节拍化疗在乳腺癌晚期治疗中的临床应用进展Δ
2016-12-19蔡鑫君浙江省肿瘤医院药剂科杭州300杭州市红十字会医院药剂科杭州30003
程 斌,蔡鑫君,王 增(.浙江省肿瘤医院药剂科,杭州 300;.杭州市红十字会医院药剂科,杭州30003)
·综述讲座·
节拍化疗在乳腺癌晚期治疗中的临床应用进展Δ
程斌1*,蔡鑫君2,王增1(1.浙江省肿瘤医院药剂科,杭州310022;2.杭州市红十字会医院药剂科,杭州310003)
目的:了解节拍化疗在乳腺癌晚期治疗中的临床应用进展。方法:查阅近年来国内外相关文献,就节拍化疗的作用机制及其在乳腺癌晚期治疗中的临床应用进展进行归纳和总结。结果:节拍化疗主要通过抑制肿瘤血管的生成、减少肿瘤干细胞数量、调节免疫功能、诱导肿瘤休眠等多方面来实现抗肿瘤作用。单药节拍化疗可减少用药品种,降低化疗费用,但会导致疗效降低;多药联合节拍化疗可通过多靶点作用增加疗效,但会增加费用并降低患者顺应性;节拍化疗联合内分泌治疗特别适合激素相关的乳腺癌,可减轻耐药程度,提高疗效。结论:节拍化疗在乳腺癌晚期治疗中具有良好的应用前景,可提高疗效,减少不良反应,延长患者生存期,是乳腺癌晚期治疗的一种新方法。
节拍化疗;乳腺癌晚期;肿瘤干细胞;内分泌
近年来,恶性肿瘤的临床治疗取得了显著进展,化疗仍然是其临床治疗的重要方法,但传统化疗方案大都选择最大耐受剂量(Maximum tolerated dose,MTD),旨在最大限度地杀伤肿瘤细胞,达到最佳的治疗效果。然而,这种化疗方法仅对一些血液恶性肿瘤和早期恶性肿瘤有较好的治愈率,大部分恶性肿瘤患者化疗后病情仍会进展,且MTD存在毒性大、不良反应多、作用不持久、化疗间歇期肿瘤重新生长和易引起肿瘤细胞耐药等缺点,限制了其临床应用[1]。20世纪90年代末以来,越来越多的研究显示,持续、低剂量的抗肿瘤药物可以明显抑制肿瘤血管的生成,并促进肿瘤细胞凋亡[2-3]。Hanahan D等[4]的研究在此基础上提出了节拍化疗(Metronomic chemotherapy)的概念。与传统化疗方法相比,节拍化疗采用低剂量(剂量一般仅为MTD方案的1/3~1/10)、高频率的给药方式,并缩短治疗过程中的停药间隙。节拍化疗的主要作用靶点不再是肿瘤细胞本身,而是影响与肿瘤细胞生长密切相关的血管内皮细胞、循环内皮祖细胞和肿瘤干细胞(Tumor stem cell,TSC)的增殖和活性,并调节免疫功能和诱导肿瘤细胞休眠,不仅能够发挥抗肿瘤作用,而且能够避免传统化疗引起的肿瘤细胞耐药[5]。同时,节拍化疗可以明显减少抗肿瘤药物引起的各种不良反应,特别适用于晚期恶性肿瘤或存在转移病灶的肿瘤患者,延长生存期,提高生存质量,降低化疗费用[6-7]。
乳腺癌是常见的妇科恶性肿瘤,其肿瘤转移、耐药和复发等问题均是困扰临床的难题。目前,越来越多的乳腺癌节拍化疗方案被纳入临床研究,采用的方案包括单药节拍化疗,两种或两种以上抗肿瘤药物节拍化疗,节拍化疗与抗肿瘤血管生成药物的联用,以及节拍化疗和激素类药物的联用等,均显示出其较好的治疗效果。笔者查阅近年来国内外相关文献,就乳腺癌晚期节拍化疗的临床研究作一综述。
1 节拍化疗的作用机制
1.1抑制肿瘤血管的生成
抑制肿瘤血管的生成是由Folkman J[7]最早提出的观点,其认为血管生成在肿瘤的生长和转移过程中起到关键作用。肿瘤新生血管中的活化内皮细胞对小剂量的化疗药物有较强的敏感度。Mannel RS等[8]研究发现,低剂量的紫杉醇(PTX)对荷瘤裸鼠具有抗血管生成的作用。杨芳等[9]研究了卡培他滨片不同给药方案对肿瘤血管的影响,结果发现与MTD组[359 mg/(kg·d),连续给药4 d,间断7 d]相比,节拍化疗组[90 mg/(kg·d),连续给药6周]可以使肿瘤微血管密度(MVD)和血管内皮生长因子(VEGF)水平明显下降。
1.2减少TSC数量
TSC对于肿瘤的形成和发展具有自我更新和分化潜能的作用,可引起肿瘤进展,也是目前造成肿瘤细胞耐药的重要原因。Yi SY等[10]对荷肝癌裸鼠模型的研究发现,采用吉西他滨节拍化疗可通过显著降低TSC和活化内皮祖细胞的数量来抑制肿瘤体积增长,起到抗肿瘤作用。Vives M等[11]观察了吉西他滨联合环磷酰胺(CTX)的节拍化疗方案对荷前列腺癌动物模型的抗肿瘤效果,结果发现其肿瘤抑制率达80%,且不增加毒性,分析原因可能与CD133+/CD44+/CD24+TSC和CD133+前体细胞的数量显著减少有关。
1.3调节免疫功能
传统的化疗方式对人体的免疫系统有较大程度的破坏,降低免疫力,从而造成细菌感染或并发其他肿瘤等。节拍化疗可通过免疫刺激,调节机体的免疫力,从而刺激肿瘤细胞的免疫原性。调节性T细胞(Regulatory t cells,Treg)能抑制细胞特异性免疫应答,在肿瘤的进展过程中常伴随Treg数量的增加。因此,如何清除肿瘤组织中的Treg,从而调节患者的免疫系统,是目前抗肿瘤治疗的研究热点。
Brtnický T等[12]研究认为,卵巢癌复发率与Treg在人体外周血中的数量和增长速度密切相关。CTX节拍化疗抗肿瘤的疗效也与Treg数量减少和功能受损等相关[13-14]。另外,节拍化疗能通过树状突细胞(DC)的调节作用,增强肿瘤细胞的免疫原性,提高肿瘤特异性T细胞和γδT细胞毒活性,起到增强抗肿瘤的作用。
1.4诱导肿瘤细胞休眠
肿瘤细胞休眠是肿瘤细胞增殖和凋亡平衡的结果,可能由多种机制所致。节拍化疗可以通过抑制肿瘤新生血管的生成,使得肿瘤细胞无法得到足够的营养从而诱导肿瘤细胞的休眠,但目前尚没有直接的证据支持这一观点。
2 单药节拍化疗
乳腺癌晚期的老年患者对长期放化疗耐受性差,选择单药节拍化疗可减轻患者的不良反应,降低治疗成本,同时持续给药可减缓肿瘤进展速度,延长患者生存期。De Iuliis F等[15]的研究纳入32例转移性乳腺癌老年患者,给予长春瑞滨(VNB)30 mg,po,qod,对其不良反应、生活质量和疾病总缓解率(ORR)进行评估。结果发现,其ORR达50.0%,未发现3~4级不良反应。Addeo R等[16]的研究纳入34例转移性乳腺癌老年患者,在第1、3、5天给予VNB 70 mg/m2,po,连续用3周后停药1周,每4周为1个周期,最多给药12个周期。结果显示,在至少接受3个周期治疗的患者中,完全缓解(CR)2例(占6%),部分缓解(PR)11例(占32%),无疾病进展期(PFS)和平均总生存期(OS)分别为7.7个月和15.9个月,提示口服VNB节拍化疗乳腺癌可作为老年乳腺癌患者新的治疗方法,有较好的临床疗效[16]。Fedele P等[17]的Ⅱ期临床试验纳入60例转移性乳腺癌患者接受卡培他滨(1 500 mg/d)节拍化疗。结果显示,其ORR为62.0%,平均疾病进展期(TTP)和OS分别为7个月和17个月,PR有2例,病情稳定(SD)有7例,未发现3~4级不良反应和血液系统毒性。Park YH等[18]的一项前瞻性、随机、多中心的临床Ⅲ期研究纳入231例接受过6个周期PTX+吉西他滨治疗的晚期转移性乳腺癌患者,随机分为节拍化疗组(n=116)和对照组(n=115)。结果发现,节拍化疗组较对照组的PFS更长(7.5个月vs.3.8个月),OS也更长(32.3个月vs.23.5个月),但3级或以上不良反应中性粒细胞减少症的发生率却更高(61.0%vs.0.9%)。
3 多药节拍化疗
乳腺癌的侵袭性较强,约有5%~10%的患者在初次诊断时就已发生转移,10%~15%的患者在确诊后治疗3年内发现转移病灶[19]。为了提高治疗效果,临床尝试应用多种化疗药物联合给药的节拍化疗或联合生物靶向药物、肿瘤疫苗、环氧化酶(COX)2拮抗药等提高疗效。多药节拍化疗乳腺癌晚期患者的临床试验见表1。
由表1可见,节拍化疗乳腺癌晚期患者的ORR介于44.4%~93.3%,且有利于延长患者生存期。
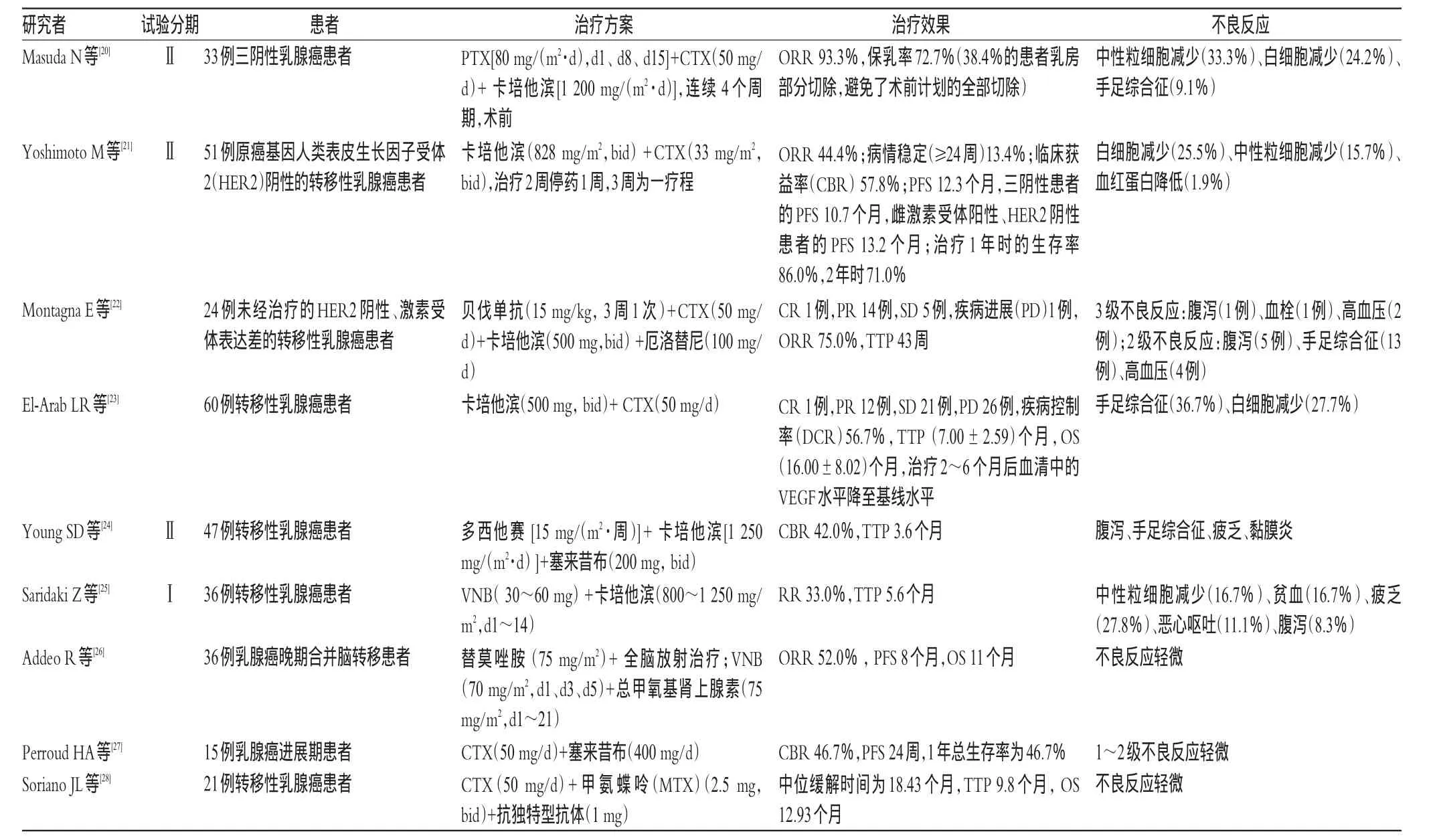
表1 多药节拍化疗乳腺癌晚期患者的临床试验
4 节拍化疗联合内分泌治疗
部分乳腺癌患者疾病的进展受体内性激素水平影响,临床亦采用内分泌治疗,如孕激素、黄体生成素释放激素(LHRH)类似物、抗雌激素类药物和芳香化酶抑制剂。但单独的内分泌治疗也易引起肿瘤细胞耐药,节拍化疗联合内分泌可减轻耐药程度,并提高疗效。
Aurilio G等[29]的研究回顾性分析了33例雌激素受体阳性的乳腺癌患者进行节拍化疗的疗效,节拍化疗药物方案为CTX(50 mg/d)+MTX(2.5 mg,bid,每周一和周四),患者临床缓解率(PR且SD>24个月)达56%(95%置信区间38%~74%),且不良反应较轻。Schwartzberg LS等[30]的一项Ⅱ期临床试验观察了内分泌治疗和抗肿瘤药物节拍化疗对HER2阴性的转移性乳腺癌患者的疗效,分别在每月第1、15、29天给予氟维司琼500、250、250 mg,随后根据患者体质量给予卡培他滨1 500或2 000 mg/d。结果发现,在11个月的治疗周期后,PFS为14.98个月,TTP为26.94个月,OS为28.65个月,患者在化疗期间耐受性良好,大约有<10%的3级不良反应,主要表现为手足综合征、疲劳和恶心等。研究显示,在激素受体阳性的前提下,这一化疗方法具备良好的治疗效果和耐受性。Licchetta A等[31]的一项Ⅱ期临床试验也证实了节拍化疗联合内分泌治疗在转移性乳腺癌中的安全性和抗肿瘤活性。研究纳入的29例患者均接受CTX(50 mg/d,28 d为1个周期,d1~23给药)+醋酸甲地孕酮(80 mg,bid),结果患者的ORR为31.0%,DCR为41.3%,TTP为7.4个月,OS为13.4个月。
5 结语
目前,已开展了多项节拍化疗乳腺癌晚期患者的临床Ⅰ、Ⅱ期研究,且正在进行多项前瞻性Ⅲ期随机临床试验[32-39]。三阴性乳腺癌标准手术治疗后给予卡培他滨节拍化疗的方案可减少患者的复发率和转移率,延长患者生存时间;卡培他滨联合多西他赛常规化疗后,采用卡培他滨进行节拍化疗来治疗转移性乳腺癌的临床研究还在进行中,结果尚未报道。这些临床研究结果将为节拍化疗乳腺癌在临床中的推广提供更多的数据支持。
综上所述,不同的节拍化疗方案有其独有的特点,单药节拍化疗可以减少用药品种,降低化疗费用,但可能会导致疗效降低;多药联合节拍化疗实现了多靶点治疗,可增加疗效,但同时会增加化疗费用和降低患者的顺应性;节拍化疗联合内分泌治疗特别适合激素相关的乳腺癌患者,可通过激素提高节拍化疗的疗效。同时,节拍化疗也存在亟待解决的问题:需要进一步确定适合乳腺癌节拍化疗的患者类型;寻找廉价和疗效显著的节拍化疗的抗肿瘤药物;探索单药或多药联合节拍化疗合理的药物剂量、使用频率和疗程;开发新型缓控释制剂,减少给药频率等。相信随着相关临床研究的不断深入,将会有越来越多的临床数据证实节拍化疗在乳腺癌治疗中的安全性、有效性和经济性[40]。节拍化疗在乳腺癌晚期治疗中具有良好的应用前景,可提高疗效,减少不良反应,延长患者生存期,是乳腺癌晚期治疗的一种新方法。
[1]Kerbel RS.A decade of experience in developing preclinical models of advanced or early-stage spontaneous metastasis to study antiangiogenic drugs,metronomic chemotherapy,and the tumor microenvironment[J].Cancer J,2015,21(4):274.
[2]Di DT,Xu P,Man S,et al.Potent efficacy of metronomic topotecan and pazopanib combination-therapy-in preclinical models of primary or late stage metastatic triplenegative breast cancer[J].Oncotarget,2015,6(40):42 396.
[3]Benzekry S,Hahnfeldt P.Maximum tolerated dose versus metronomic scheduling in the treatment of metastatic cancers[J].J Theor Biol,2013,335(20):235.
[4]Hanahan D,Bergers G,Bergsland E.Less is more,regularly:metronomic dosing of cytotoxic drugs can target tumor angiogenesis in mice[J].J Clin Invest,2000,105(8):1 045.
[5]Norrby K.Metronomic chemotherapy and anti-angiogenesis:can upgraded pre-clinical assays improve clinical trials aimed at controlling tumor growth?[J].Apmis,2014,122(7):565.
[6]Lien K,Georgsdottir S,Sivanathan L,et al.Low-dose metronomic chemotherapy:a systematic literature analysis[J]. Eur J Cancer,2013,49(16):3 387.
[7]Folkman J.Tumor a giogenesis:therapeutic implications[J]. N End J Med,1971,285(21):1 182.
[8]Mannel RS,Brady MF,Kohn EC,et al.A randomized phaseⅢtrial ofⅣcarboplatin and paclitaxel×3 courses followed by observation versus weekly maintenance lowdose paclitaxel in patients with early-stage ovarian carcinoma:a gynecologic oncology group study[J].Gynecol Oncol,2011,122(1):89.
[9]杨芳,张清媛,康欣梅.希罗达对4T1乳腺癌小鼠肿瘤血管生成的影响[J].现代生物医学进展,2007,7(9):1 294.
[10]Yi SY,Ruan J,Zhao L,et al.Metronomic gemcitabine targeted tumor vascular microenvironment decreases the population of CD133+cells in hepatocarcinoma xenografts[J]. Cancer Biomark,2014,14(6):427.
[11]Vives M,Ginestà MM,Gracova K,et al.Metronomic chemotherapy following the maximum tolerated dose is an effective anti-tumour therapy affecting angiogenesis,tumour dissemination and cancer stem cells[J].Int J Cancer,2013,133(10):2 464.
[12]Brtnický T,Fialová A,Laštovička J,et al.Clinical relevance of regulatory T cells monitoring in the peripheral blood of ovarian cancer patients[J].Hum Immunol,2015,76(2/3):187.
[13]Tongu M,Harashima N,Monma H,et al.Metronomic chemotherapy with low-dose cyclophosphamide plus gemcitabine can induce anti-tumor T cell immunity in vivo[J]. Cancer Immunol Immun,2013,62(2):383.
[14]Ge Y,Domschke C,Stoiber N,et al.Metronomic cyclophosphamide treatment in metastasized breast cancer patients:immunological effects and clinical outcome[J]. Cancer Immunol Immun,2012,61(3):353.
[15]De Iuliis F,Salerno G,Taglieri L,et al.On and off metronomic oral vinorelbine in elderly women with advanced breast cancer[J].Tumori,2015,101(1):30.
[16]Addeo R,Sgambato A,Cennamo G,et al.Low-dose metronomic oral administration of vinorelbine in the first-line treatment of elderly patients with metastatic breast cancer [J].Clin Breast Cancer,2010,10(4):301.
[17]Fedele P,Marino A,Orlando L,et al.Efficacy and safety of low-dose metronomic chemotherapy with capecitabine in heavily pretreated patients with metastatic breast cancer [J].Eur J Cancer,2012,48(1):24.
[18]Park YH,Jung KH,Im SA,et al.PhaseⅢ,multicenter,randomized trial of maintenance chemotherapy versus observation in patients with metastatic breast cancer after achieving disease control with six cycles of gemcitabine plus paclitaxel as first-line chemotherapy:KCSG-BR07-02[J].J Clin Oncol,2013,31(14):1 732.
[19]Cardoso F,Loibl S,Pagani O,et al.The European Society of breast cancer specialists recommendations for the management of young women with breast cancer[J].Eur JCancer,2012,48(18):3 355.
[20]Masuda N,Higaki K,Takano T,et al.A phaseⅡstudy of metronomic paclitaxel/cyclophosphamide/capecitabine followed by 5-fluorouracil/epirubicin/cyclophosphamide as preoperative chemotherapy for triple-negative or low hormone receptor expressing/HER2-negative primary breast cancer[J].Cancer Chemother Pharmacol,2014,74(2):229.
[21]Yoshimoto M,Takao S,Hirata M,et al.Metronomic oral combination chemotherapy with capecitabine and cyclophosphamide:a phaseⅡstudy in patients with HER2-negative metastatic breast cancer[J].Cancer Chemother Pharmacol,2012,70(2):331.
[22]Montagna E,Cancello G,Bagnardi V,et al.Metronomic chemotherapy combined with bevacizumab and erlotinib in patients with metastatic HER2-negative breast cancer:clinical and biological activity[J].Clin Breast Cancer,2012,12(3):207.
[23]EL-Arab LR,Swellam M,EL Mahdy MM.Metronomic chemotherapy in metastatic breast cancer:impact on VEGF[J].J Egypt Natl Canc Inst,2012,24(1):15.
[24]Young SD,Lafrenie RM,Clemons MJ.PhaseⅡtrial of a metronomic schedule of docetaxel and capecitabine with concurrent celecoxib in patients with prior anthracycline exposure for metastatic breast cancer[J].Curr Oncol,2012,19(2):e75.
[25]Saridaki Z,Malamos N,Kourakos P,et al.A phaseⅠtrial of oral metronomic vinorelbine plus capecitabine in patients with metastatic breast cancer[J].Cancer Chemother Pharmacol,2012,69(1):35.
[26]Addeo R,Sperlongano P,Montella L,et al.Protracted low dose of oral vinorelbine and temozolomide with wholebrain radiotherapy in the treatment for breast cancer patients with brain metastases[J].Cancer Chemother Pharmacol,2012,70(4):603.
[27]Perroud HA,Rico MJ,Alasino CM,et al.Safety and therapeutic effect of metronomic chemotherapy with cyclophosphamide and celecoxib in advanced breast cancer patients[J].Future Oncol,2013,9(3):451.
[28]Soriano JL,Batista N,Santiesteban E,et al.Metronomic cyclophosphamide and methotrexate chemotherapy combined with 1e10 anti-idiotype vaccine in metastatic breast cancer[J].Int J Breast Cancer,2011,doi:10.4061/2011/ 10292.
[29]Aurilio G,Munzone E,Botteri E,et al.Oral metronomic cyclophosphamide and methotrexate plus fulvestrant in advanced breast cancer patients:a mono-institutional casecohort report[J].Breast J,2012,18(5):470.
[30]Schwartzberg LS,Wang G,Somer BG,et al.PhaseⅡtrial of fulvestrant with metronomic capecitabine for postmenopausal women with hormone receptor-positive,HER2-negative metastatic breast cancer[J].Clin Breast Cancer,2014,14(1):13.
[31]Licchetta A,Correale P,Migali C,et al.Oral metronomic chemo-hormonal-therapy of metastatic breast cancer with cyclophosphamide and megestrol acetate[J].J Chemother,2010,22(3):201.
[32]Di DT,Kerbel RS,Bocci G.Metronomic chemotherapy for triple negative breast cancer?[J].Aging,2016,8(4):573.
[33]Souto M,Shimada A,Chaul C,et al.Low-dose metronomic chemotherapy in metastatic breast cancer:a retrospective analysis of 40 patients[J].J Cancer,2016,doi:10.4236/ jct.2016.77050.
[34]Perroud HA,Alasino CM,Rico MJ,et al.Quality of life in patients with metastatic breast cancer treated with metronomic chemotherapy[J].Future Oncol,2016,12(10):1 233.
[35]Kontani K,Hashimoto S,Murazawa C,et al.Indication of metronomic chemotherapy for metastatic breast cancer:Clinical outcomes and responsive subtypes[J].Mol Clin Oncol,2016,doi:10.3892/mco.2016.841.
[36]Hildebrand JR,Raab RE,Muzaffar M,et al.Neoadjuvant metronomic chemotherapy in triple-negative breast cancer(TNBC)(NCT00542191):updated results from a phaseⅡtrial[J].J Clin Oncol,2016,34(15):e12 502.
[37]Rabizadeh S,Simon B,Klingemann H,et al.Abstract P2-11-12:Novel protocol combining metronomic nant-paclitaxel with HER2-targeted natural killer cells(innate immunotherapy)for HER2-positive metastatic breast cancer [J].Cancer Res,2016,doi:10.1158/1538-7445.SABCS15-P2-11-12.
[38]Perroud HA,Alasino CM,Rico MJ,et al.Abstract P3-07-61:Predictors of response and follow up biomarkers for metronomic chemotherapy with cyclophosphamide and celecoxib in advanced breast cancer patients[J].Cancer Res,2016,doi:10.1158/1538-7445.SABCS15-P3-07-61.
[39]Yang S,Li S,Yu H,et al.Metronomic chemotherapy with 5-fluorouracil and cisplatin for inoperable malignant bowel obstruction because of peritoneal dissemination from gastric cancer[J].Curr Oncol,2016,23(3):248.
[40]Pandey A,Desai A,Ostwal V,et al.Outcome of operable oral cavity cancer and impact of maintenance metronomic chemotherapy:a retrospective study from rural India[J]. South Asian J Cancer,2016,5(2):52.
(编辑:陶婷婷)
R969.4
A
1001-0408(2016)32-4598-04
10.6039/j.issn.1001-0408.2016.32.45
浙江省科技计划项目(No.2015C33286);浙江省中医药科技计划项目(No.2015ZA148、2016ZA038);浙江省医药卫生科技计划项目(No.2014KYB036、2014KYB039)
*副主任药师。研究方向:医院药学。电话:0571-88122120。E-mail:bbbuben@sina.com
(2015-12-10
2016-10-10)
