其他肿瘤相关病史;④ 第2次评估在新辅助治疗后2~3个月内完成。
1.2 检查方法
CT检查采用SIEMENS公司Somatom Sensation型螺旋CT扫描仪,层厚8 mm,层距8 mm。患者检查前常规禁食8~12 h,取平卧位,平扫后行增强扫描。使用碘海醇(300 gI/L)作为造影剂,按1.5 mL/kg体重计算给药量。用高压注射器经肘静脉注射给药,注射速率为2.5 mL/s。于造影剂注射后30 s、60 s及2~15 min分别行屏气动脉期、门静脉期及延迟扫描,扫描范围包括所有病变区域。
1.3 图像分析与评价标准
采用MaZda软件(Version 4.6,Instytut Elektroniki)进行纹理分析[28]。图像通过影像归档和通信系统(Picture Archiving and Communication Systems,PACS)下载并导入软件中进行分析。对所有患者门静脉期CT图像进行ROI勾画,由两名放射科医师达成一致意见后选取(两名医师分别具有3年和13年以上工作经验),均不知道患者预后情况。ROI选择于门静脉期肝转移瘤的最大层面进行,以>1 cm病灶为目标,沿病灶边缘轮廓勾画ROI,勾画过程中尽可能避开大血管(包括门静脉及肝静脉等),生成ROI内的各个灰度直方图参数值:均值(mean),方差(variance),偏度(skewness),峰度(kurtosis)及第1、20、50、90、99百分位数(1st、10th,50th,90th,99th percentile)。采用实体肿瘤疗效评价标准(Response Evaluation Criteria in Solid Tumors,RECIST)(Version 1.1)进行疗效评估[29],将完全缓解(complete response,CR)与部分缓解(partial response,PR)患者划归于缓解组,将疾病发展(progressive disease,PD)与疾病稳定(stable disease,SD)患者划归于非缓解组。然后对各纹理参数与疗效情况进行统计学分析。
1.4 统计学处理
使用SPSS 21.0和MedCalc 12.7.2进行统计学分析。患者一般特征连续性变量符合正态分布者采用t检验,用表示;不符合正态分布者采用Mann-Whitney U检验,用中位值表示。对具有统计学意义的直方图参数,进行受试者工作特征(receiver operating characteristic,ROC)曲线分析并计算相应的曲线下面积(area under curve, AUC)。截断值采用最大约登指数计算:约登指数=灵敏度-(1-特异度)。
2 结 果
2.1 患者一般特征
根据RECIST标准,经新辅助治疗后2~3个月,将患者分为治疗后缓解组(A组,21例)和非缓解组(B组,13例)。患者接受全身化疗方案包括:FOLFOX(10例)、FOLFIRI(14例)、CapeOX (10例)。详见表1。
2.2 灰度直方图各参数的诊断效能
结果显示,CRLM患者经新辅助治疗后2~3个月的疗效评估可通过基线CT门静脉期图像灰度直方图分析中的均值、方差、偏度及百分位数(10%、50%、90%、99%)进行有效预测。缓解组(图1)中上述纹理参数显著低于非缓解组(图2) (P<0.05),但峰度值和1%百分位数在两组之间无显著差异(P=0.769、0.06)(表2)。采用ROC曲线分析CT门静脉期直方图各参数评价缓解组的诊断效能(图3)。当90th百分位数≤167时,可获得较高的准确率(81.82%),此时灵敏度、特异度、阳性预计值(positive predictive value,PPV)、阴性预计值(negative predictive value,NPV)及AUC分别为74.42%、95.65%、96.97%、66.67%和0.854 (表3)。
3 讨 论
目前,肝转移患者主要采用一线化疗方案,但随访中发现约85%患者出现疾病进展[30],且只有不到50%的患者对一线化疗敏感[31]。对于一线化疗方案疗效不理想者,可使用其他治疗方案,包括加用分子靶向治疗或联用肝动脉灌注化疗[32]。能否尽早预测新辅助化疗疗效对临床制订后续方案至关重要,已有研究评估了纹理分析评价疗效的潜力。Ganeshan等[33]和Miles等[34]在研究CRC患者肝脏纹理情况时发现,肝脏的粗糙纹理与隐匿性恶性肿瘤和不良预后有关。本研究发现,低的均值、方差、偏度和百分位数(10%、50%、90%、99%)鉴别缓解与非缓解组具有统计学意义(P<0.05),而峰度值和1%百分位数鉴别缓解与非缓解组无显著差异(P=0.769、0.06)。

图1 新辅助化疗后缓解组灰度直方图及各参数
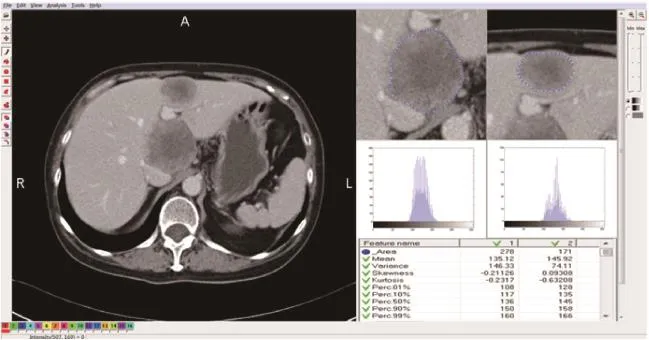
图2 新辅助化疗后非缓解组灰度直方图及各参数
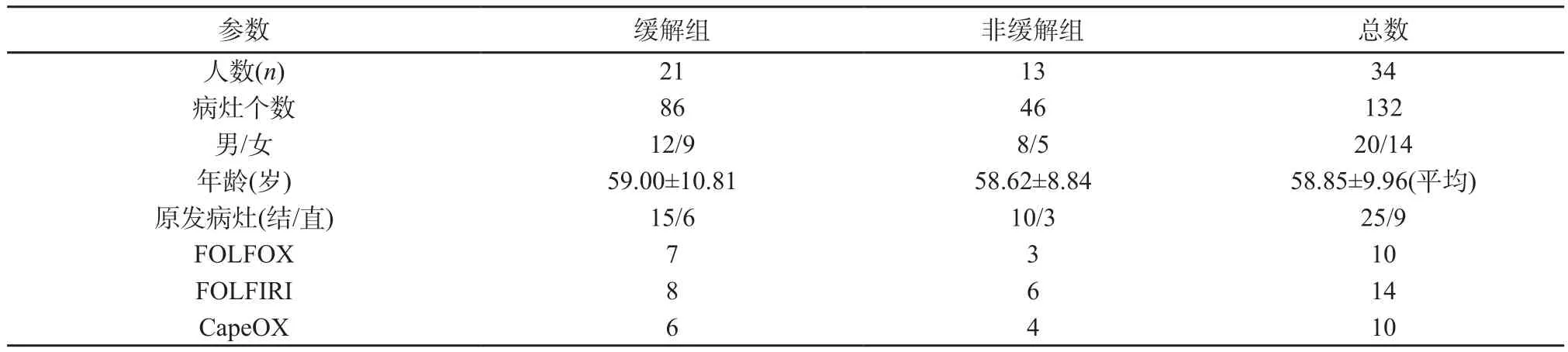
表1 患者一般特征
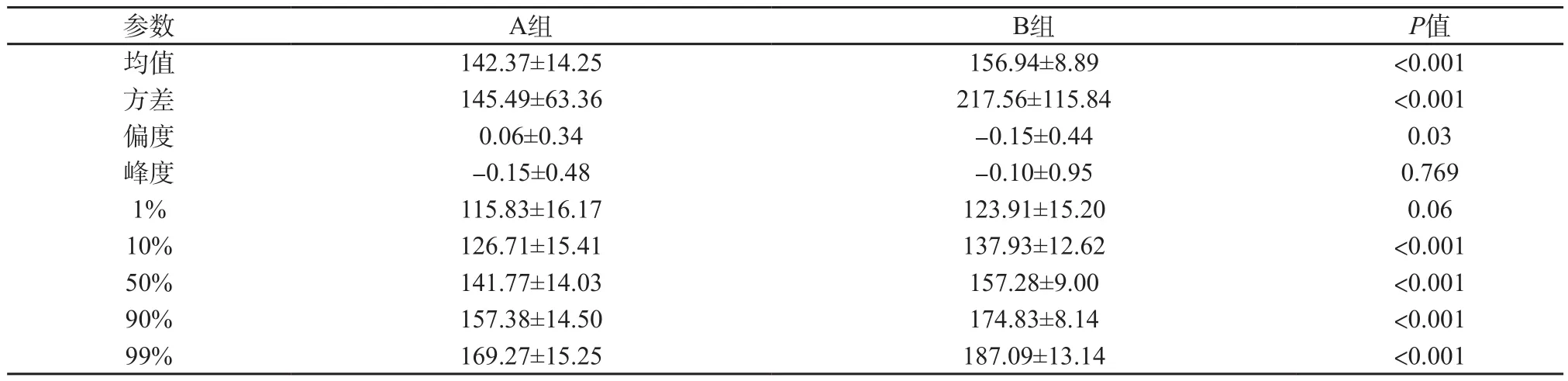
表2 缓解组(A组)与非缓解组(B组)之间门静脉期CT图像直方图分析的比较

图3 门静脉期基线CT图像直方图各参数的ROC曲线
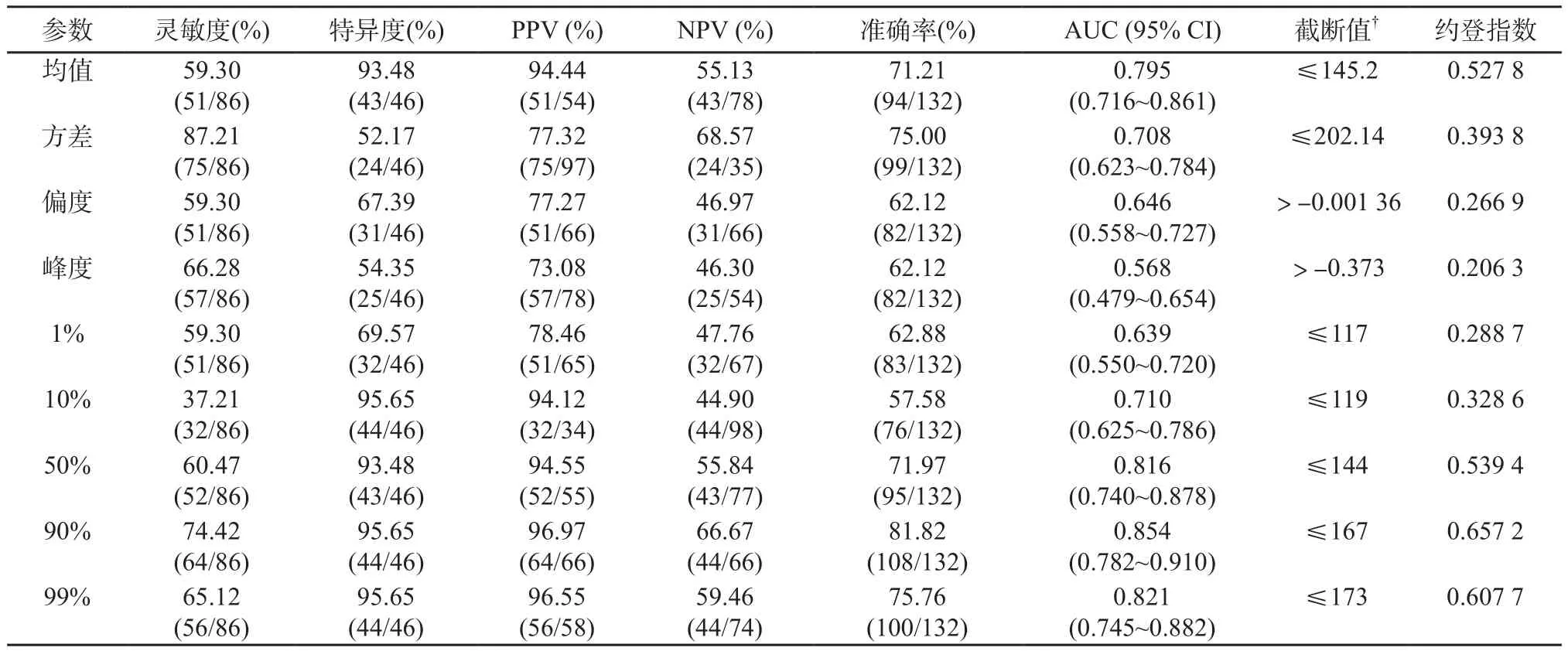
表3 纹理参数判断缓解组与非缓解组的诊断效能
偏度的绝对值越大表示其分布形态的偏斜程度越大,方差表示平均值的变化情况,偏度和方差值的大小与同质均匀性成反比[35]。因此,高的偏度值和方差表示肿瘤具有较高的异质性。肿瘤的异质性是恶性肿瘤的公认特征,反映区域内高细胞密度、坏死、出血及黏液样变[36]。肿瘤异质性是预后的重要因素,肿瘤异质性越高可能与肿瘤级别越高相关[37]。本研究结果与某些研究[34,38-39]相似,他们发现高偏度值和标准偏差代表肿瘤的异质性明显,预示患者预后较差,与本研究中治疗后非缓解组的偏度值和方差高相符。本研究显示,90th百分位数具有较高的诊断准确率(81.82%),AUC值为0.854。90th百分位数是一个量度,表示包含了90% CT值的观测数据,并剔除了直方图中10%的最大值,这些最大值可能代表ROI勾画过程中无法去除的肿瘤部分供血分支血管。因此,去除这部分10%的最大值,能更准确地反映肿瘤本身的真实强化特征。
目前,对于CT图像纹理分析扫描期相的选择并无固定标准。Goh等[40]采用动脉期图像评估肾细胞癌患者酪氨酸激酶治疗后肿瘤纹理的变化。另一些研究使用平扫来评估肝脏肿瘤[41]、肺癌[38]或食管癌[42]。然而,大多数研究[20]采用门静脉期图像的纹理来分析CRLM患者。本研究对门静脉期图像进行纹理分析,这是因为CRC患者监视随访期间,CT扫描常规需行门静脉期检查;且以往研究指出,CT门静脉期观察到的肝脏纹理与生物学性质相关,如总肝血流量和葡萄糖代谢,可作为CRC患者有价值的生物标记[33]。
本研究存在以下不足之处:首先,是一项回顾性研究,存在选择偏倚。其次,样本量较小且为单中心研究,需大样本、多中心及前瞻性研究来验证。第三,剔除了其他病理类型的CRC(如印戒细胞癌、黏液腺癌),最终选择的患者均为结直肠腺癌,缺少其他病理类型的转移。但其他病理类型例数非常少,因此对研究结果的影响甚微。第四,采用最大层面的方法勾画ROI,没有对整个病灶进行分析,可能会对结果造成一定的影响。但阅读相关文献,发现2D与3D纹理分析在CRLM患者治疗前预测疗效结果相似[43]。最后,由于统计数据量大及图像后处理的限制,没有进行其他期图像的研究,没有对纹理特征的其他参数(如灰度共生矩阵、游程矩阵、梯度模型、自回归模型和基于傅里叶变换的纹理特征)进行分析,希望以后能对此进行深入研究。
4 结 语
CRLM患者基线CT门静脉期灰度直方图分析可帮助预测新辅助治疗后是否缓解,具有一定的临床应用价值。
[1] JEMAL A, BRAY F, CENTER M M, et al. Global cancer statistics [J]. CA Cancer J Clin, 2011, 61(2): 69-90.
[2] VIBERT E, CANEDO L, ADAM R. Strategies to treat primary unresectable colorectal liver metastases [J]. Semin Oncol, 2005, 32(6 Suppl 8): S33-S39.
[3] KEMENY N. Management of liver metastases from coloreetal cancer [J]. Oneology (Williston Park), 2006, 20(10): 1161-1176, 1179-1180, 1166-1185.
[4] LAU W, LAI E. Hepatic resection for colorectal liver metastases [J]. Singapore Med J, 2007, 48(7): 635-639.
[5] TANIAI N, AKIMARU K, YOSHIDA H, et al. Surgical treatment for better prognosis of patients with liver metastases from colorectal cancer [J]. Hepatogastroenterology, 2007, 54(78): 1805-1809.
[6] ARRU M, ALDRIGHETTI L, CASTOLDI R, et al. Analysis of prognostic factors influencing long-term survival after hepatic resection for metastatic colorectal cancer [J]. World J Surg, 2008, 32(1): 93-103.
[7] FOSTER J. Treatment of metastatic disease of the liver: a skeptic’s view [J]. Semin Liver Dis, 1984, 4(2): 170-179.
[8] TIMMERMAN R D, BIZEKIS C S, PASS H I, et al. Local surgical, ablative, and radiation treatment of metastases [J]. CA Cancer J Clin, 2009, 59(3): 145-170.
[9] BENOIST S, NORDLINGER B. Neoadjuvant treatment before resection of liver metastases [J]. Eur J Surg Oncol, 2007, 33(Suppl 2): S35-S41.
[10] REDDY S K, BARBAS A S, CLARY B M. Synchronous colorectal liver metastases: is it time to reconsider traditional paradigms of management? [J]. Ann Surg Oncol, 2009, 16(9): 2395-2410.
[11] POULTSIDES G A, SERVAIS E L, SALTZ L B, et al. Outcome of primary tumor in patients with synchronous stage Ⅳ colorectal cancer receiving combination chemotherapy without surgery as initial treatment [J]. J Clin Oncol, 2009, 27(20): 3379-3384.
[12] MEHTA N N, RAVIKUMAR R, COLDHAM C A, et al. Effect of preoperative chemotherapy on liver resection for colorectal liver metastases [J]. Eur J Surg Oncol, 2008, 34(7): 782-786.
[13] GRUENBERGER B, TAMANDL D, SCHUELLER J, et al. Bevacizumab, capecitabine, and oxaliplatin as neoadjuvant therapy for patients with potentially curable metastatic colorectal cancer [J]. J Clin Oncol, 2008, 26(11): 1830-1835.
[14] COSKUN U, BUYUKBERBER S, YAMAN E, et al. Xelox (capecitabine plus oxaliplatin) as neoadjuvantchemotherapy of unresectable liver metastases in colorectal cancer patients [J]. Neoplasma, 2008, 55(1): 65-70.
[15] CASSIDY J, CLARKE S, DIAZ-RUBIO E, et al. XELOX vs. FOLFOX-4 as first-line therapy for metastatic colorectal cancer: NO16966 updated results [J]. Br J Cancer, 2011, 105(1): 58-64.
[16] COLUCCI G, GEBBIA V, PAOLETTI G, et al. PhaseⅢ randomized trial of FOLFIRI versus FOLFOX4 in the treatment of advanced colorectal cancer: a multicenter study of the Gruppo Oncologico Dell’Italia Meridionale [J]. J Clin Oncol, 2005, 23(22): 4866-4875.
[17] NAKANO H, OUSSOULTZOGLOU E, ROSSO E, et al. Sinusoidal injury increases morbidity after major hepatectomy in patients with colorectal liver metastases receiving preoperative chemotherapy [J]. Ann Surg, 2008, 247(1): 118-124.
[18] CHOTI M A. Chemotherapy-associated hepatotoxicity: do we need to be concerned? [J]. Ann Surg Oncol, 2009, 16(9): 2391-2394.
[19] MATSUHASHI N, TAKAHASHI T, KATO J, et al. Computed tomography evaluation of morphological changes, clinical response and survival in colorectal cancer liver metastasis treated by regorafenib: A case report [J]. Mol Clin Oncol, 2016, 5(6): 807-810.
[20] AHN S J, KIM J H, PARK S J, et al. Prediction of the therapeutic response after FOLFOX and FOLFIRI treatment for patients with liver metastasis from colorectal cancer using computerized CT texture analysis [J]. Eur J Radiol, 2016, 85(10): 1867-1874.
[21] RAJKUMAR V, GOH V, SIDDIQUE M, et al. Texture analysis of 125I-A5B7 anti-CEA antibody SPECT differentiates metastatic colorectal cancer model phenotypes and anti-vascular therapy response [J]. Br J Cancer, 2015, 112(12): 1882-1887.
[22] MOUGIAKAKOU S G, VALAVANIS I K, NIKITA A, et al. Differential diagnosis of CT focal liver lesions using texture features, feature selection and ensemble driven classifiers [J]. Artif Intell Med, 2007, 41(1): 25-37.
[23] HAFEEZ S, ALAM M S, SAJJAD Z, et al. Triphasic computed tomography (CT) scan in focal tumoral liver lesions [J]. J Pak Med Assoc, 2011, 61(6): 571-575.
[24] CASTELLANO G, BONILHA L, LI L M, et al. Texture analysis of medical images [J]. Clin Radiol, 2004, 59(12): 1061-1069.
[25] EMBLEM K E, NEDREGAARD B, NOME T, et al. Glioma grading by using histogram analysis of blood volume heterogeneity from MR-derived cerebral blood volume maps [J]. Radiology, 2008, 247(3): 808-817.
[26] CHOI Y S, KIM D W, LEE S K, et al. The added prognostic value of preoperative dynamic contrastenhanced MRI histogram analysis in patients with glioblastoma: Analysis of overall and progression-free survival [J]. AJNR Am J Neuroradiol, 2015, 36(12): 2235-2241.
[27] POPE W B, KIM H J, HUO J, et al. Recurrent glioblastoma multiforme: ADC histogram analysis predicts response to bevacizumab treatment [J]. Radiology, 2009, 252(1): 182-189.
[28] SZCZYPINSKI P M, STRZELECKI M, MATERKA A, et al. MaZda—a software package for image texture analysis [J]. Comput Methods Programs Biomed, 2009, 94(1): 66-76.
[29] EISENHAUER E A, THERASSE P, BOGAERTS J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1) [J]. Eur J Cancer, 2009, 45(2): 228-247.
[30] GOLDBERG R M, SARGENT D J, MORTON R F, et al. A randomized controlled trial of fluorouracil plus leucovorin, irinotecan, and oxaliplatin combinations in patients with previously untreated metastatic colorectal cancer [J]. J Clin Oncol, 2004, 22(1): 23-30.
[31] TOURNIGAND C, ANDRE T, ACHILLE E, et al. FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer: a randomized GERCOR study [J]. J Clin Oncol, 2004, 22(2): 229-237.
[32] KABBINAVAR F F, SCHULZ J, MCCLEOD M, et al. Addition of bevacizumab to bolus fluorouracil and leucovorin in first-line metastatic colorectal cancer: results of a randomized phase Ⅱ trial [J]. J Clin Oncol, 2005, 23(16): 3697-3705.
[33] GANESHAN B, MILES K A, YOUNG R C, et al. In search of biologic correlates for liver texture on portalphase CT [J]. Acad Radiol, 2007, 14(9): 1058-1068.
[34] MILES K A, GANESHAN B, GRIFFITHS M R, et al. Colorectal cancer: texture analysis of portal phase hepatic CT images as a potential marker of survival [J]. Radiology, 2009, 250(2): 444-452.
[35] MILES K A, GANESHAN B, HAYBALL M P. CT texture analysis using the filtration-histogram method: what do the measurements mean? [J]. Cancer Imaging, 2013, 13(3): 400-406.
[36] RAO R K. Prospective study of colorectal cancer in the West of Scotland: 10-year follow-up [J]. Br J Surg, 1990, 77(12): 1434.
[37] ECCLES S A, WELCH D R. Metastasis: recent discoveries and novel treatment strategies [J]. Lancet, 2007,369(9574): 1742-1757.
[38] GANESHAN B, ABALEKE S, YOUNG R C, et al. Texture analysis of non-small cell lung cancer on unenhanced computed tomography: initial evidence for a relationship with tumour glucose metabolism and stage [J]. Cancer Imaging, 2010, 10: 137-143.
[39] KATO H, KANEMATSU M, ZHANG X, et al. Computer-aided diagnosis of hepatic fibrosis: preliminary evaluation of MRI texture analysis using the finite difference method and an artificial neural network [J]. AJR Am J Roentgenol, 2007, 189(1): 117-122.
[40] GOH V, GANESHAN B, NATHAN P, et al. Assessment of response to tyrosine kinase inhibitors in metastatic renal cell cancer: CT texture as a predictive biomarker [J]. Radiology, 2011, 261(1): 165-171.
[41] HUANG Y L, CHEN J H, SHEN W C. Diagnosis of hepatic tumors with texture analysis in nonenhanced computed tomography images [J]. Acad Radiol, 2006, 13(6): 713-720.
[42] GANESHAN B, SKOGEN K, PRESSNEY I, et al. Tumour heterogeneity in oesophageal cancer assessed by CT texture analysis: preliminary evidence of an association with tumour metabolism, stage, and survival [J]. Clin Radiol, 2012,67(2): 157-164.
[43] LUBNER M G, STABO N, LUBNER S J, et al. CT textural analysis of hepatic metastatic colorectal cancer: pre-treatment tumor heterogeneity correlates with pathology and clinical outcomes [J]. Abdom Imaging, 2015, 40(7): 2331-2337.
Value of CT texture analysis in evaluating response to neoadjuvant chemotherapy for colorectal liver metastases
HU Feixiang, HU Tingdan, TONG Tong, PENG Weijun
(Department of Diagnostic Radiology, Fudan University Shanghai Cancer Center; Department of Oncology, Shanghai Medical College, Fudan University, Shanghai 200032, China)
PENG Weijun E-mail: cjr.pengweijun@vip.163.com
Objective:To explore the value of histogram analysis of baseline CT portal images before treatment in predicting the response of patients with colorectal liver metastases (CRLMs) to neoadjuvant chemotherapy.Methods:Thirty-four patients (a total of 132 lesions) diagnosed with CRLM were retrospectively enrolled and underwent contrast-enhanced CT before and after neoadjuvant chemotherapy (FOLFOX, FOLFIRI or CapeOX ). All patients underwent pre-treatment CT baseline scan withinfour weeks for primary tumor assessment and a second CT scan in 2 to 3 months, for response evaluation. Histogram of CT portal images of patients with CRLM was analyzed and response was mainly assessed using Response Evaluation Criteria in Solid Tumors (RECIST) Version 1.1. The texture parameters of the metastatic tumor were analyzed statistically to fi nd the dif f erences in baseline CT histogram parameters between responding group and non-responding group before and after treatment. The receiver operating characteristic (ROC) curves were depicted to characterize each parameter value in evaluating the treatment outcomes. The optimal cutof f value (obtained according to the maximal Youden index = sensitivity + specif i city-1), the corresponding sensitivity, specif i city, positive predictive value (PPV), negative predictive value (NPV) and accuracy were calculated. Regions of interests (ROIs) were manually drawn on the largest cross-sectional area of the primary lesions by two radiologists in consensus.Results:Twenty-one responding and 13 non-responding patients were evaluated. The values of mean, variance, skewness and percentile (10th, 50th, 90th, 99th) in responding group were much lower than those in non-responding group (P<0.05). The kurtosis and 1st percentile values between the two groups had no significant difference (P=0.769, P=0.06, respectively). The optimal cutoff value for the accurate identif i cation of responding patients was 167 for 90th percentile (74.42% sensitivity, 95.65% specif i city, 96.97% PPV, 66.67% NPV, 81.82% accuracy, and 0.854 area under curve, respectively).Conclusion:CT histogram analysis of baseline CT portal images before treatment can help to predict the response of patients with CRLM after neoadjuvant chemotherapy.
Texture analysis; Histogram; Colorectal liver metastasis
R445.3
A
1008-617X(2017)02-0106-08
2017-04-01)
国家自然科学基金项目(No:81501437)
彭卫军 E-mail:cjr.pengweijun@vip.163.com