前交叉韧带部分损伤重建时机对患者术后膝关节功能的影响
2016-03-18王洋白伦浩李彬周秉正
王洋 白伦浩 李彬 周秉正
前交叉韧带部分损伤重建时机对患者术后膝关节功能的影响
王洋 白伦浩 李彬 周秉正
【摘要】目的 探讨关节镜下前交叉韧带部分损伤手术重建的最佳时机。方法 将病例患者根据受伤与手术之间的时间间隔,以 3 周为界限分为早期手术组 ( 32 例) 与延期手术组 ( 45 例),分别采用 IKDC 评分,Lysholm 评分,Tegner 活动率、关节活动度、Kneelax 关节动计度测量仪评价患者手术前后膝关节活动度改变及稳定程度等。结果 两组患者均至少随访 2 年,平均 27 个月。在屈膝 30°、132 N 条件下对同侧膝关节稳定性进行测量:早期手术组 Kneelax 值为 ( 1.0±0.9) mm,延期手术组 Kneelax 值为 ( 2.3±1.5) mm,P<0.01。以上数据说明术后 2 年,早期组患者膝关节前移程度明显小于延期组患者。对于病例中出现的复合伤,早期手术组出现内侧半月板撕裂者 2 例,外侧半月板撕裂者 3 例。延期手术组中,内侧半月板伴有关节软骨损伤者 4 例,外侧半月板伴有关节软骨损伤者 5 例,同时伴有内外侧半月板以及软骨损伤者 5 例,单纯性内侧半月板损伤者 5 例。以上病例证明早期手术患者的伴发损伤明显少于延期组患者 ( P=0.036)。早期手术组和延期手术病例患者膝关节平均移动度分别为 ( 120.6±9.9) °,( 132.4±13.2) ° ( P=0.452)。早期手术组和延期手术组患者 Lysolem 平均分,分别为 ( 94.7±9.3) 分,( 92.2±7.8) 分 ( P=0.332),两组病例患者 Tegner 平均分为 ( 7.1±1.2) 分,( 6.3±1.8) 分 ( P=0.935)。IKDC 评估中,早期手术组 32 例中 30 例 ( 93.75%) 被认为正常或接近正常,延期手术组 45 例中 43 例 ( 95.56%) 被认为正常或接近正常 ( P=0.976)。以上四种评估方法认为两组病例无统计学意义 ( P>0.05)。结论 前交叉韧带部分损伤的早期手术重建能很好地恢复膝关节的稳定性,不会导致膝关节的粘连,而且能够防止前交叉韧带的再次松弛,降低半月板和关节软骨的伴发损伤。
【关键词】半月板,胫骨;前交叉韧带重建;关节镜检查;医院,康复
前交叉韧带包括两个主要的部分:前内侧束和后外侧束[1-2]。当膝关节屈曲时,前内侧束紧张,当膝关节伸直时,后外侧束紧张[2]。二者共同保持膝关节的前向稳定性。传统观念认为,对于单纯的前交叉韧带部分损伤进行保守治疗是可行的,并且预后良好[3-5]。然而,一些学者认为,前交叉韧带部分撕裂会因为相关血管的破坏而逐步发展为剩余韧带的坏死、断裂[6-9]。此外,前交叉韧带的双束韧带解剖学重建相对于单束韧带的重建在临床上更常用于保持膝关节的旋转稳定性[10-11]。因此,一些学者认为,大多数前交叉韧带部分撕裂的患者,尤其是有更多运动需求的患者,需要立即进行前交叉韧带重建手术[12-14]。有的学者认为,膝关节韧带重建手术宜在损伤后 3 周内进行,此时损伤结构辨认清晰,手术简单。手术越早,解剖结构辨认越清楚,越容易修补。超过 3 周以后,损伤的解剖层次不清,组织脆弱,难以缝合[15]。因此,本研究以 3 周为界限,将患者分为早期手术组 ( 32 例) 与延期手术组 ( 45 例)。然而,何时对前交叉韧带部分损伤的患者进行关节镜重建手术,目前仍没有一个明确的定论。
2009 年至 2012 年,我科室共经治 77 例单侧前交叉韧带部分断裂的患者,现总结分析如下。关节镜下前交叉韧带重建手术防止整条韧带的再次松弛,减少半月板以及关节软骨的远期伴发损伤,且不导致关节粘连。
资料与方法
一、一般资料
本组 77 例均为膝关节外伤,伴有轻度或中度膝关节肿胀以及疼痛。本组 77 例包括前内侧束前交叉韧带损伤 56 例,后外侧束前交叉韧带损伤 21 例。其中男 51 例,女 26 例。22 例左膝,55 例右膝,平均年龄 26.5 ( 年龄 17~49) 岁。受伤与手术间隔为 1 周到 12 个月不等。本组 77 例中,32 例在伤后3 周内手术 ( 早期手术组),其余 45 例为延期手术( 延期手术组)。
本组 77 例术前因受膝关节不稳影响,均无伤前膝关节活动水平。前交叉韧带部分断裂的诊断根据为:Lachman 征或者前抽屉试验阳性[16],伴或不伴有轴移试验阳性[17],Kneelax 动计度测量仪器检查胫骨上端前向活动异常[18]。这些查体与辅助检查结果均与健侧进行对比,以判断有无前交叉韧带松弛。磁共振显示:韧带可见异常信号,韧带局部弥漫性肿胀、增粗,边缘不清或韧带变细,但连续性尚存在,部分韧带纤维弯曲或成波浪状[19]。
二、手术方法
手术全部由一名高年资医师全程完成。两组患者均采用平卧位,麻醉成功后,通过膝关前外侧以及前内侧入路,关节镜下对患者进行诊断性的探查,前交叉韧带是否部分损伤可通过镜下得以确认,残余的韧带纤维数量以及质量可通过探钩牵拉和前抽屉试验来评估。膝关节前内侧束损伤时前抽屉试验采用膝关节屈曲 20° 体位检查后外侧束状态,后外侧束损伤时前抽屉试验采用膝关节屈曲 70°体位检查前内侧束是否完整、松弛。
所有相关解剖结构,经镜下检查确认有无半月板和软骨损伤。半月板损伤者行半月板部分切除成形术治疗,关节软骨损伤者行软骨清理术治疗。清理破坏的滑膜,韧带残端需保留。术中需谨慎保护好前交叉韧带前内侧束以及后外侧束。
妥善剥离并取出半腱肌,用一号可吸收线交织缝合取出的半腱肌两头 3 cm 位置,沿着取半腱肌的切口,用导针定位,在内侧入路位置插入导架,定位于前交叉韧带的前内侧束或后外侧束胫骨着点,打通一直径为 6~7 mm 通道。建立股骨隧道,前内侧入路置入股骨前交叉韧带胫骨导向器,暴露股骨髁间窝外侧后壁,清理髁间窝,隧道中心定位在前交叉韧带前内侧束和后外侧束股骨止点交界偏后处,制作匹配移植物直径的骨道。把准备好的韧带置入隧道中。带襻钢板固定韧带于股骨端,胫骨端固定一可吸收门钉。
三、术后康复
术后所有患者,均在专业康复师的指导下,进行早期物理治疗和康复训练。术后康复训练的好坏是影响关节功能的一个很重要的因素,早期的康复训练是为了使关节在获得良好稳定性的基础上,尽早恢复正常活动,遵循循序渐进、从弱到强、灵活机动、不疲劳能耐受为原则[20]。直腿抬高以及主动屈膝训练在术后第 2 天进行。术后第 3 天,患者在患肢伸直位置佩戴好支具,可利用拐杖的帮助在患肢不负重情况下开始下地行走。术后 1 周,患肢主动屈曲可达 90°。术后 6 周,患者可佩戴支具下完全负重行走,屈膝角度同常人。所有患者均在术后6 个月内完全康复,可进行正常的日常生活工作。
四、观察指标与判定方法
两组患者分别在术后 24 个月内进行 Lysolem 评分,IKDC 评分,Tegner 评分,关节活动度,Kneelax关节动计度测量仪测量,以上数据均由同一个未参与患者治疗的医师测量。
五、统计学分析
所有数据经整理后应用 SPSS 17.0 软件进行分析。两组数据应用非配对 t 检验进行连续性的检验,计数资料应用 χ2检验,计量资料应用 Wilcoxon检验。P<0.05 认为差异有统计学意义。
结 果
早期手术组 25 例,延期手术组 31 例,有前内侧束韧带损伤,早期手术组 10 例,延期手术组11 例,有后外侧束韧带损伤。早期手术组,内侧半月板撕裂者 2 例,外侧半月板撕裂者 3 例。延期手术组,19 例出现不同程度合并的复合伤。内侧半月板和关节软骨损伤者 4 例,外侧半月板损伤伴有关节软骨损伤者 5 例,内外侧半月板及关节软骨损伤者 5 例,单纯内侧半月板损伤者 5 例。这些病例证明早期手术患者的伴发损伤明显少于延期手术患者 ( P=0.036) ( 表 1,2),同侧膝关节稳定性测量的平均值 ( 屈膝 30° 和 132 N) 为早期手术组 ( 1.0±0.9) mm,延期手术组为 ( 2.3±15) mm,P<0.01。以上数据说明术后 2 年,早期组患者关节前移程度明显小于延期组患者。
术后膝关节平均移动度:早期手术组、延期手术组,分别为 ( 120.6±9.9) °,( 132.4±13.2) °,差异无统计学意义 ( P=0.452)。Lysolem 评分:早期手术组、延期手术组分别为 ( 94.7±9.3) 分,( 92.2±7.8) 分 ( P=0.332),Tegner 评分:早期手术组、延期手术组分别为 ( 7.1±1.2) 分,( 6.3±1.8) 分( P=0.935)。IKDC 评估:早期手术组 32 例中 30 例( 93.75%) 以及延期手术组 45 例中 43 例 ( 95.56%)被视为正常或接近正常 ( P=0.976)。两组差异无统计学意义 ( P>0.05)。两组均无须再次手术的术后即发并发症。
表1 两组患者术前情况比较 (±s)Tab.1 A comparison of patients preoperatively in 2 groups (±s)
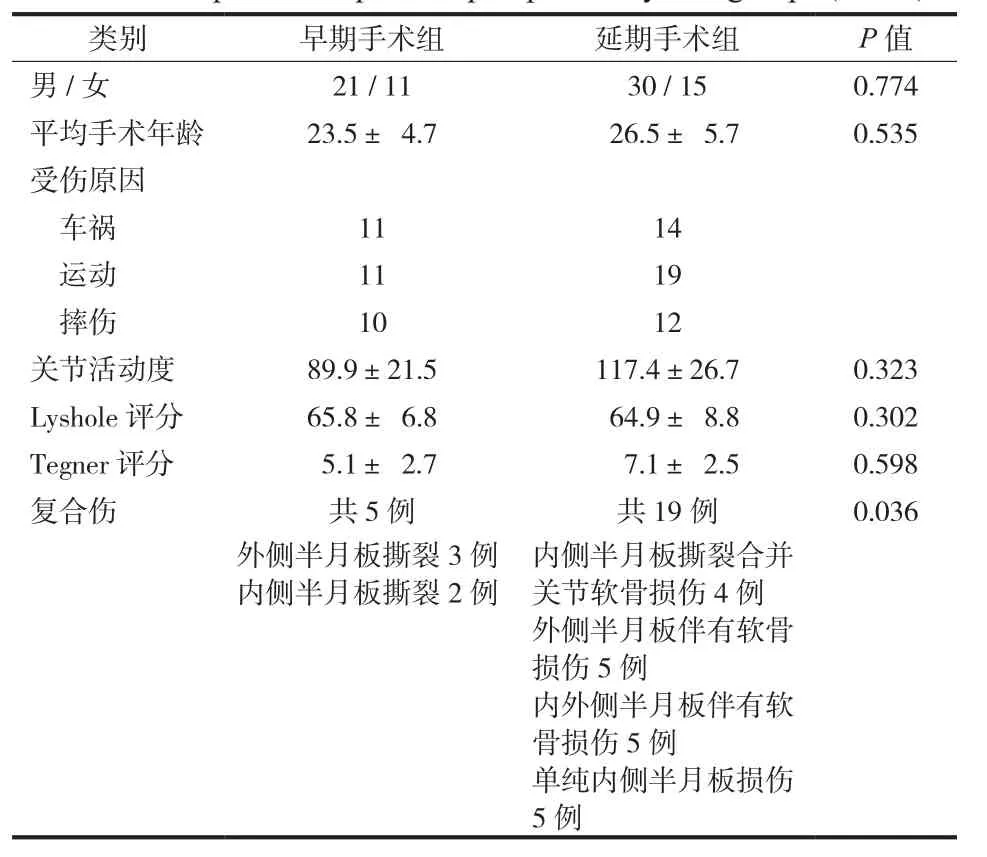
表1 两组患者术前情况比较 (±s)Tab.1 A comparison of patients preoperatively in 2 groups (±s)
类别 早期手术组 延期手术组 P 值男 / 女 21 / 11 30 / 15 0.774平均手术年龄 23.5±4.7 26.5±5.7 0.535受伤原因车祸 11 14运动 11 19摔伤 10 12关节活动度 89.9±21.5 117.4±26.7 0.323 Lyshole 评分 65.8±6.8 64.9±8.8 0.302 Tegner 评分 5.1±2.7 7.1±2.5 0.598复合伤 共 5 例 共 19 例 0.036外侧半月板撕裂 3 例内侧半月板撕裂 2 例内侧半月板撕裂合并关节软骨损伤 4 例外侧半月板伴有软骨损伤 5 例内外侧半月板伴有软骨损伤 5 例单纯内侧半月板损伤5 例
表2 两组患者术后比较 (? ±s)Tab.2 Postoperative changes in both groups (±s)
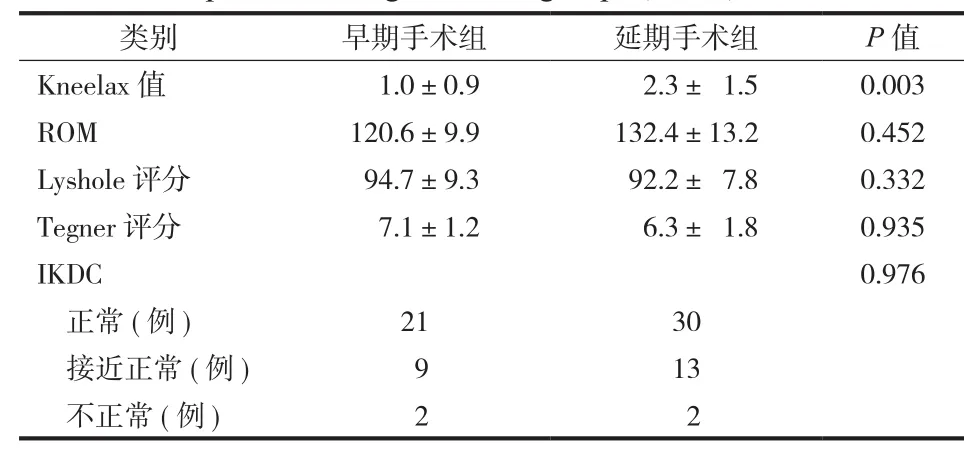
表2 两组患者术后比较 (? ±s)Tab.2 Postoperative changes in both groups (±s)
类别 早期手术组 延期手术组 P 值Kneelax 值 1.0±0.9 2.3±1.5 0.003 ROM 120.6±9.9 132.4±13.2 0.452 Lyshole 评分 94.7±9.3 92.2±7.8 0.332 Tegner 评分 7.1±1.2 6.3±1.8 0.935 IKDC 0.976正常 ( 例) 21 30接近正常 ( 例) 9 13不正常 ( 例) 2 2
讨 论
Shelbourne 等[21]回顾性的研究了 169 例前交叉韧带损伤病例,研究发现早期前交叉韧带重建手术的患者,尤其是伤后 1 周内进行手术者有更高的几率形成关节粘连。
Mayl 等[22]回顾了 156 例前交叉韧带重建术后发生关节粘连的病例,发现膝关节纤维化的进展与患膝出现炎症、肿胀的症状密切相关。Duquin 等[23]报告 993 例的调查结果,认为膝关节活动度以及膝关节肿胀的程度是前交叉韧带重建手术时机选择的重要标准。
笔者用 Kneelax 测量仪对膝关节进行稳定度测量后认为:伤后与手术前这段时间里,部分损伤的前交叉韧带束被拉长,整束前交叉韧带趋向于松弛。这与之前的 3 项研究报告结果相似[6,8,24]。Danychuk 等发现,前交叉韧带部分损伤进展成为完全性断裂的原因可能是相关血管的中断以及坏死导致。笔者认为,前交叉韧带单束损伤后,为了维持膝关节的稳定性,另一束需要承受更多的应力作用,从而逐渐引起这一束韧带纤维的松弛。重建手术越早进行,这束韧带受到的异常应力作用越少,则松弛的可能性越低。
有学者对完全性前交叉韧带损伤重建的手术时间与发生半月板和关节软骨损伤的概率进行了研究。Kennedy 等[25]报告称延期手术能明显增加相关伴发损伤发生的风险。Granan 等[26]认为,成年人膝关节软骨损伤患者,从受伤到手术,每延迟 1 个月,其软骨损伤的几率就增加 1%,而如果伴有半月板损伤,其软骨损伤的几率翻倍,反之亦然。Papastergiou 等[27]提出,前交叉韧带重建手术需在伤后 3 个月内进行,以最大程度上降低伴发损伤的风险。本组病例的随访时间显短。尽管早期手术组复合伤明显少于延期手术组,但术后 2 年膝关节功能的评估 ( 包括 Lysolem 评分,IKDC 评分,Tegner 评分) 结果,显示两组并无明显差异。因此对两组病例更长时间的随访,以评估膝关节功能以及相关损伤的发生是非常必要的。
本研究结果提示对前交叉韧带部分损伤的患者,早期手术重建可有益于保护前交叉韧带和半月板,并且手术不会导致膝关节发生粘连。
参 考 文 献
[1] Zantop T, Petersen W, Sekiya JK, et al. Anterior cruciate ligament anatomy and function relating to anatomical reconstruction. Knee Surg Sports Traumatol Arthrosc, 2006, 14(10):982-992.
[2] Amis AA, Dawkins GP. Functional anatomy of the anterior cruciate ligament. Fibre bundle actions related to ligament replacements and injuries. J Bone Joint Surg Br, 1991, 73(2): 260-267.
[3] Kannus P, Järvinen M. Conservatively treated tears of the anterior cruciate ligament.Long-term results. J Bone Joint Surg Am, 1987, 69(7):1007-1012.
[4] Odensten M, Lysholm J, Gillquist J. The course of partial anterior cruciate ligament ruptures. Am J Sports Med, 1985, 13(3):183-186.
[5] Sommerlath K, Odensten M, Lysholm J. The late course of acute partial anterior cruciate ligament tears. A nine to 15-year follow-up evaluation. Clin Orthop Relat Res, 1992, (281): 152-158.
[6] Noyes FR, Mooar LA, Moorman CT 3rd, et al. Partial tears of the anterior cruciate ligament. Progression to complete ligament defcien-cydeficiency. J Bone Joint Surg Br, 1989, 71(5): 825-833.
[7] Fruensgaard S, Johannsen HV. Incomplete ruptures of the anterior cruciate ligament. J Bone Joint Surg Br, 1989, 71(3): 526-530.
[8] Fritschy D, Panoussopoulos A, Wallensten R, et al. Can we predict the outcome of a partial rupture of the anterior cruciate ligament? A prospective study of 43 cases. Knee Surg Sports Traumatol Arthrosc, 1997, 5(1):2-5.
[9] Danylchuk KD, Finlay JB, Krcek JP. Microstructural organization of human and bovine cruciate ligaments. Clin Orthop Relat Res, 1978, (131):294-298.
[10] Yagi M, Wong EK, Kanamori A, et al. Biomechanical analysis of an anatomic anterior cruciate ligament reconstruction. Am J Sports Med, 2002, 30(5):660-666.
[11] Yasuda K, Kondo E, Ichiyama H, et al. Clinical evaluation of anatomic double-bundle anterior cruciate ligament reconstruction procedure using hamstring tendon grafts: comparisons among 3 different procedures. Arthroscopy, 2006, 22(3):240-251.
[12] Serrano-Fernandez JM, Espejo-Baena A, Martin-Castilla B, et al. Augmentation technique for partial ACL ruptures using semitendinosus tendon in the over-the-top position. Knee Surg Sports Traumatol Arthrosc, 2010, 18(9):1214-1218.
[13] Sonnery-Cottet B, Lavoie F, Ogassawara R, et al. Selective anteromedial bundle reconstruction in partial ACL tears:a series of 36 patients with mean 24 months follow-up. Knee Surg Sports Traumatol Arthrosc, 2010, 18(1):47-51.
[14] Buda R, Ferruzzi A, Vannini F, et al. Augmentation technique with semitendinosus and gracilis tendons in chronic partial lesions of the ACL: clinical and arthrometric analysis. Knee Surg Sports Traumatol Arthrosc, 2006, 14(11):1101-1107.
[15] 孙康, 徐强, 王杰峰. 急性与慢性前交叉韧带合并膝关节后外角损伤. 中国矫形外科杂志, 2004, 12(3、4):297-298.
[16] Furman W, Marshall JL, Girgis FG. The anterior cruciate ligament: A functional analysis based on postmortem studies. J Bone Joint Surg Am, 1976, 58(2):179-185.
[17] Barrack RL, Buckley SL, Bruckner JD, et al. Partial versus complete acute anterior cruciate ligament tears. The results of nonoperative treatment. J Bone Joint Surg Br, 1990, 72(4): 622-624.
[18] Bach BR Jr, Warren RF, Flynn WM, et al. Arthrometric evaluation of knees that have a torn anterior cruciate ligament. J Bone Joint Surg Am, 1990, 72(9):1299-1306.
[19] 傅强, 杨柳. MRI诊断膝关节前交叉韧带损伤的研究进展. 第四军医大学学报, 2007, 28(12):1150-1152.
[20] 方菊飞, 余宁先, 卢春秀, 等. 膝关节镜下自体髌韧带移植重建前交叉韧带的康复训练. 护理实践与研究, 2012, 9(5): 35-36.
[21] Shelbourne KD, Wilckens JH, Mollabashy A, et al. Arthrofibrosis in acute anterior cruciate ligament reconstruction. The effect of timing of reconstruction and rehabilitation. Am J Sports Med, 1991, 19(4):332-336.
[22] Mayr HO, Weig TG, Plitz W. Arthrofbrosis following ACL reconstruction--reasons and outcomes. Arch Orthop Trauma Surg, 2004, 124(8):518-522
[23] Duquin TR, Wind WM, Fineberg MS, et al. Current trends in anterior cruciate ligament reconstruction. J Knee Surg, 2009, 22(1):7-12.
[24] Shelbourne KD, Patel DV. Timing of surgery in anterior cruciate ligament-injured knees. Knee Surg Sports Traumatol Arthrosc, 1995, 3(3):148-156.
[25] Kennedy J, Jackson MP, O’Kelly P, et al. Timing of reconstruction of the anterior cruciate ligament in athletes and the incidence of secondary pathology within the knee. J Bone Joint Surg Br, 2010, 92(3):362-366.
[26] Granan LP, Bahr R, Lie SA, et al. Timing of anterior cruciate ligament reconstructive surgery and risk of cartilage lesions and meniscal tears: a cohort study based on the Norwegian National Knee Ligament Registry. Am J Sports Med, 2009, 37(5): 955-961.
[27] Papastergiou SG, Koukoulias NE, Mikalef P, et al. Meniscal tears in the ACL-deficient knee: correlation between meniscal tears and the timing of ACL reconstruction. Knee Surg Sports Traumatol Arthrosc, 2007, 15(12):1438-1444.
( 本文编辑:李贵存)
. 作者须知 Instruction for authors .
Optimal reconstruction timing of partially injured anterior cruciate ligaments on postoperative knee functions WANG Yang, BAI Lun-hao, LI Bin, ZHOU Bing-zheng. Department of Joint and Sports Medicine, Shengjing Hospital, China Medical University, Shenyang, Liaoning, 110000, PRC
【Abstract】Objective To explore the optimal timing for arthroscopic surgery of partially injured anterior cruciate ligaments ( ACL). Methods Cases were classified based on the time interval between injury and surgery: early surgery group ( < 3 weeks, n = 32), delayed surgery group ( > 3 weeks, n = 45). International Knee Documentation Committee ( IKDC) score, Lysholm knee score, Tegner activity rating, knee range of motion ( ROM), and Kneelax arthrometer were applied to measure the changes of ROM and stability before and after surgery. Results Minimum follow-up was 2 years, average of 27 months. Knee stability assessed by Kneelax arthrometer ( 30° flexion and 132 N): ( 1.0 ±0.9) mm in early surgery group and ( 2.3 ±1.5) mm in delayed surgery group ( P < 0.01). The stability results indicated that patients in the early surgery group had significantly less anterior displacement than patients in the delayed surgery group 2 years postoperatively. With regard to associated injuries, 2 patients had medial meniscus rupture and 3 had lateral meniscus rupture in the early surgery group. While in the delayed surgery group: 4 patients had medial meniscus rupture and cartilage injury, 5 had lateral meniscus rupture and cartilage injury, 5 had medial and lateral meniscus rupture and cartilage injury, 5 had simple medial meniscus rupture. It demonstrated that associated injuries in early surgery patients were significantly fewer than in the delayed surgery group ( P = 0.036). The mean range of motion were ( 120.6 ±9.9) ° and ( 132.4 ±13.2) ° ( P = 0.452), mean Lysholm scores ( 94.7 ±9.3) point and ( 92.2 ±7.8) point ( P = 0.332), mean Tegner scores ( 7.1 ±1.2) point and ( 6.3 ±1.8) point ( P = 0.935)book=141,ebook=66in the early and delayed surgery group. In terms of the IKDC evaluation system, 30 out of 32 ( 93.75%) patients in the early surgery group and 43 out of 45 ( 95.56%) patients in the delayed surgery group were graded as normal or nearly normal ( P = 0.976). No statistical significance existed between the 2 groups with respect to the 4 types of assessment results ( P > 0.05). Conclusions Early surgical reconstruction of partially ruptured ACLs will not result in arthrofbrosis but may prevent secondary loosening of the intact bundles and further meniscal and chondral injury.
【Key words】Menisci, tibia; Anterior cruciate ligament reconstruction; Arthroscopy; Hospitals, convalescent
( 收稿日期:2015-07-28)
Corresponding author:BAI Lun-hao, Email: bailh@sj-hospital.org
通信作者:白伦浩,Email: bailh@sj-hospital.org
DOI:10.3969/j.issn.2095-252X.2016.02.014
作者单位:110000 沈阳,中国医科大学附属盛京医院关节运动病房
中图分类号:R684
