Prostate-specific antigen doubling time and response to cabazitaxel in a hormone-resistant metastatic prostate cancer patient
2015-02-14MarwanGhosnAlainDagherFadiElKarak
Marwan Ghosn,Alain Dagher,Fadi El-Karak
Prostate-specific antigen doubling time and response to cabazitaxel in a hormone-resistant metastatic prostate cancer patient
Marwan Ghosn✉,Alain Dagher,Fadi El-Karak
Hematology-Oncology Department,Faculty of Medicine,Saint-Joseph University,Beirut,Lebanon.
We report a case of metastatic castration-resistant prostate cancer,who received prior treatment with docetaxel and was then given cabazitaxel as salvage therapy.The patient was monitored by prostate-specific antigen doubling time and prostate-specific antigen absolute value.The prostate-specific antigen doubling time was found to be a good response predictor in the patient.
prostate-specific antigen,doubling time,prostate cancer,cabazitaxel,docetaxel
Introduction
Cabazitaxel is a novel taxane and an effective second-line agent in patients with metastatic castration-resistant prostate cancer(mCRPC)refractory to a docetaxelcontaining regimen.Here,we report a patient with mCRPC who received prior treatment with docetaxel and was then given cabazitaxel as salvage therapy. Treatment response was monitored by prostate-specific antigen(PSA)doubling time and PSA absolute value.
Case report
A 68-year-old male was initially diagnosed with prostate adenocarcinom a in January 2005.He underwent radical prostatectomy.The patienthad grade 5 adenocarcinoma with a Gleason score of 7(4+3).The tumor occupied both lobes and reached the apical margin.The right seminal vesicle,apex and bladder neck margins were negative for malignancy.The postoperative PSA reached the nadir(0.05 ng/mL)in April 2005.Eight months later, the PSA increased to 1.03 ng/mL,and the patient received salvage external beam radiation concurrently with bicalutamide from February 16 to April 5,2006, followed by treatment with adjuvant luteinizing hormone releasing hormone(LHRH)agonists.
In September 2009,the patient relapsed with bone metastasis at the right acetabulum(PSA:5.9 ng/mL). He received 10 sessions of radiation therapy and was started on monthly zoledronic acid.In March 2010, his PSA level increased to 7.5 ng/mL(Fig.1)and radiologic evaluation showed a stable bone defect affecting the right side of L4 vertebral body,with a soft tissue mass exhibiting mild increased uptake,but there were no signs suggesting local recurrence in the prostatic bed.He received 4 cycles of docetaxel while continuing the LHRH inhibitor.
Two comparative PET-CT scans performed in July 2010 and February 2011 showed a stable disease on the bone despite an increase of PSA of 26 ng/mL(doubling in 2 months).The patient continued his treatmentwith LHRH agonists and zoledronic acid.In April 2011,the PSA level increased to 150 ng/mL.The patient started his treatment with cabazitaxel at a dose of 25 mg/m2for every 21 days.In June 2011 and after receiving 3 cycles,his PSA level increased to 213 ng/mL.Despite that the patient continued to receive the same treatment,his PSA level reached 288 n g/mL in January 2012.In M arch 2012,the patient developed a symptomatic pulmonary embolism and had dyspnea.During this period,the patient was clinically stable,all the staging radiologic tests showed no signs of major recurrence at the prostatic bed and the metastatic sites.A fter resolution of pulmonary embolism,the patient continued the same treatment with cabazitaxel at the same schedule with no delays or interrup tions.In M ay 2012,when 15 injections of cabazitaxel(750 mg)were performed,the first decline was observed in PSA level(245 ng/mL).
In October 2012,the patient decided to stop the treatment after a total of 21 cycles and a cumulative dose of 1,050 mg.Generally,he tolerated the therapy well.He was given growth factors prophylactically and did not experience any fever or neutropenia.He gained weight and his performance status was improved.
D iscussion
In 2010,the U.S.Food and Drug Administration (FDA)approved cabazitaxel for use in combination with prednisone for treatment of patients with mHRPC previously treated with a docetaxel-containing regimen.Based on data from the TROPIC trial,cabazitaxel should only be considered in patients,who previously received a cumulative docetaxel dose of at least 225 mg/m2[1].Our patient had previously received a cumulative dose of docetaxel of 350 mg/m2and was given cabazitaxel as a salvage therapy.Clinical and radio logic evaluation demonstrated clinical benefit even though PSA level increased.This counterintuitive situation led to an impression that the treatment was not effective.Indeed,after the 4thcycle of cabazitaxel, the PSA doubling time started to slow and was considered a"positive indicator of response".The 1stdecline in the absolute PSA value was noticed after the15thcycle,which was maintained through a long period of prolonged PSA doubling(Fig.1).
The literatures are conflicting about the usefulness of PSA velocity or doubling time as predictors of disease progression.Some studies showed little evidence that calculation of PSA velocity or doubling time provides predictive information beyond that provided by absolute PSA level alone[2-5].Moreover,the use of PSA dynamics is not supported by current clinical evidence[3-4].However,PSA kinetics has been established as useful indicators for prognosis and survival in different clinical settings,mainly in intermediate-and high-risk patients.For instance,a high pre-therapy PSA velocity is associated with a greater risk of death from prostate cancer after surgery or radiation therapy[7].Similarly,PSA doubling time with PSA recurrence after definitive local therapy is able to identify patients at high risk of prostate cancer specific mortality[7].
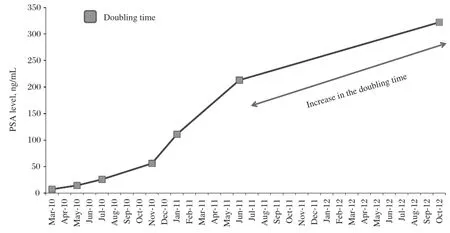
Fig.1 PSA levels and doubling time in a 68-year-old male with metastatic castration resistant prostate cancer.PSA:prostate-specific antigen.
In some active surveillance studies,a high PSA velocity will inevitably lead to a high PSA and progression[2,6-8].Other studies reported that the PSA doubling time was performed in the pretreatment prognostic factors to predict survival outcomes,and can be used as an independent factor for overall prostate cancer management and guidance for treatment strategies,including appropriate timing of chemotherapy[9].In conclusion, second-line chemotherapy options for mCRPC were limited until the recent approval of cabazitaxel.Even with significant prior treatment with docetaxel,responses to cabazitaxel are seen in the setting of aggressive and advanced mCRPC.The response assessment is based on clinical status,radiologic findings and PSA levels. Our experience with cabazitaxel in this case illustrates the eventual role of PSA doubling time as an early predictive factor of response.
[1] de Bono JS,Oudard S,Ozguroglu M,et al.TROPIC Investigators.Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment:a randomised open-label trial[J]. Lancet,2010,376(9747):1147-1154.
[2] Vickers AJ,Savage C,O’Brien MF,et al.Systematic review of pretreatment prostate-specific antigen velocity and doubling time as predictors for prostate cancer[J]. J Clin Oncol,2009,27(3):398-403.
[3] O’Brien MF,Cronin AM,Fearn PA,et al.Pretreatment prostate-specific antigen(PSA)velocity and doubling time are associated with outcome but neither improves prediction of outcome beyond pretreatment PSA alone in patients treated with radical prostatectomy[J].J Clin Oncol,2009,27(22):3591-3597.
[4] Ulmert D,Serio AM,O’Brien MF,et al.Long-term prediction of prostate cancer:PSA velocity is predictive but does not improve the predictive accuracy of a single PSA measurement 15 years or more before cancer diagnosis in a large,representative,unscreened population[J]. J Clin Oncol,2008,26(6):835-841.
[5] Thomsen FB,Christensen IJ,Brasso K,et al.Prostate-specific antigen doubling time as a progression criterion in an active surveillance programme for patients with localised prostate cancer[J].BJU Int,2014,113(5b):E98-105.
[6] Sengupta S,Myers RP,Slezak JM,et al.Preoperative prostate specific antigen doubling time and velocity are strong and independent predictors of outcomes following radical prostatectomy[J].J Urol,2005,174(6):2191-2196.
[7] D’Am ico AV,Chen MH,Roehl KA,et al.Preoperative PSA velocity and the risk of death from prostate cancer after radical prostatectomy[J].N Engl J Med,2004,351(2): 125-135.
[8] Khatam i A,Aus G,Damber JE,et al.PSA doubling time predicts the outcome after active surveillance in screening-detected prostate cancer:Results from the European randomized study of screening for prostate cancer,Sweden section[J].Int J Cancer,2007,120(1):170-174.
[9] Elshafei A,Li YH,Hatem A,et al.The utility of PSA velocity in prediction of prostate cancer and high grade cancer after an initially negative prostate biopsy[J].Prostate, 2013,73:1796-1802.
✉Corresponding author:Marwan Ghosn,MD,MHHM,Hematology-Oncology Department,Faculty of Medicine,Saint-Joseph University, Beirut,Lebanon,894 Blvd Alfred Naccache,Bldg Sehanoui,5thFloor, POBox:166830,Beirut,Lebanon.Tel/Fax:+961-1-613395;+961-3-226842/+961-1-613397,E-mail:mghosn.hd f@usj.edu.lb.
Received 29 September 2013,Revised 06 January 2014,Accepted 23 February 2014,Epub 30 March 2014
R737.25,Document code:B
The authors reported no conflict of interests.
©2015 by the Journal of Biomedical Research.All rights reserved.
10.7555/JBR.28.20130148
杂志排行

THE JOURNAL OF BIOMEDICAL RESEARCH的其它文章
- Internal radiation therapy:a neglected aspect of nuclear medicine in the molecular era
- Hypercholesterolemia,low density lipoprotein receptor and proprotein convertase subtilisin/kexin-type 9
- Endothelin-1-induced mini-stroke in the dorsal hippocampus or lateral amygdala results in deficits in learning and memory
- Netrin-1 overexpression in bone marrow mesenchymal stem cells promotes functional recovery in a rat model of peripheral nerve injury
- Acute effect of aspartame-induced oxidative stress in Wistar albino rat brain
- Differential mRNA expression profiling of oral squamous cell carcinoma by high-throughput RNA sequencing