房颤患者立体心电图P环特点与射频消融术后复发的关系
2013-08-08马君马长生李学文
马君,马长生,李学文
房颤患者立体心电图P环特点与射频消融术后复发的关系
马君,马长生,李学文
目的应用立体心电图(3D-ECG)分析房颤患者心房传导时间、传导方向及振幅的变化与房颤射频消融术后复发的关系。方法纳入2009年12月-2010年3月在北京安贞医院确诊房颤并进行射频消融术的患者42例。分别在患者射频消融术术前及术后采集窦性心律3D-ECG并同步获取12导联心电图,分析每位患者射频消融术前、术后心房传导时间,P环除极方向及振幅与射频消融术术后复发的关系。查阅入选患者病历资料获取此次射频消融术术前心脏超声心动图左房内径数值及患者病史年限等资料,分析该组数据与房颤发生和射频消融术后复发的关系。结果术后P环方位对房颤复发具有明显影响(P=0.027),P环方位异常者房颤复发风险是P环方位正常者的8.4倍;左房大小对房颤复发的影响亦有统计学意义(P=0.022);P环运行时间差对房颤复发的影响位于检验水准附近(P=0.058)。病史年限每增加1年,射频消融术后房颤复发的风险增加1.363倍。相关分析显示,右房直径与术后P环最大振幅呈正相关(P=0.044),随右房直径增加,术后P环最大振幅呈增大趋势。结论随着病史时间延长,心房传导时间延长,心房除极方位及振幅发生变化,房颤患者的心房发生电重构和结构重构,二者共同作用导致了房颤的发生与维持。
心房颤动;导管消融术;电重构;结构重构
立体心电图(three-dimensional electrocardiogram,3D-ECG)问世于1989年,是指采用Frank校正导联体系,经过方法学的改进,通过不同的三维角度,同步采样,同源转换,显示及描记出立体心电向量图(3D-VCG)和立体影像心电图(3DI-ECG)[1]。目前临床上通过分析房颤危险因素来预测房颤发生的研究较多。无创心电图检查的预测指标主要是P波离散度及信号平均心电图的心房传导时间和心房除极末RMS(均方差)振幅等。3D-ECG技术利用计算机成像技术描记出心脏的立体心电向量环,可单独或同时显示P、QRS、T环,并可旋转及放大,便于观察和分析心脏的电活动“路径”[2-3]。3D-ECG还可以显示心动周期任意时间的振幅和空间角度,能准确反映患者的情况。本研究应用3D-ECG对房颤患者心房传导时间、心房除极方向和振幅的变化进行分析,旨在探讨P环运行状况与房颤射频消融术后复发的关系。
1 资料与方法
1.1 研究对象 选取2009年12月-2010年3月入住北京安贞医院心内科确诊房颤并行射频消融术的患者42例,男29例,女13例,年龄57.5±12.3岁,其中合并高血压病24例,冠心病4例。阵发性房颤34例,持续性房颤8例,术前病情均平稳,无明显心功能不全。纳入标准:阵发性及持续性房颤患者,有明确的病史及既往有体表心电图或动态心电图明确记录证据;左室射血分数>40%,无明显心功能不全。进行检查前,患者均知情同意并已停用抗心律失常药物。
1.2 仪器 3D-ECG仪(北京卡迪斯医疗科技有限公司生产)。类别:E型号;准确度:标准灵敏度±5%;质量标准:京药监械(准)字2007第2210227号。一次性纽扣式心电电极(北京市天润伟业医用设备厂)。
1.3 检测方法及随访 采集所有入选患者射频消融术术前和术后的3D-ECG,同时记录患者超声心动图左房内径数值。在走速50mm/s、增益20mm/mV条件下测量每位患者的3D-ECG,在稳定窦性心律下取明确起始点及终点的P波进行测量并记录所得心房传导时间、心房除极方位及振幅等数据。起始点与终点均选取与等电位线交点处。由安贞医院房颤中心派专人按照手术后1、3、6个月进行电话随访。复发的判定标准:消融术后3个月内发生的房颤/房扑/房速,如果持续时间≥30s视为早期复发;消融术后3个月后发生的房颤/房扑/房速,如果持续时间≥30s视为远期复发,12个月以后的为更远期复发。
1.4 统计学处理 采用SPSS 16.0软件进行统计分析,计量资料以表示,采用logistic回归及简单直线回归分析。P<0.05为差异有统计学意义。
2 结 果
2.1 房颤患者的3D-ECG总体特征 简单直线回归分析发现,随着病程年限增加,房颤患者P环运行时间延长越发明显,同时心房直径也随之增大,P环方位异常,由正常的左下前方位发生了各种改变。P环振幅异常。3D-ECG的P环振幅正常应<0.12mV,增大则提示右房负荷过重。
2.2 心房传导特点、左房大小及病史与房颤复发的相关性 Logistic回归分析发现,P环方位、P环运行时间差、左房内径以及病史均与房颤发生相关(表1)。病史年限每增加1年,射频消融术后房颤复发的风险增加1.363倍。典型病例:一例P环大致正常房颤患者,房颤病史半年,心房传导方向大致正常,心房除极运行时间略延长,行射频消融术后半年内未复发(图1);另一例P环明显异常的房颤患者,病史8年,心房传导方向明显异常,心房除极运行时间延长,行射频消融术后3个月及6个月均有复发情况(图2);一例房颤患者,病程6年,高血压病史50年,冠心病史3年,心房内径明显扩大,左房50mm×46mm×62mm,右房57mm×58mm,P环方位术前为左上前,术后为左下前,射频消融术有效纠正了异位电活动,术后该患者1个月内有早期复发,药物干预后6个月内未复发(图3)。
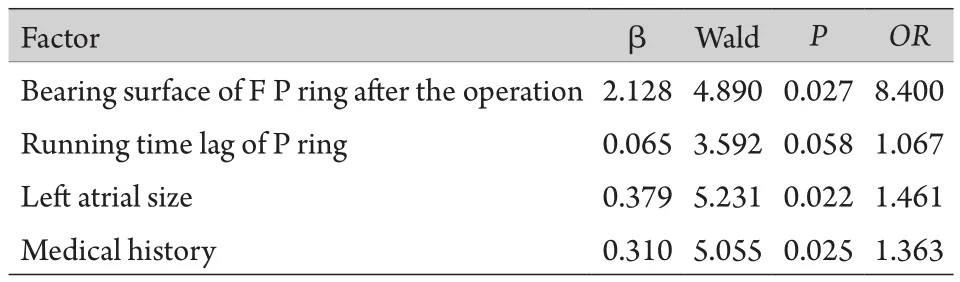
表1 心房传导方位变化、左房大小及病史与房颤复发的关系Tab.1 Directional changes of atrial conduction and the relationship between left atrial size and the recurrence of atrial fibrillation recurrence
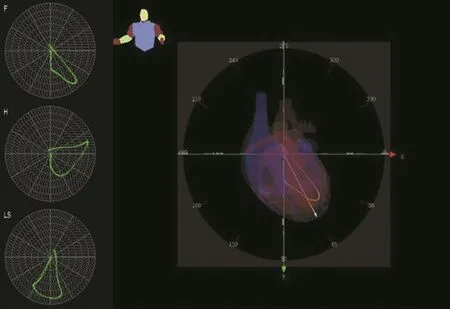
图1 P环大致正常房颤患者3D-ECGFig. 1 Three-dimensional electrocardiogram (3D-ECG) of patients with atrial fibrillation and roughly normal P ring
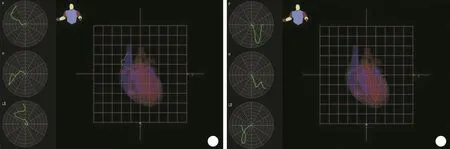
图3 房颤患者射频消融术前、术后的P环运行状况Fig.3 P ring running status in patients with atrial fibrillation before and after radiofrequency ablation
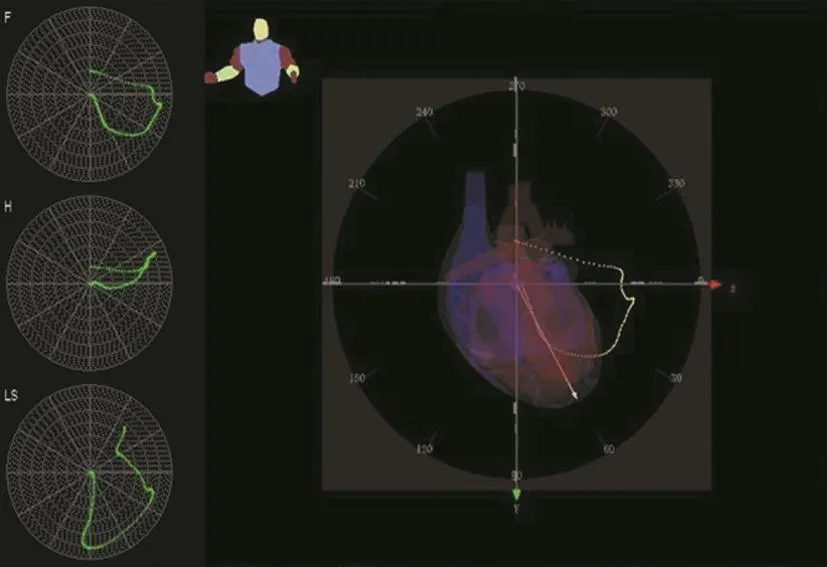
图2 P环明显异常的房颤患者射频消融术后房颤高复发Fig. 2 Hyper-recurrence of atrial fibrillation in patients with atrial fibrillation and obviously abnormal P ring after radiofrequency ablation
2.3 右心房直径与P环最大振幅的关系 简单直线回归分析显示,右房直径与术前最大振幅无线性关系,但与术后最大振幅存在线性关系且有统计学意义(表2),且由图4可知,随着右房直径增加,术后最大振幅呈增加趋势,表达式如下:y=0.108+0.024x。
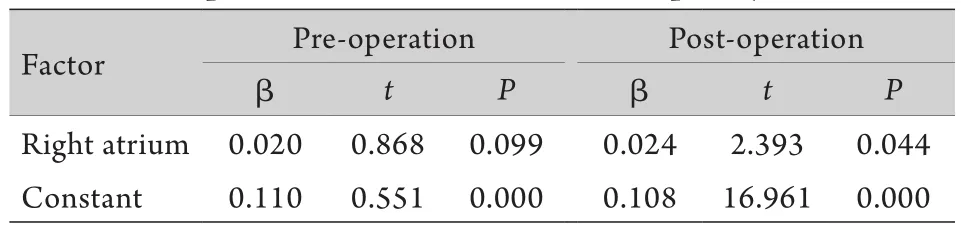
表2 右房直径与射频消融术术前及术后P环最大振幅大小的关系Tab.2 The relationship between right atrial inner diameter and maximum amplitude before and after radiofrequency ablation
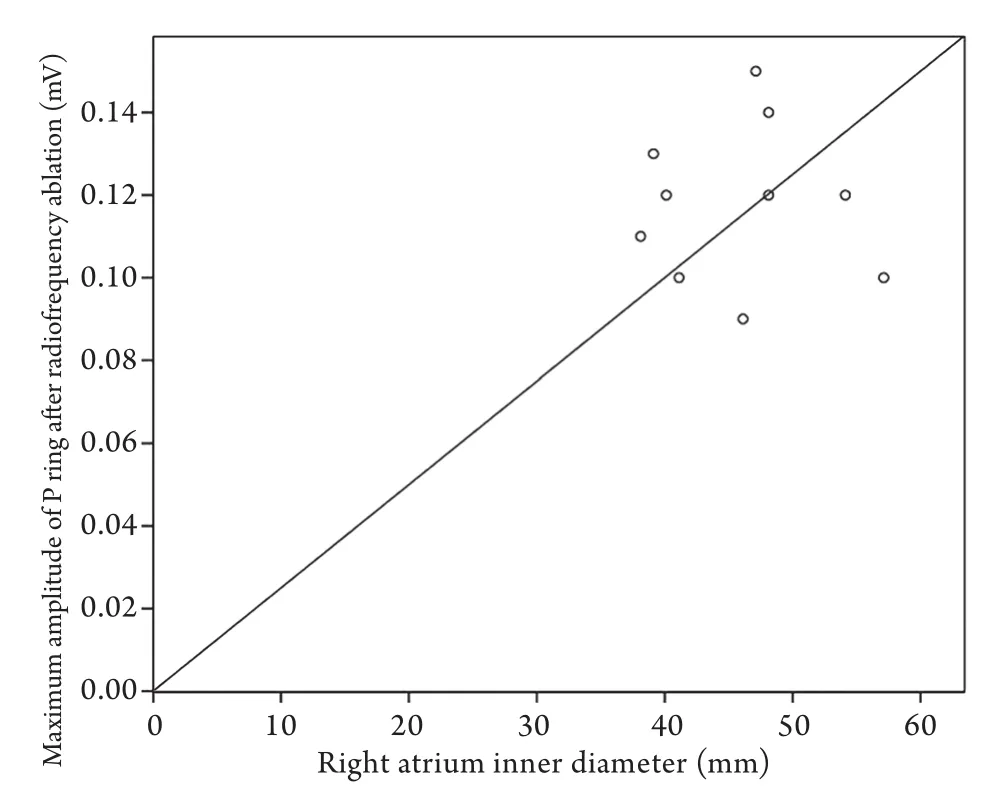
图4 射频消融术后P环最大振幅与右房的关系Fig.4 Relationship between maximum amplitude of P ring and right atrial after radiofrequency ablation
3 讨 论
心房除极运行时间及除极方位与心房结构重构及电重构相关。P环运行时间延长提示心房结构发生改变,内径增大,而P环的方位发生改变则说明心房内电活动异常。心房电重构与结构重构共同作用导致了房颤的发生与维持。3D-ECG可从多个角度说明心房除极的方向、除极运行的时间以及振幅的变化。
本研究应用3D-ECG分析房颤患者射频消融术前及术后心房传导时间、心房除极方向和振幅、心房结构变化,结果显示:①随着病史的延长,房颤患者心房传导时间延长,同时心脏彩超显示心房结构发生相应改变,此类患者在行射频消融术后房颤容易复发。有研究发现,心肌细胞间的结构及电活动改变,可引起心房不应期离散度增大或导致局部心肌电活动传导异常,使激动传导减慢、路径曲折,从而促进房颤的发生及维持。左房越大、左右房的病理改变越明显,电复律的效果就越差[4],提示左房容积和左房心肌病理改变是房颤发生的重要基础。②一些房颤患者心房除极时间延长并不明显,但心房除极方向发生异常,表明心房已经存在电重构,同样也为射频消融术后复发奠定了基础[5-7]。心房发生电重构后,心肌自律性增高,局灶发放的异位冲动使心房组织提前除极,产生振荡性后电位,形成微折返,是诱发或触发房颤的因素,对房颤维持起着重要作用。③P波振幅正常应<0.12mV,增大表示右房负荷过重,P波振幅与右房彩超数据分析结果表明,一部分患者存在右房负荷过重,进一步导致了肺动脉高压、肺静脉周围电活动异常,这从另一个角度说明了目前证实的房颤机制之一,即起源于肺静脉的局灶快速激动。有研究表明心房传导时间及整个P波振幅的增加与严重高血压相关[8]。2000年Mandapati等[9]的研究结果显示位于左房内具有极短周长的“转子”伴颤动样传导是肺静脉起源的房颤的发生机制;近年临床肺静脉电隔离术也证实起源于肺静脉的局灶快速激动在通过肺静脉前庭时容易形成折返及颤动样传导,导致房颤维持。
综上所述,3D-ECG可通过三维的心房除极时间、方位及振幅等指标分析心房传导时间和心房除极末振幅,从心房除极角度和立体三维P环进一步研究预测房颤的发生[10]。心房电重构与结构重构共同作用导致了房颤的发生及维持[11],随着病史延长,疾病本身又会进一步加重心房结构的重构,成为房颤维持和射频消融术后复发的重要因素。射频消融是目前治疗房颤的有效方法,及时治疗高血压、冠心病、风湿性心脏瓣膜病、心肌病、甲状腺功能亢进等可能导致心房结构重构的疾病,控制可以导致房颤发生的危险因素,在必要时及早进行有效的射频消融治疗可以减少心房结构的重构,缩短病程,避免血栓并发症的发生。随着时代的变迁,科学技术的发展,有关房颤的研究进展较快,射频消融术的技术也在不断提高,房颤临床治愈已经成为可能。
[1] Zhao F. Vector diagram of electrocardiogram, heart, a threedimensional evaluation of electrocardiogram (ECG) and outlook[J]. Clin Equip, 2004, 3(6): 33-37. [赵峰. 对心电图、心向量图、立体心电图的评价暨展望[J]. 常规医疗装备, 2004, 3(6): 33-37.]
[2] Rosiak M, Bolinska H, Ruta J. P wave dispersion and P wave duration on SAECG in predicting atrial fibrillation in patients with acute myocardial infarction[J]. Ann Noninvasive Electrocardiol, 2002, 7(4): 363-368.
[3] Budeus M, Felix O, Hennersdorf M,et al. Prediction of conversion from paroxysmal to permanent atrial fibrillation[J]. Pacing Clin Electrophysiol, 2007, 30(2): 243-252.
[4] Yang SS, Han W, Zhou HY,et al. Effects of spironolactone on electrical and structural remodeling of atrium in congestive heart failure dogs[J]. Chin Med J (Engl), 2008, 121(1): 38-42.
[5] Vranka I, Penz P, Dukát A. Atrial conduction delay and its association with left atrial dimension, left atrial pressure and left ventricular diastolic dysfunction in patients at risk of atrial fibrillation[J]. Exp Clin Cardiol, 2007, 12(4): 197-201.
[6] Jurkko R, Väänänen H, Mäntynen V,et al. High-resolution signal-averaged analysis of atrial electromagnetic characteristics in patients with paroxysmal lone atrial fibrillation[J]. Ann Noninvasive Electrocardiol, 2008, 13(4): 378-385.
[7] Karaca M, Kinay O, Nazli C,et al. The time interval from the Initiation of the P-wave to the start of left atrial appendage ejection flow: does it reflect- interatrial conduction time[J]? Echocardiography, 2007, 24(8): 810-815.
[8] Madu EC, Baugh DS, Gbadebo TD,et al. Effect of ethnicity and hypertension on atrial conduction: evaluation with highresolution P-wave signal averaging[J]. Clin Cardiol, 2001, 24(9): 597-602.
[9] Mandapati R, Skanes A, Chen J,et al. Stable microreentrant sources as a mechanism of atrial fibrillation in the isolated sheep heart[J]. Circulation, 2000, 101(2): 194-199.
[10] Daniel G, Lissa G, Medina Redondo D,et al. Real-time 3D vectorcardiography: an application for didactic use[J]. J Phys: Conf Ser, 2007, 90 012013 doi:10.1088/1742-6596/90/1/012013.
[11] Guo LN, Liu YS, Cui MY. Expression of platelet derived growth factor β receptor in atrial tissue during atrial fibrillation of dogs[J]. J Zhengzhou Univ (Med Sci) , 2011, 46(1): 34-37. [郭林娜, 刘元生, 崔明玉. 心房颤动犬心肌组织中血小板源生长因子受体β的表达[J]. 郑州大学学报(医学版), 2011, 46(1): 34-37.]
Relationship between three-dimensional electrocardiographic P ring features and atrial fibrillation (AF) recurrence after radiofrequency ablation in AF patients
MA Jun1,2, MA Chang-sheng2, LI Xue-wen31Department of Cardiology, Beijing Anzhen Hospital Affiliated to Capital Medical University, Beijing 100029, China
2ICU of Mentougou District Hospital, Beijing 102300, China
3Department of Cardiology, Shanxi Large Hospital, Taiyuan 030001, China
ObjectiveTo explore the relation of the conduction time, conduction direction and amplitude of threedimensional electrocardiogram (3D-ECG) to the recurrence after radiofrequency ablation in atrial fibrillation (AF) patients.MethodsForty-two patients diagnosed with AF and receiving radiofrequency ablation in Beijing Anzhen Hospital from December 2009 to March 2010 participated in the present study. 3D-ECG and synchronous 12-lead ECG of sinus rhythm was recorded before and after radiofrequency ablation to analyze the correlation between the recurrence of AF after radiofrequency ablation and atrial conduction time, depolarization direction or amplitude of P ring. Meanwhile, the left atrial diameter determined by echocardiography before ablation and medical history were recorded, and the relationship between these data and both the occurrence of AF and recurrence after ablation was analyzed.ResultsThe azimuth of P ring after surgery could significantly affect the recurrence of AF (P=0.027), and the recurrence risk in patients with abnormal azimuth of P ring was 8.4 times that in patients with regular azimuth. The left atrial diameter could also significantly affect the recurrence (P=0.022), while the influence of the difference in P ring response duration on AF recurrence was near the significant level (P=0.058). The risk of AF recurrence increased 1.363-fold with each one additional year of AF history. A positive correlation was found between the right atrial diameter and maximal amplitude of P ring (P=0.044).ConclusionWith the development of AF, atrial conduction time become longer, and atrial depolarization azimuth and amplitude change, then the atrial electrical and anatomical remodeling occur, and both of them could lead to the occurrence and maintenance of AF.
atrial fibrillation; catheter ablation; electrical remodeling; structure reconstruction
R541.7
A
] 0577-7402(2013)10-0847-04
10.11855/j.issn.0577-7402.2013.10.014
2013-06-12;
2013-08-13)
(责任编辑:张小利)
马君,医学硕士,主治医师。主要从事心内科的临床工作
100029 北京 首都医科大学附属北京安贞医院心内科[马君(现在北京市门头沟区医院ICU工作)、马长生];030001 太原 山西大医院心内科(李学文)