椎体压缩性骨折四种影像学诊断的一致性研究
2014-02-14孙金磊付亚东王延林金玉莲李葆青
张 祥 孙金磊 付亚东 王延林 金玉莲 梁 洁 李葆青
. 骨科影像学 Orthopaedic radiology .
椎体压缩性骨折四种影像学诊断的一致性研究
张 祥 孙金磊 付亚东 王延林 金玉莲 梁 洁 李葆青
目的对比分析 MRI、CT 侧位定位像、CT 重建图像和 X 线平片诊断椎体压缩性骨折的一致性。方法回顾性分析 2014 年 1 月 1 日至 2014 年 4 月 30 日,我院同时行胸椎或腰椎 MRI 和 CT 检查的患者 50 例 ( 398 个椎体 ),以及同时行 MRI 和 X 线平片检查的患者 70 例 ( 480 个椎体 ),覆盖 T4~L5椎体范围,运用半定量分级方法,按椎体压缩程度分为 0~3 级,分别统计 MRI-CT 组和 MRI-X 线平片组中 MRI、CT 侧位定位像、CT 重建图像、X 线平片的各级椎体的个数,采用 kappa 分析得到 MRI 与 CT 侧位定位像、CT 重建图像诊断压缩性骨折 ≥1 级和 ≥2 级的椎体的一致性,然后分析 MRI 与 X 线平片诊断压缩性骨折 ≥1 级和 ≥2 级的椎体的一致性;两组分别以 MRI 为标准,0 级为阴性结果,≥1 级为阳性结果,计算侧位 CT 定位像、CT 重建图像和 X 线平片诊断椎体压缩性骨折的敏感性和特异性。结果MRI 与 CT 侧位定位像诊断≥1 级椎体有中等程度的一致性 ( k=0.583 ),诊断 ≥2 级椎体有好的一致性 ( k=0.818 );MRI 与 CT 重建图像诊断 ≥1 级和 ≥2 级椎体均有好的一致性 ( k=0.836 和 0.961 );MRI 与 X 线平片诊断 ≥1 级椎体有中等程度一致性 ( k=0.651 ),诊断 ≥2 级椎体有好的一致性 ( k=0.862 );MRI-CT 组中 CT 侧位定位像诊断椎体压缩性骨折的敏感性和特异性分别为 55.2% 和 97.1%,CT 重建图像诊断的敏感性和特异性分别为 81.6% 和 98.5%;MRI-X 线平片组中 X 线平片诊断椎体压缩性骨折的敏感性和特异性分别为 62.5% 和 96.7%。结论MRI 和 CT重建图像诊断椎体骨折的一致性最高;相对 MRI,CT 重建图像诊断椎体压缩性骨折的敏感性和特异性均较高,而 CT 侧位定位像和 X 线平片的特异性较高,敏感性较低。
骨折,压缩性;磁共振成像;体层摄影术,X 线;体层摄影术,X 线计算机
椎体压缩性骨折是临床上引起腰背部疼痛的常见原因之一,以胸腰椎最为多见。其常由外伤、骨质疏松等因素造成[1-6]。影像检查是诊断该病的主要手段,X 线平片、CT 和 MRI 均可用于椎体压缩性骨折的诊断,其中 X 线平片是临床首选的检查手段;而 MRI 由于具有多参数、多层面、多方向成像的特点,一直被认为是诊断椎体压缩性骨折最可靠的影像学检查方法[1-4];MRI、CT 侧位定位像对诊断椎体压缩性骨折也有一定的价值[2,5-6],CT 扫描对显示骨细微结构和通过三维重组技术对骨折的发现和分级,均有十分重要的价值[4-8]。本研究通过回顾性分析行 X 线平片、CT、MRI 检查的椎体压缩性骨折的病例,以 MRI 检查为诊断的标准,运用半定量分级的方法比较分析 3 种检查方法的一致性、敏感性和特异性,旨在比较 3 种影像方法对诊断该病的效能。
资料与方法
一、一般资料
回顾性分析 2014 年 1 月 1 日至 2014 年 4 月30 日,我院同时行胸椎或腰椎 MRI 和 CT 检查的患者 50 例 ( MRI-CT 组 ),其中男 19 例,女 31 例,年龄 32~93 岁,平均 ( 69.86±14.34 ) 岁;分析同一时间段内同时行胸椎或腰椎 MRI 和 X 线平片检查的患者 70 例 ( MRI-X 线平片组 ),其中男 18 例,女52 例,年龄 22~89 岁,平均 ( 69.96±14.11 ) 岁。所有 MRI 扫描在 GE Signa HD 1.5 T MRI 机上进行,采集矢状位 T1WI、T2WI、STIR 和横轴位 T2WI 图像,矢状位扫描层厚 2.5 mm,横轴位扫描层厚为 5 mm;所有 CT 扫描在 GE Lightspeed 64 排 VCT 上进行,采集侧位定位像和横轴位图像 ( 层厚 0.625 mm ),然后进行 2.0 mm 横轴位和矢状位图像重建;所有 X 线平片在 DR 机上进行,拍摄正侧位片。
二、纳入及排除标准
影像科 2 名高年资主治医师采用双盲法分析两组中 MRI、CT 侧位定位像、CT 横轴位+矢状位重建图像 ( CT 重建图像 ) 和 X 线平片的所有影像资料。2 名医师各对所有资料前后分析 2 次,间隔 ≥2 周,分析的范围为 T4~L5椎体,当每组中两种检查方法覆盖椎体范围不一致时,取在交集范围内的每一个椎体进行分析,2 名医师对以上椎体诊断出是否有骨折 ( 无论新旧与否 ),并进行分级,比较每个椎体 2 名医师前后共计 4 次分析的诊断与分级结果,任何 2 次之间的结果 ( 2 人之间或 2 次之间 ) 出现不一致的椎体列入有疑问椎体排除出本研究。
三、影像资料的半定量分析
2 名高年资主治医师对所有的椎体进行半定量分析。分级方法:按椎体压缩的形态分为 4 个级别,0 级:椎体形态正常;1 级:椎体前部、中部或后部的轻度压缩,压缩高度约 20%~25%,压缩面积约 10%~20%;2 级:椎体中度压缩,压缩高度约 25%~40%,压缩面积约 20%~40%;3 级:椎体重度压缩,压缩高度和 ( 或 ) 面积达到 40%以上[2,5-6]。
四、统计学分析
统计 MRI-CT 组和 MRI-X 线平片组的 MRI 图像、CT 定位像、CT 重建图像以及 X 线平片中诊断压缩为 0 级、≥1 级 ( 1、2、3 级 )、≥2 级 ( 2、3 级 ) 的椎体个数,然后采用 kappa 分析,分别比较MRI 与 CT 定位像、MRI 与 CT 重建图像和 MRI 与X 线平片之间诊断压缩 ≥1 级和 ≥2 级的椎体的一致性,k>0.75 认为有好的一致性,~0.75 为中等程度的一致性,<0.4 为差的一致性;然后以 MRI 诊断为标准,以诊断为 0 级者为阴性,诊断为 ≥1 级者为阳性,分别计算两组资料中 CT 定位像、CT 重建图像和 X 线平片诊断椎体压缩性骨折的敏感性和特异性。采用 SPSS 13.0 软件进行统计学分析。
结 果
MRI-CT 组共有椎体 398 个,其中 MRI 诊断压缩程度为 0 级、≥1 级、≥2 级的椎体个数分别为 273 个、125 个、83 个;CT 侧位定位像诊断压缩程度为 0 级、≥1 级、≥2 级的椎体个数分别为321 个、77 个、65 个,在 CT 侧位定位像中有 6 例腰椎骨质密度明显减低,骨质边缘显示不清,难以辨别形态,按 0 级计算;CT 重建图像诊断压缩程度为 0 级、≥1 级、≥2 级的椎体个数分别为 292 个、106 个、78 个。MRI-X 线平片组共有椎体 480 个,其中 MRI 诊断压缩程度为 0 级、≥1 级、≥2 级的椎体个数分别为 360 个、120 个、78 个;X 线平片诊断压缩程度为 0 级、≥1 级、≥2 级的椎体个数分别为 393 个、87 个、67 个 ( 表 1 )。
MRI-CT 组中 MRI 与 CT 侧位定位像比较,诊断压缩 ≥1 级的椎体有中等程度的一致性 ( k=0.583 );MRI 与 CT 侧位定位像诊断压缩 ≥2 级的椎体有好的一致性 ( k=0.818 ) ( 表 2,3 );MRI 与 CT 重建图像比较,诊断压缩 ≥1 级 ( k=0.836 ) 和 ≥2 级 ( k=0.961 ) 的椎体均有好的一致性 ( 表 4,5 ) ( 图 1 )。MRI-X 线平片组中 MRI 和 X 线平片比较,诊断压缩 ≥1 级的椎体有中等程度的一致性 ( k=0.651 );诊断压缩 ≥2 级的椎体有好的一致性 ( k=0.862 ) ( 表 6,7 ) ( 图 2 )。

表1 MRI-CT 组和 MRI-X 线平片组诊断压缩性骨折分级各级椎体数 ( 个 )Tab.1 The number of vertebral bodies at different grades in both MRI-CT group and MRI-X-ray group ( n )
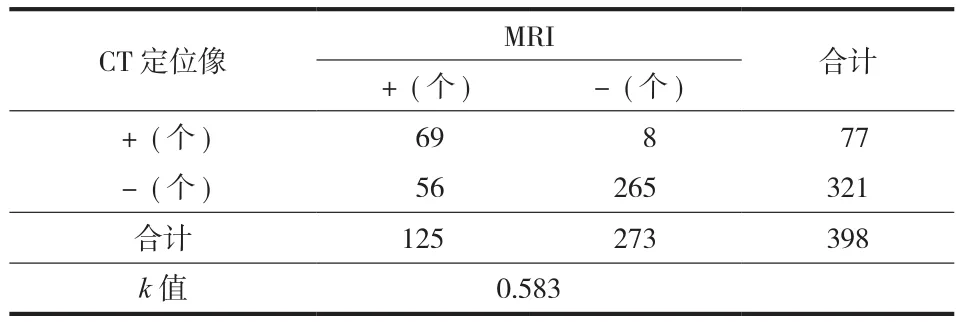
表2 MRI 和 CT 侧位定位像诊断压缩性骨折阴性和阳性的比较Tab.2 Comparison of MRI andlateral scout images of CT in the diagnosis of negative and positive compression fractures
MRI-CT 组中 CT 侧位定位像诊断为压缩 ≥1 级的敏感性为 55.2% ( 69 / 125 ),特异性为 97.1% ( 265 / 273 );CT 重建图像诊断为压缩 ≥1 级的敏感性为81.6% ( 102 / 125 ),特异性为 98.5% ( 269 / 273 )。MRI-X 线平片组中 X 线平片诊断为 ≥1 级的敏感性为 62.5% ( 75 / 120 ),特异性为 96.7% ( 348 / 360 )。
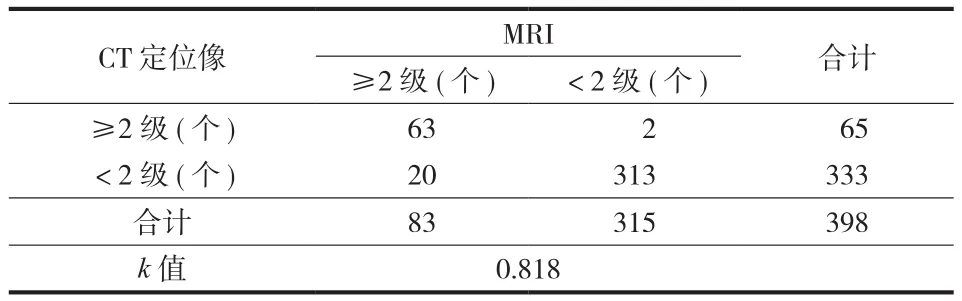
表3 MRI 和 CT 侧位定位像诊断压缩 ≥2 级骨折的比较Tab.3 Comparison of MRI andlateral scout images of CT in the diagnosis of compression fractures ≥ grade 2
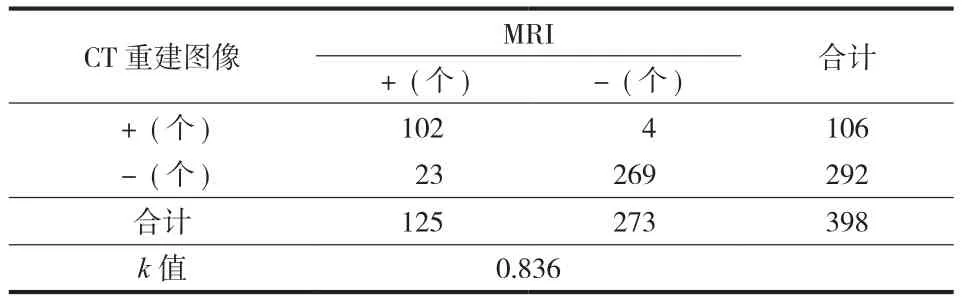
表4 MRI 和 CT 重建图像诊断压缩性骨折阴性和阳性的比较Tab.4 Comparison of MRI and CT reformation images in the diagnosis of negative and positive compression fractures
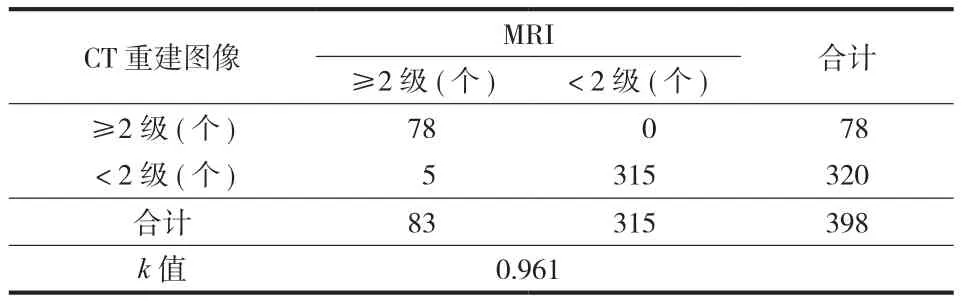
表5 MRI 和 CT 重建图像诊断压缩 ≥2 级骨折的比较Tab.5 Comparison of MRI and CT reformation images in the diagnosis of compression fractures ≥ grade 2
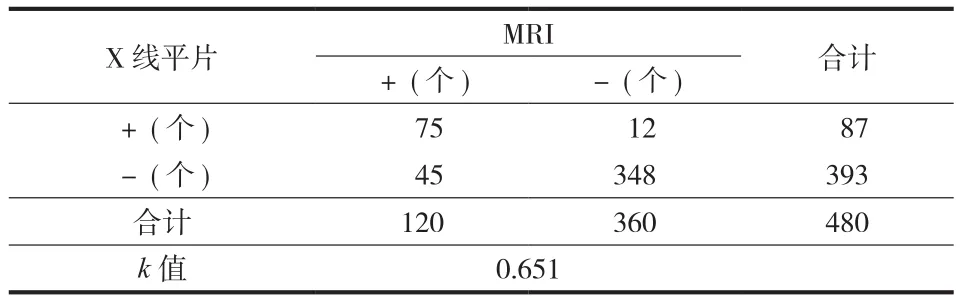
表6 MRI 和 X 线平片诊断压缩性骨折阴性和阳性的比较Tab.6 Comparison of MRI and X-ray plain flms in the diagnosis of negative and positive compression fractures
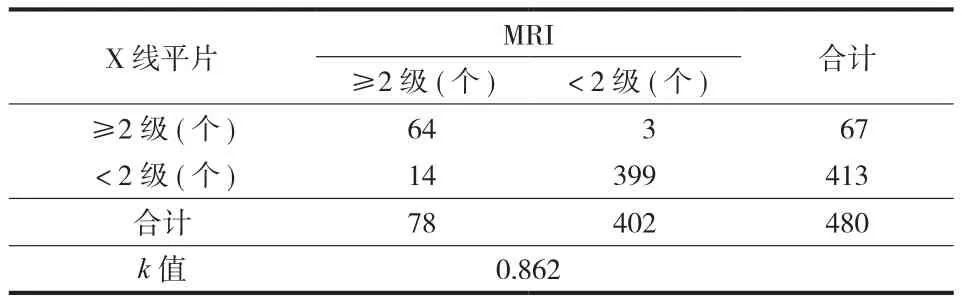
表7 MRI 和 X 线平片诊断压缩 ≥2 级骨折的比较Tab.7 Comparison of MRI and X-ray plaim flms in the diagnosis of compression fractures ≥ grade 2
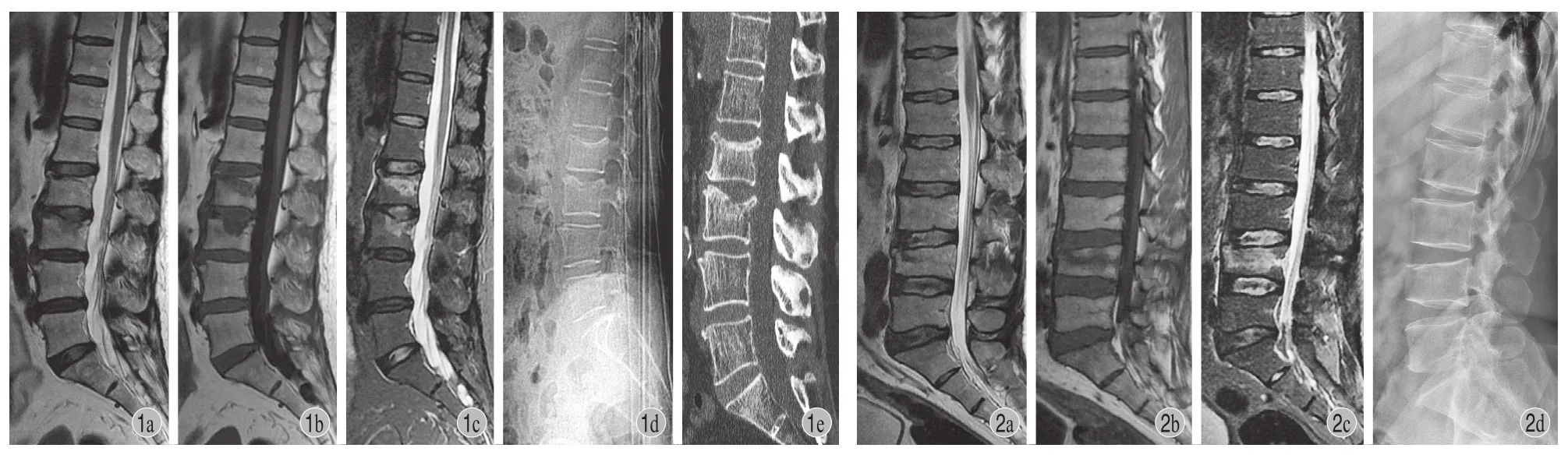
图1 患者,女,66 岁,腰椎 MRI 和 CT 对照 a~c:分别为矢状位 T2WI、T1WI 和 STIR 像,显示 L2椎体压缩性骨折 1 级,L3椎体压缩性骨折 2 级;d:为 CT 侧位定位像,显示 L2、L3椎体压缩性骨折,与 MRI 分级一致;e:为 CT 矢状位重建图像,显示 L2、L3椎体压缩性骨折,与 MRI 分级一致图 2 患者,男,48 岁,腰椎 MRI 与 X 线平片对照 a~c:分别为矢状位 T2WI、T1WI 和 STIR 像,显示 L4椎体压缩性骨折 2 级;d:为X 线侧位平片,显示 L4椎体压缩性骨折,与 MRI 分级一致Fig.1 The comparison of lumbar spine MRI and CT of a 66-year-old female a-c: The sagittal T2WI, T1WI and STIR images showed L2compression fractures of grade 1 and L3compression fractures of grade 2; d: The lateral scout image of CT showed L2and L3compression fractures, which was consistent with the MRI examination results; e: The sagittal CT reformation image showed the grade of L2and L3compression fractures was consistent with the MRI examination resultsFig.2 The comparison of lumbar spine MRI and X-ray plain flms of a 48-year-old male a-c: The sagittal T2WI, T1WI and STIR images showed L4compression fractures of grade 2; d: The lateral X-ray plain flm showed the grade of L4compression fractures was consistent with the MRI examination results
讨 论
本研究通过对相同病例的 MRI 和 X 线平片图像、MRI 和 CT 侧位定位像及 CT 重建图像的对比分析可以看出,对于诊断为 2 级以上的椎体压缩性骨折,X 线平片 ( k=0.862 )、CT 侧位定位像 ( k=0.818 ) 和 CT 重建图像 ( k=0.961 ) 与 MRI 图像之间均有好的一致性,其中 CT 重建图像的一致性最好。诊断包含 1 级的椎体压缩性骨折时,三者与 MRI 图像的一致性均有所下降,其中 CT 重建图像与 MRI图像仍有好的一致性 ( k=0.836 ),而 X 线平片 ( k=0.651 ) 和 CT 侧位定位像 ( k=0.583 ) 只有中等程度的一致性;同时可以看出 X 线平片、CT 侧位定位像和 CT 重建图像相对 MRI 图像诊断椎体压缩性骨折( ≥1 级 ) 的敏感性均不如其特异性高,其中 CT 重建图像相对 MRI 图像诊断椎体压缩性骨折 ( ≥1 级 )的敏感性和特异性均较高 ( 敏感性 81.6%,特异性98.5% ),而 CT 侧位定位像和 X 线平片诊断椎体压缩性骨折的特异性高 ( 分别为 97.1% 和 96.7% ),敏感性低 ( 分别为 55.2% 和 62.5% ),说明 CT 重建图像、CT 侧位定位像和 X 线平片发生误诊的几率均比较小,而 CT 侧位定位像和 X 线平片发生漏诊的几率大,从一致性分析可以推断出两者漏诊主要出现在对 1 级椎体压缩性骨折的诊断上。
本研究主要在矢状位上分析诊断椎体压缩性骨折。MRI 能够进行多体位扫描,从而得到矢状位和横轴位图像。大多文献认为矢状位 MRI 扫描对评估椎体形态起主要作用,也有报道认为 MRI 矢状位定位像与矢状位扫描图像诊断椎体压缩性骨折有很好的一致性[2-3]。MRI 另一个优势是多参数成像,MRI能够通过 T1WI、T2WI 和压脂序列的信号特点来分析出骨折所处的阶段,并对椎间盘、附件、韧带结构和脊髓结构一并作出判断,因此很容易与肿瘤、结核、骨髓炎等其它病理性骨折进行鉴别诊断,从而作出准确的定性诊断和骨折程度的分级[9-12]。由于 MRI 能通过多体位扫描清晰显示椎体的形态,通过信号特点准确诊断椎体是否为压缩性骨折并进行分级,故本研究将其作为椎体压缩性骨折诊断的标准与 CT 和 X 线平片进行比较,而 MRI 的缺点主要是扫描时间长且价格昂贵。CT 对骨皮质、骨小梁结构的显示比 MRI 更清晰,能够获得更小的层厚( 64 排螺旋 CT 最小 0.625 mm ),但以往的研究表明矢状位重建仍然比原始的横轴位图像诊断椎体压缩更敏感。Samelson 等[5]和 Kim 等[6]的研究认为,CT定位像对诊断椎体压缩性骨折与 CT 重建图像有好的一致性。本研究中侧位 CT 定位像与 MRI 对诊断2 级以上的椎体压缩有较好的一致性,而对 1 级以上的椎体压缩的诊断一致性较低,敏感性也较低,原因是骨质疏松,由于骨密度明显减低,造成椎体边缘在定位像上显示得不够清晰,有些椎体很难辨认或难以分级,只有对 2 级以上明显的变形,才容易被发现,而当椎体的骨密度正常,或仅仅由于外伤造成的轻度压缩时,CT 定位像则能作出准确诊断。一些文献通过分析胸部和腹部平扫时的椎体图像,得出 CT 的矢状位重建诊断压缩性骨折的敏感性和特异性均高于横轴位[3,8,11,13-15]。在实际工作中,横轴位和矢状位重建均会被一起作为常规观察,并且两者有一定的互补性。因此,本研究把两者共同作为一种检查方法参与比较,并得到了与 MRI 检查好的一致性,敏感性和特异性也较高,但与 MRI 相比,CT 仅有密度分辨这一个参数,对于一些椎体轻微变形的骨折,当骨密度与上下椎体相近时,会造成假阴性的结果。MRI 则较易辨认,这也可能是本研究中 CT 的敏感性不如特异性高的一个原因。另外 CT 和 MRI 图像的重建 / 扫描层厚也对分级有一定的影响,有报道认为矢状位层厚 ≤3 mm 对准确分级有重要的价值[1-2,7]。CT 的缺点是辐射剂量大,近年来低剂量扫描诊断椎体压缩性骨折的研究逐渐增多[14]。X 线平片一直是诊断椎体压缩性骨折的首选检查方法,简单易行,检查时间短,可以进行床旁拍摄,患者较易配合,本组 X 线平片诊断为 ≥2 级的椎体与 MRI 也有好的一致性,且诊断压缩性骨折的特异性也较高,但其对急性较轻微的压缩性骨折( 1 级 ) 的敏感性稍低,容易引起漏诊,本组研究中诊断的敏感性略高于 CT 定位像。
本研究的不足是样本量较少,没有对 2 名医师之间和前后 2 次之间的诊断分别进行比较,而是把 2 次诊断均不能达成一致意见的椎体排除出了研究,将在今后进一步扩大样本量一并进行研究,MRI 定位像也没有单独列出进行分析比较。总之,本研究中,MRI 和 CT 重建图像是最为可靠的检查方法,但 X 线平片和 CT 定位像由于特异性也很高,并且简单易行,辐射量小,仍可作为椎体压缩性骨折的筛查方法。利用各影像技术的优势,对椎体压缩性骨折进行综合分析和判定,无疑更科学、精准和可行。
[1]Daghigh MH, Safavi SS, Goldust M. Evaluation of magnetic resonance imaging signal changes in vertebral depressed fractures to determine the fracture time. Pak J Biol Sci, 2013, 16(6):299-300.
[2]Bazzocchi A, Garzillo G, Fuzzi F, et al. Localizer sequences of magnetic resonance imaging accurately identify osteoporotic vertebral fractures. Bone, 2014, 61:158-163.
[3]Kanchiku T, Imajo Y, Suzuki H, et al. Usefulness of an early MRI-based classification system for predicting vertebral collapse and pseudoarthrosis after osteoporotic vertebral fractures. J Spinal Disord Tech, 2014, 27(2):E61-65.
[4]Pizones J, Castillo E. Assessment of acute thoracolumbar fractures: challenges in multidetector computed tomography and added value of emergency MRI. Semin Musculoskelet Radiol, 2013, 17(4):389-395.
[5]Samelson EJ, Christiansen BA, Demissie S, et al. Reliability of vertebral fracture assessment using multidetector CT lateral scout views: the Framingham Osteoporosis Study. Osteoporos Int, 2011, 22(4):1123-1131.
[6]Kim YM, Demissie S, Genant HK, et al. Identification of prevalent vertebral fractures using CT lateral scout views: a comparison of semi-automated quantitative vertebral morphometry and radiologist semi-quantitative grading. Osteoporos Int, 2012, 23(3):1007-1016.
[7]Müller D, Bauer JS, Zeile M, et al. Significance of sagittal reformations in routine thoracic and abdominal multislice CT studies for detecting osteoporotic fractures and other spine abnormalities. Eur Radiol, 2008, 18(8):1696-1702.
[8]Bauer JS, Müller D, Ambekar A, et al. Detection of osteoporotic vertebral fractures using multidetector CT. Osteoporos Int, 2006, 17(4):608-615.
[9]方秀统, 于方, 付胜良, 等. 经皮椎体后凸成形术治疗老年人骨质疏松性脊柱压缩骨折的疗效分析. 中华医学杂志, 2013, 93(33):2654-2658.
[10]So KY, Kim DH, Choi DH, et al. The influence of fat infltration of back extensor muscles on osteoporotic vertebral fractures. Asian Spine J, 2013, 7(4):308-313.
[11]Voth M, Nau C, Marzi I. Thoracic and lumbar spinal injuries in children and adolescents. Unfallchirurg, 2013, 116(12): 1062-1068.
[12]Kim YJ, Chae SU, Kim GD, et al. Radiographic detection of osteoporotic vertebral fracture without collapse. J Bone Metab, 2013, 20(2):89-94.
[13]Carberry GA, Pooler BD, Binkley N, et al. Unreported vertebral body compression fractures at abdominal multidetector CT. Radiology, 2013, 268(1):120-126.
[14]Woo EK, Mansoubi H, Alyas F. Incidental vertebral fractures on multidetector CT images of the chest: prevalence and recognition. Clin Radiol, 2008, 63(2):160-164.
[15]Bartalena T, Giannelli G, Rinaldi MF, et al. Prevalence of thoracolumbar vertebral fractures on multidetector CT: underreporting by radiologists. Eur J Radiol, 2009, 69(3): 555-559.
( 本文编辑:王萌 李贵存 )
Research on the consistency of four imaging methods in the diagnosis of vertebral compression fractures
ZHANG Xiang, SUN Jin-lei, FU Ya-dong, WANG Yan-lin, JIN Yu-lian, LIANG Jie, LI Bao-qing. Department of Radiology, Beijing Shijingshan Hospital, 100043, PRC
ObjectiveTo analyze the consistency of magnetic resonance ( MRI ), lateral scout images of computed tomography ( CT ), reformation images of CT and X-ray plain flms in the diagnosis of vertebral compression fractures.MethodsFrom January 1, 2014 to April 30, 2014, 50 patients ( 398 vertebral bodies ) underwent thoracic or lumbar spine MRI and CT examinations and 70 patients ( 480 vertebral bodies ) had spine MRI and X-ray examinations, whose clinical data were retrospectivley analyzed. The vertebral body from T4to L5were involved. The semi-quantitative ( SQ ) method was used to classify the fractures as grade 0 to 3 according to the degree of vertebral compression. The number of vertebral bodies at different grades were respectively counted in all the patients based on the MRI, lateral scout images of CT, reformation images of CT and X-ray plain flms. A Kappa analysis was used to assess the consistency between MRI and lateral scout images of CT and between MRI and reformation images of CT in the diagnosis of compression fractures ≥ geade 1 and ≥ grade 2. And then the consistency between MRI and X-ray plain flms were assessed in the diagnosis of compression fractures ≥ geade 1 and ≥ grade 2. MRI was considered as the standard in the diagnosis of fractures, and grade 0 was taken as negative resultes and ≥ geade 1 as positive results. Finally, the sensibility and specificity of scout images and reformation images of CT and X-ray plane films were calculated in the diagnosis of vertebral compression fractures.ResultsA fair consistency existed between MRI and lateral scout images of CT in the diagnosis of fractures ≥ grade 1 ( k=0.583 ), and a good consistency in the diagnosis of fractures ≥ grade 2 ( k=0.818 ). A good consistency was noticed between MRI and reformation images of CT in the diagnosis of fractures ≥ grade 1 and 2 ( k=0.836 and k=0.961 ). A fair consistency was found between MRI and X-rayplain flms in the diagnosis of fractures ≥ grade 1 ( k=0.651 ), and a good consistency in the diagnosis of fractures ≥grade 2 ( k=0.862 ). The sensibility and specifcity of lateral scout images of CT, reformation images of CT and X-ray plain flms were 55.2% and 97.1%, 81.6% and 98.5% and 62.5% and 96.7% respectively in the diagnosis of vertebral compression fractures.ConclusionsThe best consistency is detected between MRI and reformation images of CT in the diagnosis of vertebral compression fractures. When compared with that of MRI, the sensibility and specifcity of reformation images of CT are higher. And while the sensibility of lateral scout images of CT and X-ray plan flms is higher and their specifcity is lower than that of MRI.
Fractures, compression; Magnetic resonance imaging; Tomography, X-ray; Tomography, X-ray computed
10.3969/j.issn.2095-252X.2014.11.003
R683.2, R445
首都卫生发展科研专项自主创新项目 ( 首发 2014-2-112 );首都临床特色应用研究项目 ( z141107002514072 )
100043 北京市石景山医院医学影像科
李葆青,libaoqing@21cn.com
2014-08-05 )
