不同干预措施对腰痛患者恐动症干预效果的网状Meta分析
2023-06-25巩应霞吴慧娟许瑞贾鸿安王渭昭王慧娟苗俊芳
巩应霞 吴慧娟 许瑞 贾鸿安 王渭昭 王慧娟 苗俊芳




【摘要】 目的:采用網状Meta分析的方法评价不同干预措施对腰痛患者恐动症干预效果。方法:计算机检索The Cochrane Library、PubMed、WOS、Embase、CNKI、CBM、VIP、WanFang Data数据库中与腰痛患者恐动症干预措施相关的随机对照试验,检索时限从建库至2022年1月。由2名研究者独立筛选文献、提取资料并评价纳入研究的偏倚风险后,采用Stata 16.0软件进行网状Meta分析。结果:纳入16项研究,1 137例患者。网状Meta分析结果显示,认知行为疗法、虚拟现实训练与常规治疗相比,差异均有统计学意义。SUCRA概率排序结果显示,由高到低依次为虚拟现实训练>认知行为疗法>疼痛神经科学教育>多学科协作疗法>手法治疗>物理治疗>普拉提>分级活动>常规治疗>视频锻炼。结论:本研究证据表明,虚拟现实训练干预腰痛患者恐动症效果最优,其次是认知行为疗法。受纳入研究数量和质量限制,上述结论还需开展更多高质量的RCT来对本研究结果进一步验证。
【关键词】 腰痛 恐动症 网状Meta分析
A Network Meta-analysis of the Effect of Different Interventions in Kinesiophobia Patients with Low Back Pain/GONG Yingxia, WU Huijuan, XU Rui, JIA Hong'an, WANG Weizhao, WANG Huijuan, MIAO Junfang. //Medical Innovation of China, 2023, 20(09): -157
[Abstract] Objective: To evaluate the effect of different interventions in kinesiophobia patients with low back pain by using network meta-analysis. Method: Randomized controlled trials related to kinesiophobia intervention in patients with low back pain were searched in The Cochrane Library, PubMed, WOS, Embase, CNKI, CBM, VIP and WanFang Data databases. The retrieval period is from database construction to January 2022. Two researchers independently screened the literature, extracted data, and evaluated the risk of bias in the included studies. Stata 16.0 software was used for mesh Meta-analysis. Result: A total of 16 studies involving 1 137 patients were included. Results of network Meta-analysis showed that cognitive behavioral therapy, virtual reality training, and multidisciplinary collaborative therapy were statistically significant compared with conventional treatment. The ranking results of SUCRA probability showed that the order from high to low was virtual reality training >cognitive behavioral therapy >pain neuroscience education >multidisciplinary collaborative therapy >manual therapy >physical therapy >Pilates >graded activity >routine therapy >video exercise. Conclusion: The evidence of this study indicates that virtual reality training has the best effect on motility in patients with low back pain, followed by cognitive behavioral therapy. Due to the limitations of the number and quality of the included studies, the above conclusions need to be further verified by more high-quality RCTS.
[Key words] Low back pain Kinesiophobia Network Meta-analysis
First-author's address: School of Nursing, Gansu University of Traditional Chinese Medicine, Lanzhou 730000, China
doi:10.3969/j.issn.1674-4985.2023.09.036
腰痛是最常见的肌肉骨骼疾病之一,也是世界范围内导致疼痛、功能障碍、残疾的主要因素之一[1-2]。恐动症(kinesiophobia)也被称为运动恐惧症,即对身体运动和活动产生过度的、非理性的、使人衰弱的恐惧,这种恐惧是由于对疼痛刺激或害怕再次受伤的脆弱感造成的[3]。恐动症在腰痛人群中的发生率较高,对腰痛患者日常活动、情绪、生活质量都有着不良影响[4]。有研究表明,患有腰痛且运动恐惧程度较高的患者发生身体残疾的风险比无运动恐惧症腰痛患者高出41%[5]。腰痛患者因疼痛对功能锻炼产生逃避心理,而功能锻炼等措施在腰痛患者康复中占有重要地位[6]。近年来,国内外对腰痛患者恐动症的干预措施多样,不同措施干预效果不一。因此,本文采取网状Meta分析[7]的方法评价不同干预措施对腰痛患者恐动症的干预效果,以期为腰痛患者恐动症的干预方法选择提供科学依据。
1 资料与方法
1.1 纳入标准及排除标准
1.1.1 纳入标准 (1)纳入类型,国内外公开发表的随机对照试验(randomized controlled trail,RCT);(2)研究对象,临床正式诊断为腰痛的患者;(3)干预措施,试验组采用虚拟现实训练(虚拟现实训练[8]、虚拟行走[9])、认知行为疗法(认知功能治疗[10]、认知行为治疗[11]、认知行为团体干预[12])、多学科协作疗法(多学科项目干预[13]、多学科管理[14]、多学科康复计划[15])、普拉提[16-17]、分级活动[18-19]、视频锻炼(基于视频锻炼的远程康复软件家庭锻炼[20]、基于视频游戏的练习[21])、手法治疗[22]、疼痛神经科学教育[23]等干预措施;对照组采用常规治疗或物理治疗;(4)結局指标,主要结局指标为恐动症评分表(Tampa Scale of Kinesiophobia,TSK)。
1.1.2 排除标准 (1)研究对象合并下肢深静脉曲张、危重症、急性期和手术患者;(2)非中英文文献、重复发表、TSK量表数据缺乏或不能获取全文的研究;(3)综述、个案报道、系统评价/Meta分析、回顾总结、会议论文或学位论文等。
1.2 文献检索策略 计算机检索The Cochrane Library、PubMed、Web of Science、Embase、CNKI、VIP、WanFang Data、CBM数据库中与腰痛患者恐动症干预措施相关的RCT,检索时限从建库至2022年1月。中文检索词包括:腰痛、慢性腰痛、慢性下背痛、慢性腰背痛、慢性腰痛、恐动症、运动恐惧症、恐惧回避信念、疼痛灾难化、干预措施、干预治疗、随机对照试验等;英文检索词包括:back pain,lumbago,lumbar pain,Kinesiophobia,fear of movement,fear of reinjur,panic disorder,pain catastrophizing,fear avoidance,intervention,intervening measure,randomized controlled trial。检索
采用主题词与自由词相结合的方式,同时所有检索策略均通过多次检索后确定,最后的检索策略必须经过所有作者一致同意。
1.3 文献筛选及资料提取 由2名研究者独立进行文献检索与筛选、提取资料并交叉核对,出现分歧时,邀请第三方协助判断。将检索文献导入Endnote X9软件去除重复文献,阅读题目、摘要进行初筛,删除不相关的文献,进一步阅读全文,以确定是否纳入。提取信息包括:研究特征(例如第一作者姓名、发表时间、国家等),患者特点(例如患者例数、平均年龄、性别比例等),干预措施(例如干预的形式、持续时间等),测量指标(TSK评分)。
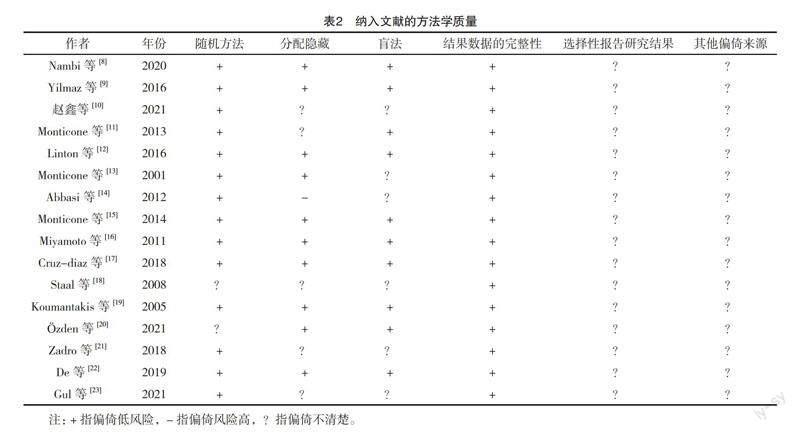
1.4 文献质量评价 由2名研究者按照Cochrane Handbook 5.1.0版本中推荐的偏倚风险评估标准对纳入文献进行质量评价,主要评价内容包括:(1)随机序列的产生;(2)分配隐藏;(3)实施偏倚(研究和受试者实施盲法);(4)测量偏倚(研究结局盲法评价);(5)随访偏倚(结果数据的完整性);(6)报告偏倚;(7)其他。
1.5 统计学处理 运用Stata 16.0软件进行网状Meta分析,对连续性变量采用均数差(MD)及95%置信区间(CI)为效应量进行分析。采用SUCRA(surface under the cumulative ranking)进行概率排序,根据SUCRA值呈现干预措施。SUCRA的累积排序概率越大,其治疗效果就越佳[24]。当存在闭合环时,进行不一致性检验,若P>0.05,则无显著性差异;同时采用节点劈裂法进行局部不一致性检验,P>0.05时说明局部不一致性,无统计学意义。
2 结果
2.1 文献检索结果 根据检索策略,初步检索出相关文献5 258篇,用Endnote X9软件去除重复文献1 559篇,根据纳入和排除标准,阅读相关题目及摘要,排除不相关文献,最后纳入16篇文献,文献筛选流程及结果见图1。
2.2 纳入文献的基本特征 本研究共纳入16篇文献,其中英文文献15篇,中文文献1篇,共1 137例慢性腰痛患者,纳入文献基本特征见表1。
2.3 纳入文献的方法学质量评价 纳入分析的16项研究中2项研究未提及明确的随机方法,10研究提及分配隐藏,10项研究提及盲法。纳入16篇文献数据完整性较好,纳入文献的方法学质量评价见表2。
2.4 网状Meta的分析结果
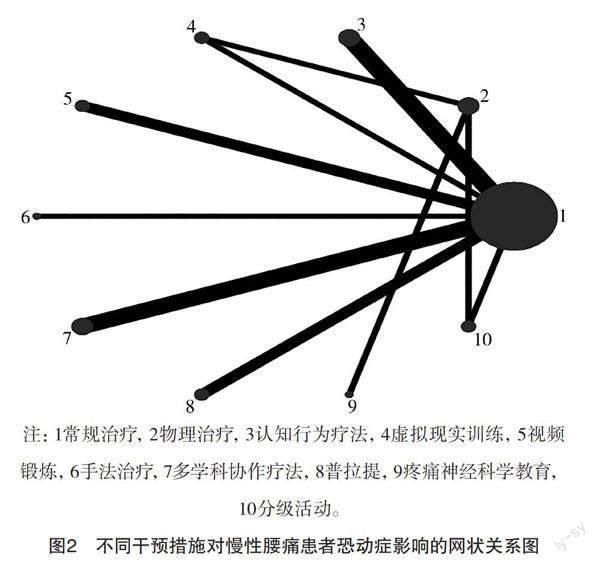
2.4.1 网状关系图 图中的每个圆点代表一种干预措施,圆点越大表明此干预措施包含样本量越大。由图可见圆点1面积最大,1-3、1-5、1-7、1-8之间的连线较粗,表明纳入研究中干预措施1-3、1-5、1-7、1-8之间比较的研究出现频率较多,各干预措施之间的网状关系见图2。
2.4.2 一致性检验 16项研究结果报道了10种不同干预措施之间TSK评分比较,检验结果显示P=0.342 4,P>0.05,不一致性检验无统计学意义,即本研究结果一致性较好。
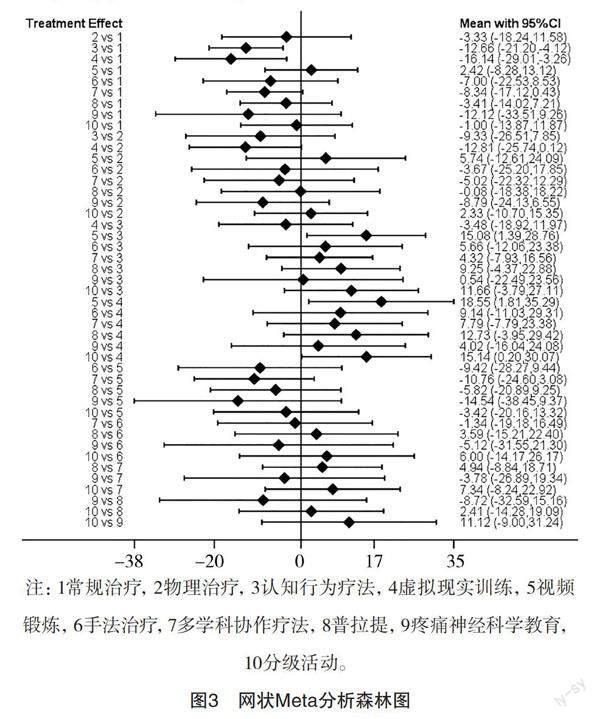
2.4.3 网状Meta分析森林图 当MD的95%CI包含0时,说明两种干预措施比较无统计学意义,反之,则有统计学意义。网状Meta分析结果显示,认知行为疗法与常规治疗相比、虚拟现实训练与常规治疗相比,两种干预措施应用效果差异均有统计学意义,分级活动与虚拟现实训练相比、视频锻炼与虚拟现实训练相比应用效果差异均有统计学意义,其余干预措施两两比较差异均无统计学意义,见图3。
2.4.4 结果排序 不同干预措施的SUCRA由高到低依次为虚拟现实训练(SUCRA=86.7)、认知行为疗法(SUCRA=77.9)、疼痛神经科学教育(SUCRA=71.5)、多学科协作疗法(SUCRA=61.5)、手法治疗(SUCRA=54.8)、物理治疗(SUCRA=42.9)、普拉提(SUCRA=40.2)、分级活动(SUCRA=30.3)、常规治疗(SUCRA=22.5)、视频锻炼(SUCRA=16.4)。不同干预措施对腰痛患者恐动症影响效果SUCRA累积概率排序图见图4。
2.4.5 发表偏倚评价 漏斗图可见两侧基本对称分布,说明本研究存在发表偏倚的可能性较小,见图5。
3 讨论
3.1 纳入研究的质量评价 本文纳入的16篇文献均为RCT,其中14篇研究均报告了产生随机序列的具体方法,16项研究数据结果完整,方法质量学评价为B级文献。纳入研究中的试验组与对照组的基线资料差异无统计学意义(P>0.05),具有可比性。
3.2 虚拟现实训练对腰痛患者恐动症效果最佳,可作为优先选择 网状Meta分析结果和SUCRA结果表明,相比其他干预措施,虚拟现实训练对腰痛患者恐动癥的效果最优。有研究表明,恐动症是加重腰痛患者继续发展的最强预测因子之一[25-28]。短期内避免运动可降低疼痛焦虑而有益于腰痛患者,但长期而言,有限的活动会导致脊柱关节周围结缔组织缩短、周围肌肉的萎缩[29-31]。腰痛患者负面想法和信念会使患者出现恐惧回避行为,阻碍康复进程[32]。虚拟现实治疗是一种有效的疼痛分散治疗,它专注于外部刺激而不是身体运动,主要任务是通过分散注意力来减少对疼痛的注意力[33-34]。有研究表明,虚拟现实训练是有效的干扰因素,可以显著降低干预过程中的疼痛等不舒适感[35-38]。Bordeleau等[39]最近发表的一篇Meta分析表明虚拟现实训练不仅可以有效地改善腰痛的疼痛强度,还对运动活动有积极影响,以一种有趣且有吸引力的方式参与康复锻炼,虚拟环境提供的互动元素和反馈可以增加患者对练习的坚持[33,40]。此外,虚拟现实被认为对腰痛患者是一种经济高效的工具[41]。因此,与常规治疗方法相比,虚拟现实训练具有一定优势,可以分散疼痛的注意力,激发患者参与度,并鼓励继续积极参与治疗。
3.3 认知行为疗法对腰痛患者恐动症效果显著 认知行为疗法干预效果显著。认知行为疗法由4部分组成:患者对疼痛及其疼痛感的认知和理解、学习积极的应对策略、维持应对策略、处理疼痛和挑战性情境的问题的解决方法。Wenzel等[42]认为,认知行为疗法可以改变不适应行为,克服回避行为,从而改善自我护理。在Yang等[43]的Meta分析中指出认知行为疗法能够有效改善慢性腰背痛(CLBP)患者的疼痛、残疾、恐惧回避和自我效能。认知行为疗法通过人与人之间的交流互动,改变不良认知和行为,建立正确的康复观念,促进早日康复。
3.4 其他干预措施对慢性腰痛患者恐动症干预效果尚不确定 本研究结果表明,视频训练、手法治疗、普拉提、疼痛神经科学教育、分级活动与常规治疗相比,差异均无统计学意义;视频训练、手法治疗、普拉提、疼痛神经科学教育、分级活动与物理治疗相比,差异均无统计学意义。目前,暂无足够证据证明除虚拟现实训练、认知行为疗法以外的干预措施对腰痛患者恐动症改善有显著效果。本Meta分析中纳入视频锻炼2篇、手法治疗1篇、普拉提3篇、疼痛神经科学教育1篇、分级活动2篇,排除了低质量的原始文献后,纳入研究少,尚不能证实其对慢性腰痛患者恐动症干预有效性,需未来进行高质量原始研究证明其显著性。
3.5 本研究的局限性 (1)纳入的部分文献未进行分配隐藏,可能存在实施、测量偏倚。(2)纳入的不同干预措施文献数量较少,网状关系图形成的闭合环偏少。(3)同一种干预措施因研究人员理解不同,故研究人员具体实施方案稍微有所差别。
4 结论
当前研究表明,对慢性腰痛患者恐动症进行干预时,虚拟现实训练是目前最优的干预措施,其次是认知行为协作疗法。因此,在对患者进行干预时,可根据实际需求选择更为适宜的措施来改善慢性腰痛患者恐动症的影响,以实现更好的干预效果。受纳入研究数量和质量限制,上述结论还需开展更多高质量的RCT来对本研究结果进一步验证。
参考文献
[1] SEBBAG E,FELTEN R,SAGEZ F,et al.The world-wide burden of musculoskeletal diseases: a systematic analysis of the World Health Organization Burden of Diseases Database[J].Ann Rheum Dis,2019,78(6):844-848.
[2] JAMES S L,AABTEE D,ABATE K H,et al.Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the global burden of disease study 2017[J].The Lancet 2018,392(10159):1789-1858.
[3] LINTON S J,NORDIN E.A 5-year follow-up evaluation of the health and economic consequences of an early cognitive behavioral intervention for back pain: a randomized, controlled trial[J].Spine (Phila Pa 1976),2006,31(8):853-858.
[4] ANTUNES R S,DE MACEDO B G,AMARAL TDA S,et al.
Pain, kinesiophobia and quality of life in chronic low back pain and depression[J].Acta Ortop Bras,2013,21(1):27-29.
[5] TROCOLI T O,BOTELHOotelho R V.Prevalência de ansiedade, depressão e cinesiofobia em pacientes com lombalgia e sua associacao com os sintomas da lombalgia[J].Revista Brasileira de Reumatologia,2016,56(4):330-336.
[6] MACDONALD D A,MOSELEY G L,HODGES P W.The lumbar multifidus: does the evidence support clinical beliefs?[J].Man Ther,2006,11(4):254-263.
[7]張天嵩.Stata软件network组命令在网状Meta分析中的应用[J].中国循证医学杂志,2015,15(11):1352-1356.
[8] NAMBI G,ABDELBASSET W K,ALRAWAILI S M,et al.
Virtual reality or isokinetic training; its effect on pain, kinesiophobia and serum stress hormones in chronic low back pain: a randomized controlled trial[J].Technol Health Care,2021,29(1):155-166.
[9] YILMAZ YELVAR G D,ÇIRAK Y,DALKILINC M,et al.Is physiotherapy integrated virtual walking effective on pain, function, and kinesiophobia in patients with non-specific low-back pain? Randomised controlled trial[J].Eur Spine J,2017,26(2):538-545.
[10]赵鑫,徐斌,肖涛,等.认知功能治疗对重度持续性腰痛患者临床疼痛与实验性疼痛敏感性的改善效果[J].颈腰痛杂志,2021,42(2):266-268.
[11] MONTICONE M,FERRANTE S,ROCCA B,et al.Effect of a long-lasting multidisciplinary program on disability and fear-avoidance behaviors in patients with chronic low back pain: results of a randomized controlled trial[J].Clin J Pain,2021,29(11):929-938.
[12] LINTON S J,RYBERG M.A cognitive-behavioral group intervention as prevention for persistent neck and back pain in a non-patient population: a randomized controlled trial[J].Pain,2001,90(1-2):83-90.
[13] MONTICONE M,AMBROSINI E,ROCCA B,et al.Group-based task-oriented exercises aimed at managing kinesiophobia improved disability in chronic low back pain[J].Eur J Pain,2016,20(4):541-551.
[14] ABBASI M,DEHGHANI M,KEEFE F J,et al.Spouse-assisted training in pain coping skills and the outcome of multidisciplinary pain management for chronic low back pain treatment: a 1-year randomized controlled trial[J].Eur J Pain,2012,16(7):1033-1043.
[15] MONTICONE M,AMBROSINI E,ROCCA B,et al.A multidisciplinary rehabilitation programme improves disability, kinesiophobia and walking ability in subjects with chronic low back pain: results of a randomised controlled pilot study[J].Eur Spine J,2014,23(10):2105-2113.
[16] MIYAMOTO G C,COSTA L O,GALVANIN T,et al.The efficacy of the addition of the Pilates method over a minimal intervention in the treatment of chronic nonspecific low back pain: a study protocol of a randomized controlled trial[J].J Chiropr Med,2011,10(4):248-254.
[17] CRUZ-DIAZ D,ROMEU M,VELASCO-GONZALEZ C,et al.The effectiveness of 12 weeks of Pilates intervention on disability, pain and kinesiophobia in patients with chronic low back pain: a randomized controlled trial[J].Clin Rehabil,2018,32(9):1249-1257.
[18] STAAL J B,HLOBIL H,KOKE A J,et al.Graded activity for workers with low back pain: who benefits most and how does it work?[J].Arthritis Rheum,2008,59(5):642-649.
[19] KOUMANTAKIS G A,WASTO P J,OLDHAM J A.Trunk muscle stabilization training plus general exercise versus general exercise only: randomized controlled trial of patients with recurrent low back pain[J].Phys Ther,2005,85(3):209-225.
[20] ÖZDEN F,SARI Z,KARAMAN Ö N,et al.The effect of video exercise-based telerehabilitation on clinical outcomes, expectation, satisfaction, and motivation in patients with chronic low back pain[J].Ir J Med Sci,2022,191(3):1229-1239.
[21] ZADRO J R,SHIELEY D,SIMIC M,et al.Video-game-based exercises for older people with chronic low back pain: a randomized controlledtable trial (GAMEBACK)[J].Phys Ther,2019,99(1):14-27.
[22] DE OLIVEIRA M F,De OLIVEIRA M C J C,DA SILVA E B.Osteopathic manipulation treatment versus therapeutic exercises in patients with chronic nonspecific low back pain: a randomized, controlled and double-blind study[J].J Back Musculoskelet Rehabil,2020,33(3):367-377.
[23] GUL H,EREL S,TORAMAN N F.Physiotherapy combined with therapeutic neuroscience education versus physiotherapy alone for patients with chronic low back pain: a pilot, randomized-controlled trial[J].Turk J Phys Med Rehabil,2021,67(3):283-290.
[24] SALANTI G,ADES A E,LOANNIDIS J P.Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: an overview and tutorial[J].J Clin Epidemiol,2011,64(2):163-171.
[25] CHOU R,SHEKELLE P.Will this patient develop persistent disabling low back pain?[J].JAMA,2010,303(13):1295-1302.
[26] NICHOLAS M K,LINTON S J,WATSON P J,et al."Decade of the Flags" Working Group. Early identification and management of psychological risk factors ("yellow flags") in patients with low back pain: a reappraisal[J].Phys Ther,2011,91(5):737-753.
[27] GEORGE S Z,BENECIUK J M.Psychological predictors of recovery from low back pain: a prospective study[J].BMC Musculoskelet Disord,2015,16:49.
[28] MAIN C J,GEORGE S Z.Psychologically informed practice for management of low back pain: future directions in practice and research[J].Phys Ther,2011,91(5):820-824.
[29] HIDES J A,RICHARDSON C A,JULL G A.Magnetic resonance imaging and ultrasonography of the lumbar multifidus muscle. Comparison of two different modalities[J].Spine (Phila Pa 1976),1995,20(1):54-58.
[30] HIDES J A,RICHARDSON C A,JULL G A.Multifidus muscle recovery is not automatic after resolution of acute, first-episode low back pain[J].Spine (Phila Pa 1976),1996,21(23):2763-2769.
[31] LIEBER RL, STEINMAN S, BARASH IA, et,al. Structural and functional changes in spastic skeletal muscle[J].Muscle Nerve,2004,29(5):615-627.
[32] VLAEYEN J W S,LINTON S J.Fear-avoidance model of chronic musculoskeletal pain: 12 years on[J].Pain,2012,153(6):1144-1147.
[33] PERIRA M F,PRAHM C,KOLBENSCHLAG J,et al.
Application of AR and VR in hand rehabilitation: a systematic review[J].J Biomed Inform,2020,111:103584.
[34] MATHEVE T,BOGAERTS K,TIMMERMANS A.Virtual reality distraction induces hypoalgesia in patients with chronic low back pain: a randomized controlled trial[J].J Neuroeng Rehabil,2020,17(1):55.
[35] MALLOY K M,MILLING L S.The effectiveness of virtual reality distraction for pain reduction: a systematic review[J].Clin Psychol Rev,2010,30(8):1011-1018.
[36] HOFFMAN H G,PATTERSON D R,SOLTANI M,et al.
Virtual reality pain control during physical therapy range of motion exercises for a patient with multiple blunt force trauma injuries[J].Cyberpsychol Behav,2009,12(1):47-49.
[37] HOFFMAN H G,PATTERSON D R,SEIBEL E,et al.Virtual reality pain control during burn wound debridement in the hydrotank[J].Clin J Pain,2008,24(4):299-304.
[38] GOLD J I,BELMONT K A,THOMAS D A.The neurobiology of virtual reality pain attenuation[J].Cyberpsychol Behav,2007,10(4):536-544.
[39] BORDELEAU M,STAMENKOVIC A,TARDIF P A,et al.The use of virtual reality in back pain rehabilitation: a systematic review and Meta-Analysis[J].J Pain,2022,23(2):175-195.
[40] DE MIGGUEL-RUBIO A,RUBIO M D,ALBA-RUEDA A,
et al.Virtual reality systems for upper limb motor function recovery in patients with spinal cord injury: systematic review and Meta-Analysis[J/OL].JMIR Mhealth Uhealth,2020,8(12):e22537.https://pubmed.ncbi.nlm.nih.gov/33270040/.
[41] LI L,YU F,SHI D,et al.Application of virtual reality technology in clinical medicine[J].Am J Transl Res,2017,9(9):3867-3880.
[42] WENZEL A.Basic strategies of cognitive behavioral therapy[J].Psychiatr Clin North Am,2017,40(4):597-609.
[43] YANG J,LO W L A,ZHENG F,et al.Evaluation of cognitive behavioral therapy on improving pain, fear avoidance, and self-efficacy in patients with chronic low back pain: a systematic review and Meta-analysis[J].Pain Res Manag,2022,2022:4276175.
(收稿日期:2022-10-18) (本文編辑:张明澜)
