早期非小细胞肺癌切除范围的临床研究
2016-12-23许庆生刘宝东王若天支修益
胡 牧 张 毅 许庆生 刘宝东 苏 雷 王若天 支修益
(首都医科大学宣武医院胸外科,北京 100053)
· 肺癌精准治疗 ·
早期非小细胞肺癌切除范围的临床研究
胡 牧 张 毅 许庆生 刘宝东 苏 雷 王若天 支修益*
(首都医科大学宣武医院胸外科,北京 100053)
目的 比较肺叶切除和胸腔镜亚肺叶切除在治疗早期非小细胞肺癌的安全性和近期疗效。方法 将直径≤2 cm的早期肺癌回顾性分成胸腔镜下亚肺叶切除组和肺叶切除组,比较两组住院手术期间的各项指标(手术时间、手术出血量、术后住院时间、术后合并症)和术后1年病死率及复发率、术后1年肺功能减少比率。结果 2组手术时间比较,亚肺叶切除组短于肺叶切除组(P=0.000)。2组在手术出血量、术后住院时间和术后合并症方面比较,差异无统计学意义(P>0.05)。术后1年对患者进行随访,两组均未发现死亡病例,未发现肿瘤复发转移情况。亚肺叶切除组在术后1年肺功能减少比例中明显优于肺叶切除组,差异有统计学意义(P=0.000)。结论 胸腔镜下亚肺叶切除术对于早期非小细胞肺癌患者安全性和有效性在本研究中得到一定证实。
非小细胞肺癌;亚肺叶切除;肺叶切除;早期
肺癌是我国最常见的恶性肿瘤,居恶性肿瘤死亡原因第1位,其中80%以上为非小细胞肺癌(non-small cell lung cancer, NSCLC)[1]。外科手术依然是早期肺癌最有效的治疗方法,目前肺癌的标准手术方式是肺叶切除加区域淋巴结清扫。随着新一代螺旋CT 在临床上的广泛应用,发现越来越多的直径≤2 cm的早期周围型NSCLC患者[2]。
本研究旨在探讨亚肺叶切除术对于直径≤2 cm的早期周围型NSCLC的可行性和有效性,并与肺叶切除术进行回顾性对照临床研究。目的是确定亚肺叶切除术是否适用于治疗早期周围型NSCLC,进一步提高早期肺癌外科治疗效果,提高患者术后生活质量。
1 资料与方法
1.1 一般资料
首都医科大学宣武医院2011年10月至2014年12月施行胸腔镜下亚肺叶切除(包括解剖性肺段切除和楔形切除)和肺叶切除治疗早期非小细胞肺癌患(T≤2 cm N0M0)者各30例按1∶1分配至亚肺叶切除组和肺叶切除组。2组患者术前均行血常规、尿常规、肝肾功能、凝血功能、肿瘤标志物、心肺功能评估等常规检查,行头颅MRI、上腹部CT、骨扫描或PET/CT等排除远处转移。个别患者如为肺毛玻璃样病变(ground glass opacity,GGO)或结节较小估计术中定位困难者,术前采用CT定位,穿刺后在病变旁注入生物胶标记。
1.2 手术方法
所有手术均在全腔镜下完成,采用双腔气管插管全身麻醉,单肺通气。取健侧卧位,采用3个切口完成(腋中线第7肋间为胸腔镜观察孔,腋前线一锁骨中线间3~4肋间为主操作孔,腋后线7~9肋间为副操作孔)。术前无病理的患者,先行肺楔形切除术,术中快速病理示恶性结节后,经探查后认为可行肺叶或亚肺叶(包括楔形切除和肺段切除)切除术,2组均行淋巴结清扫(左侧5、6、7、10组,右侧2、4、7、10组)。
1.3 主要评价指标
手术的安全性和可行性及短期疗效评估。肺叶切除已经是肺癌根治的经典术式,而肺段切除和楔形切除也是成熟的手术方式。短期疗效评估定义为从自患者接受本研究手术治疗后到首次记录疾病进展时间。次要指标:肺功能第1秒用力呼气容积(forced expiratory volume in 1 second, FEV1)。
1.4 统计学方法
2 结果
各组病例基本临床资料比较,差异无统计学意义(表1、2)。2组手术情况的比较亚肺叶切除组在手术时间上要短于肺叶切除组(P=0.000)。在亚组分析中楔形切除组手术时间明显短于肺段切除组,另外楔形切除组手术出血量也明显少于肺段切除组(表3)。
在术后住院时间上楔形切除组也少于肺段切除组,2组的术后住院时间是[(4.30±0.67)dvs(5.50±1.00)d]比较,差异有统计学意义(P=0.003)(表4)。如果单独把肺段切除组和肺叶切除组对比,手术时间、术中出血、术后住院时间和合并症发生情况差异均无统计学意义(P>0.05)(表5)。亚肺叶切除和肺叶切除2组在手术出血量、术后住院时间和术后合并症方面差异无统计学意义(P>0.05)。
表1 亚肺叶切除组和肺叶切除组患者临床信息对比
Tab.1 Comparison of clinical information between patients of sublobectomy and lobectomy groups

ItemSublobectomyLobectomyPGender Male11120.571 Female1918Age/a65.57±5.4064.17±6.170.321Tumordiameter/mm1.16±0.421.14±0.330.714Tumorsite Leftupperlobe1140.423 Leftlowerlobe6150.601 Rightupperlobe460.439 Rightmiddlelobe040.317 Rightlowerlobe9110.714CTimage PureGGO12100.501 PartialGGO460.474 Solid14140.491Pathology Squamous120.469 Invasiveadenoma11130.398 Mircoinvasiveadenoma13150.376 Adenomainsitu520.546
GGO:ground glass opacity.
表2 亚肺叶切除组亚组患者临床信息对比
Tab. 2 Comparison of clinical information between patients of sublobectomy subgroups
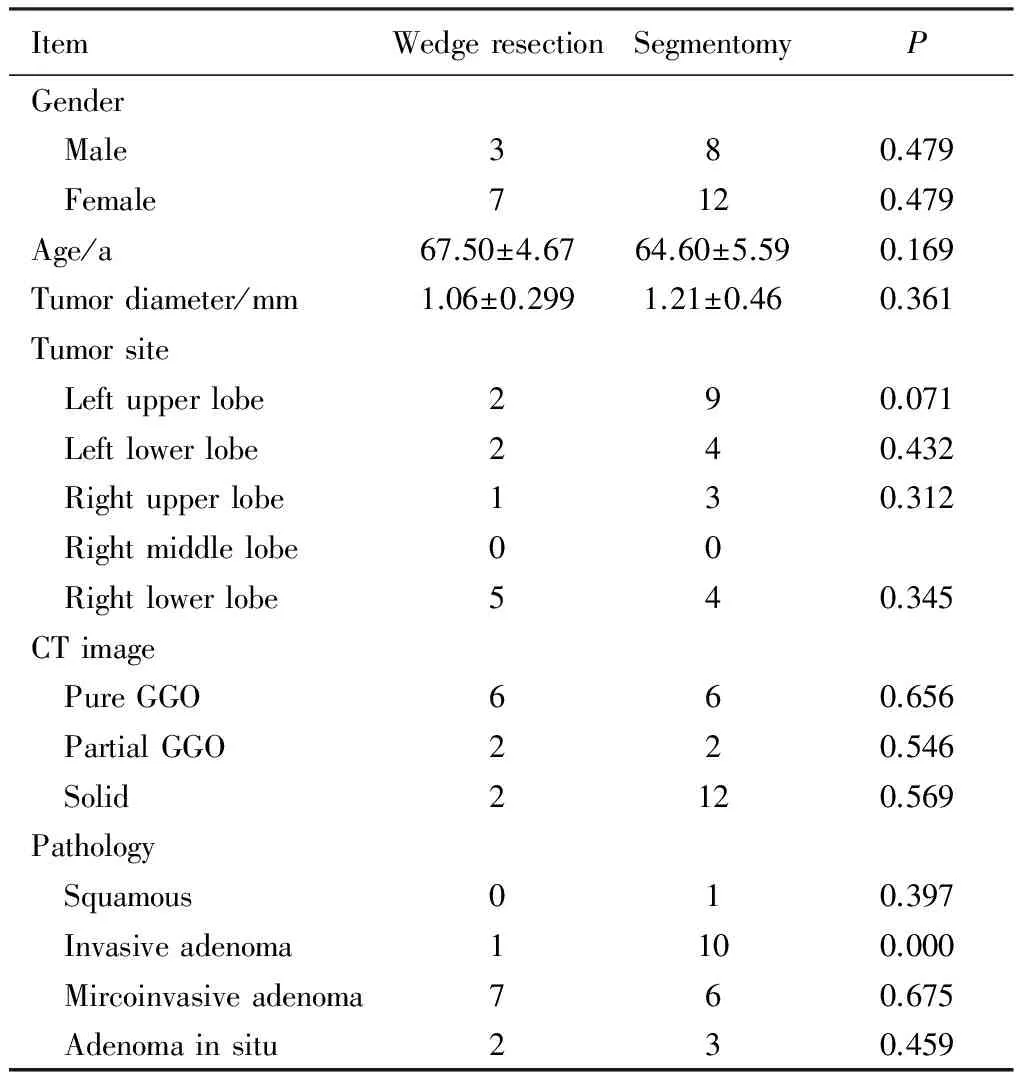
ItemWedgeresectionSegmentomyPGender Male380.479 Female7120.479Age/a67.50±4.6764.60±5.590.169Tumordiameter/mm1.06±0.2991.21±0.460.361Tumorsite Leftupperlobe290.071 Leftlowerlobe240.432 Rightupperlobe130.312 Rightmiddlelobe00 Rightlowerlobe540.345CTimage PureGGO660.656 PartialGGO220.546 Solid2120.569Pathology Squamous010.397 Invasiveadenoma1100.000 Mircoinvasiveadenoma760.675 Adenomainsitu230.459
GGO:ground glass opacity.
表3 肺叶切除组和亚肺叶切除组患者手术情况对比
Tab.3 Comparison of operation between patients of sublobectomy and lobectomy groups

ItemSublobectomyLobectomyPOperationtime/min123.50±34.57157.00±22.46<0.001Intraoperativebloodloss/mL134.33±89.47163.00±74.890.079Postoperativehospitalstay/d5.10±1.065.73±0.830.012Postoperativecomplications/case15130.551
表4 亚肺叶切除组亚组患者手术情况对比
Tabl.4 Comparison of operation between patients of sublobectomy subgroups

ItemWedgeresectionSegmentomyPOperationtime/min86.5±10.55142.00±26.28<0.001Intraoperativebloodloss/mL50.00±20.00176.50±80.09<0.001Postoperativehospitalstay/d4.30±0.675.50±1.000.003Postoperativecomplications/case411<0.001
表5 肺叶切除组和肺段切除组患者手术情况对比
Tab. 5 Comparison of operation between patients of lobectomy and segmentectomy groups

ItemSegmentomyLobectomyPOperationtime/min142.00±26.28157.00±22.460.306Intraoperativebloodloss/mL176.50±80.09163.00±74.890.505Postoperativehospitalstay/d5.50±1.005.73±0.830.353Postoperativecomplications/case11130.675
术后1年对患者进行随访。2组均未发现死亡病例,未发现肿瘤复发转移情况。亚肺叶切除组在术后1年肺功能减少比率(6.03%±2.37%)中明显优于肺叶切除组(9.87%±1.66%) (P=0.000),类似的肺功能降低在楔形切除组(3.36%±1.37%)要优于肺段切除组(7.58%±1.07%)(P=0.000)。
3 讨论
肺癌是严重威胁人类生命健康的疾病,病死率居恶性肿瘤首位[3]。随着新一代螺旋CT在肺癌筛查和健康体检人群中的广泛应用,越来越多最大径<2 cm的早期周围型肺癌获得临床诊断。早期肺癌的标准手术方式为肺叶切除+系统淋巴结清扫。一些回顾性临床研究的结果[4-5]显示,对于因心肺功能不佳而不能接受肺叶切除的老年早期肺癌患者,亚肺叶切除术尤其是解剖性肺段切除术可以获得类似于肺叶切除的治疗效果。
1993年Kirby等[6-7]首次报告了胸腔镜肺叶切除术,目前在世界范围内已被广泛用于早期NSCLC及肺部良性结节的治疗,其安全、微创等特点已得到临床充分验证。Roviaro等[8]于1993年首次报告胸腔镜肺段切除术。有研究[9-10]显示,对于I A期NSCLC,胸腔镜解剖性肺段切除与肺叶切除术相比,淋巴结清除组数及个数相似,局部复发率和生存率相似。而解剖性肺段切除与肺楔形切除相比,肺段切除能保证足够的切缘以及段间、叶间淋巴结的清扫,淋巴结切除个数、局部复发率及5年生存率均优于肺楔形切除。美国匹兹堡实验研究中心的研究[11]结果表明,术后病理为I A期的NSCLC,肺叶切除和肺段切除的两组患者在术后局部复发率及5年生存率方面差异无统计学意义。
随着影像学技术的进步和肺癌筛查的突破性进展,越来越多的GGO病变被发现[12]。有研究[13-14]显示这些GGO病变通常倾向于原位腺癌(adenocarcinoma in situ, AIS)或微浸润腺癌(minimally invasive adenocarcinoma, MIA),对于这些病变来说手术治疗效果较好[15],因此对这一类NSCLC患者而言,亚肺叶切除术有可能成为其标准术式。2014年,Tsutani等[16]分析了239例呈GGO样改变的临床Ia期肺腺癌患者临床资料,其中有90例肺叶切除术、56例肺段切除术、93例肺楔形切除术,术后3年无病生存率(disease free survival, DFS)分别为96.4%、96.1% 和98.7%,3者比较,差异无统计学意义(P=0.440)。这些回顾性研究虽然证据等级较低,但为前瞻性研究提供了一定的支持。
从本研究情况来看2组手术情况的比较亚肺叶切除组在手术时间上要短于肺叶切除组(P=0.000),主要的原因是亚肺叶组的楔形切除组手术时间明显较肺段及肺叶切除短,因此拉低了亚肺叶组的手术时间,单纯比较肺段切除和肺叶切除组手术时间差异无统计学意义(P>0.05)。从这一组患者的情况分析楔形切除组在手术创伤上要小于肺段及肺叶切除组。而短期的随访显示肿瘤治疗效果一致。从术后1年肺功能损失来看,亚肺叶肺切除组较肺段切除组有优势(P=0.000),考虑到亚肺叶组有部分肺楔形切除的患者,因此可能放大了肺功能保护的优势。本研究中楔形切除组的数据与肺段切除组相比,在手术时间、出血等创伤保护方面有明显优势,而在短期的随访中并未表现出肿瘤治疗效果上的劣势,可能和楔形切除组分期更早,病变更小,且纯GGO例数较多有关。将来在1 cm以下超早期肺癌治疗上,可以做一些深入研究。
胸腔镜下亚肺叶切除术对于早期非小细胞肺癌患者安全性和有效性在本研究中得到一定证实,但还存在一些局限,如例数较少、非随机,本单位已经在2014年启动了多中心开放、对照的早期肺癌切除范围研究,相信随着同类前瞻性研究结果发布,胸腔镜下亚肺叶切除术极有可能成为治疗早期非小细胞肺癌患者的一种标准手术方式。
[1] 诸葛雪朋. 胸腔镜解剖性肺段切除术用于治疗老年早期肺癌患者的研究[J]. 中国实用医刊, 2015, 3(42):13-14.
[2] 支修益. 解剖性肺段切除治疗早期非小细胞肺癌[J]. 中华外科杂志, 2015, 10(53):794-797.
[3] Siegel R, Ma J M, Zou Z H, et al. Cancer statistics[J], 2014 CA Cancer J Clin, 2014, 64(1): 9-29.
[4] Okada M, Koike T, Higashiyama M, et al. Radical sublobar resection for small-sized non-small cell lung cancer: a multicenter study[J]. J Thorac Cardiovasc Surg, 2006, 132(4): 769-775.
[5] Okumura M, Goto M, Ideguchi K, et al. Factors associated with outcome of segmentectomy for non-small cell lung cancer: long-term follow-up study at a single institution in Japan[J]. Lung Cancer, 2007, 58(2): 231-237.
[6] Kirby T J, Rice T W. Thoracoscopic lobectomy[J]. Ann Thorac Surg, 1993, 56(3): 784-786.
[7] Kirby T J, Rice T W. Video-assisted pulmonary lobectomy[J]. Semin Thorac Cardiovasc Surg, 1993, 5(4): 316-320.
[8] Roviaro G C, Rebufft C, Vareli F, et al. Videoendoscopic thoracic surgery[J]. Int Surg, 1993, 78(1): 4-9.
[9] Schuchert M J, Abbas G, Awais O, et al. Anatomic segmentectomy for the solitary pulmonary nodule and early-stage lung cancer[J]. Ann Thorac Surg, 2012, 93(6): 1780-1785.
[10]Yendamuri S, Sharma R, Demmy M, et al. Temporal trends in outcomes following sublobar and lobar resections for small (
[11]Koike T, Yoshiya K, Tsuchida M, et al. Risk factor analysis of locoregional recurrence after sublobar resection in patients with clinical stage ⅠA non-small cell lung cancer[J]. J Thorac Cardiovasc Surg, 2013, 146(2): 372-328.
[12]Kramer B S, Berg C D, Aberle D R, et al. Lung cancer screening with low-dose helical CT: results from the National Lung Screening Trial (NLST)[J]. J Med Screen, 2011, 18(3): 109-111.
[13]Suzuki K, Asamura H, Kusumoto M, et al. “Early” peripheral lung cancer: prognostic significance of ground glass opacity on thin-section computed tomographic scan[J]. Ann Thorac Surg, 2002. 74(5): 1635-1639.
[14]Asamura H. Minimally invasive open surgery approach for the surgical resection of thoracic malignancies[J]. Thorac Surg Clin, 2008, 18(3): 269-273.
[15]Asamura H, Hishida T, Suznki K, et al. Radiographically determined noninvasive adenocarcinoma of the lung: survival outcomes of Japan clinical oncology group 0201[J]. J Thorac Cardiovasc Surg, 2013, 146(1): 24-30.
[16]Tsutani Y, Miyata Y, Nakayama H, et al. Appropriate sublobar resection choice for ground glass opacity-dominant clinical stage ⅠA lung adenocarcinoma: wedge resection or segmentectomy[J]. Chest, 2014, 145(1): 66-71.
编辑 慕 萌
Clinical study for resection range for early stage non-small cell lung cancer patients
Hu Mu, Zhang Yi, Xu Qingsheng, Liu Baodong, Su Lei, Wang Ruotian, Zhi Xiuyi*
(DepartmentofThoracicSurgery,XuanwuHospital,CapitalMedicalUniversity,Beijing100053,China)
Objective To compare video assisted thoracic surgery(VATS) lobectomy and sublobectomy in the treatment of early stage non-small cell lung cancer on safety and short term follow up. Methods The early lung cancer patients with lesion 2 cm or less in diameter were divided into lobectomy and sublobectomy resection group. Two groups were compared in the hospitalization after operation, operation time, surgical blood loss, postoperative complications and postoperative recurrence at 1-year, mortality and postoperative lung function reduction rate after 1 year. Results Comparing two groups, sublobecomy group had a shorter operation time than lobectomy group (P=0.000). Surgical blood loss, postoperative hospital stay and postoperative complications had no significant difference (P>0.05) between two groups. After 1 year follow-up, no mortality was found in any group, no tumor recurrence or metastasis was found in any group. In sublobectomy group, reduction of lung function 1 year after surgery was obviously better than the ratio of lobectomy group (P=0.000). Conclusion Safety and effectiveness of VATS sublobectomy for early stage non-small cell lung cancer patients compared with lobectomy have been established in this study.
non-small cell lung cancer; sublobectomy resection; lobectomy; early stage
北京市科委重大项目(D14110700020000)资助。This study was supported by Beijing Municipal Science and Technology Commission Major Projects (D14110700020000) .
时间:2016-12-14 20∶19
http://www.cnki.net/kcms/detail/11.3662.r.20161214.2019.026.html
10.3969/j.issn.1006-7795.2016.06.009]
R 734.2
2016-10-03)
*Corresponding author, E-mail:xiuyizhi2015@163.com
