糖尿病与人工关节置换术后假体周围感染的相关性研究
2018-04-24赵振马保安龙华牛舜
赵振 马保安 龙华 牛舜
糖尿病已经成为最常见的慢性疾病之一。据统计 2013 年,全球大约有 3 亿 8200 万人患糖尿病,预计到 2035 年将上升至 5 亿 9200 万;而大多数糖尿病患者生活在低收入和中等收入的国家和地区( 包括中国 )[1]。文献报道中关节置换的患者中糖尿病患者的比例约为 7.8%~25%[2-9]。O’Toole 等[3]报告到 2030 年进行人工关节置换 ( total joint arthroplasty,TJA ) 的患者中大约 40% 将是糖尿病患者。
TJA 能够明显缓解患者关节疼痛、改善关节功能、提高患者生活质量,已经成为治疗终末期关节疾病最有效的方法之一。但是术后并发症,特别是关节假体周围感染 ( prosthetic joint infection,PJI ),常导致严重后果,并造成患者严重的经济负担[10-13]。据报道,PJI 在关节置换后的发生率为0.51%~3.35%[6,8-9,11,13-18],同时 Bozic 等[19]认为 PJI 患病率可能因为其诊断的困难而被低估。并且 PJI 已经成为术后翻修的最常见原因之一,超过 25% 的翻修是由于发生感染,而这个比例还在上升。据多篇文献报道,糖尿病被认为是关节置换后发生 PJI 的独立危险因素[7,20-25]。也有研究认为糖尿病和 PJI 患病率并没有相关性[26-27]。本研究回顾性分析了我院经治的 1799 例全髋、全膝关节置换术患者的临床资料,以探讨糖尿病及糖耐量异常与初次人工全髋及全膝关节置换术后感染的关系。
资料与方法
一、纳入标准与排除标准
1. 纳入标准:( 1 ) 2010 年 1 月至 2016 年 3 月,在我院行初次人工全髋或全膝关节置换者;( 2 ) 临床诊断明确者;( 3 ) 年龄 ≥ 18 岁者。
2. 排除标准:( 1 ) 资料不全者;( 2 ) 失访或随访时间<12 个月者;( 3 ) 合并有免疫功能缺陷或者其它特殊的内科疾病者;( 4 ) 肿瘤患者;( 5 ) 肺部感染者。
二、数据收集
本研究共纳入 1799 例,2319 个人工关节 ( 双侧同时置换者 520 例 )。其中糖尿病组 361 例,共453 个人工关节 ( 双侧同时置换者 92 例 ),非糖尿病组 1438 例,共 1866 个人工关节 ( 其中双侧同时置换者 428 例 ),1799 例随访至少 12 个月 ( 12~48 个月 )。基线资料收集包括年龄,性别,吸烟史,并发症 ( 脑梗、冠心病 ),高血压史,手术时间,是否炎性关节炎。
三、诊断标准
1. 本次研究采用美国肌肉与骨骼感染协会 ( Muscularskeletal infection society,MSIS ) 共识 PJI 的诊断标准:( 1 ) 2 次假体周围标本培养出同一种致病菌或发现与关节相通的窦道;( 2 ) 当下列 6 种情况中存在 4 种时:ESR 及 CRP 水平升高;关节液中 WBC计数升高;关节液中 PMN% 升高;受感染关节周围发现脓液;从 1 例假体周围组织标本中培养、分离出细菌;假体组织病理学分析,在 5 个或以上高倍镜视野下观察到至少 5 个中性粒细胞 / 视野。
2. 糖尿病诊断标准 WHO ( 1999 年 ):( 1 ) 糖尿病症状 ( 典型症状包括多饮、多尿和不明原因的体重下降 ) 加 ① 随机血糖 ≥ 11.1 mmol / L ( 200 mg /dl ) 或 ② 空腹血糖 ≥ 7.0 mmol / L ( 126 mg / dl ) 或③ 葡萄糖负荷后 2 h 血糖 ≥ 11.1 mmol / L ( 200 mg /dl );( 2 ) 无糖尿病症状者,需另日重复检查明确诊断。糖耐量异常诊断标准:6.1 mmol / L ≤ 空腹血糖<7.0 mmol / L 和 ( 或 ) 7.8 mmol / L ≤ 葡萄糖负荷后 2 h 血糖<11.1 mmol / L。
四、统计学处理
本次队列研究数据采用 SPSS 19.0 软件进行统计分析,对基线资料采用χ2检验或非参数检验,通过Logistic 回归分析来计算比值比 ( odds ratios,OR) 和95% 可信区 ( confidence intervals,CI),评估糖尿病与 PJI 发病率的相关性。之后将性别、年龄、手术时间、高血压病史、并发症进行分层,评估糖尿病与 PJI 发病率的相关性。最后按照血糖正常、糖耐量异常、糖尿病患者进行分组,评估糖尿病及糖耐量异常与 PJI 发病率的相关性。以P≤ 0.05 差异有统计学意义。
结 果
糖尿病组与非糖尿病组在性别、手术时间及吸烟史方面差异无统计学意义 (P>0.05 )。糖尿病组中高龄人群、高血压患者、患有其它并发症比例高于非糖尿病组患者 (P<0.05 ) ( 表1 )。
糖尿病组患者 PJI 发生风险提高了 1.83 倍 ( 95%CI:1.01~3.32,P<0.05 );调节性别、年龄、手术时间、吸烟、高血压、并发症、炎性关节炎等因素后OR值为 1.8 ( 95%CI:0.971~3.34,P=0.06 ) ( 表2 )。
表3 将患者性别、年龄、手术时间、并发症进行分层后,女性患者中相较于非糖尿病患者,糖尿病组患者 PJI 发生风险提高了 2.0 倍 ( 95%CI:0.95 ~4.1;P=0.067 );年龄<55 岁患者中糖尿病组患者比非糖尿病患者 PJI 发生风险提高了 6.2 倍 ( 95%CI:0.95~41.1,P=0.057 );手术时间>180 min 患
注:广泛调节:调节性别、年龄、手术时间、吸烟、高血压、并发症、炎性关节炎
Notice: Wide range of adjustment: to adjust the gender, age, operation time,smoking, high blood pressure, complications, inflammatory arthritis者中相较于非糖尿病患者,糖尿病患者发生 PJI 的OR值为 3.2 ( 95%CI:1.2~8.7;P<0.05 ),明显高于手术时间<180 min 组;双侧同时行人工关节置换患者组中,糖尿病患者 PJI 发病率的OR值为 7.2( 95%CI:1.2~43.6;P<0.05 ),明显高于仅行单侧人工关节置换组患者 (OR值为 1.9 )。
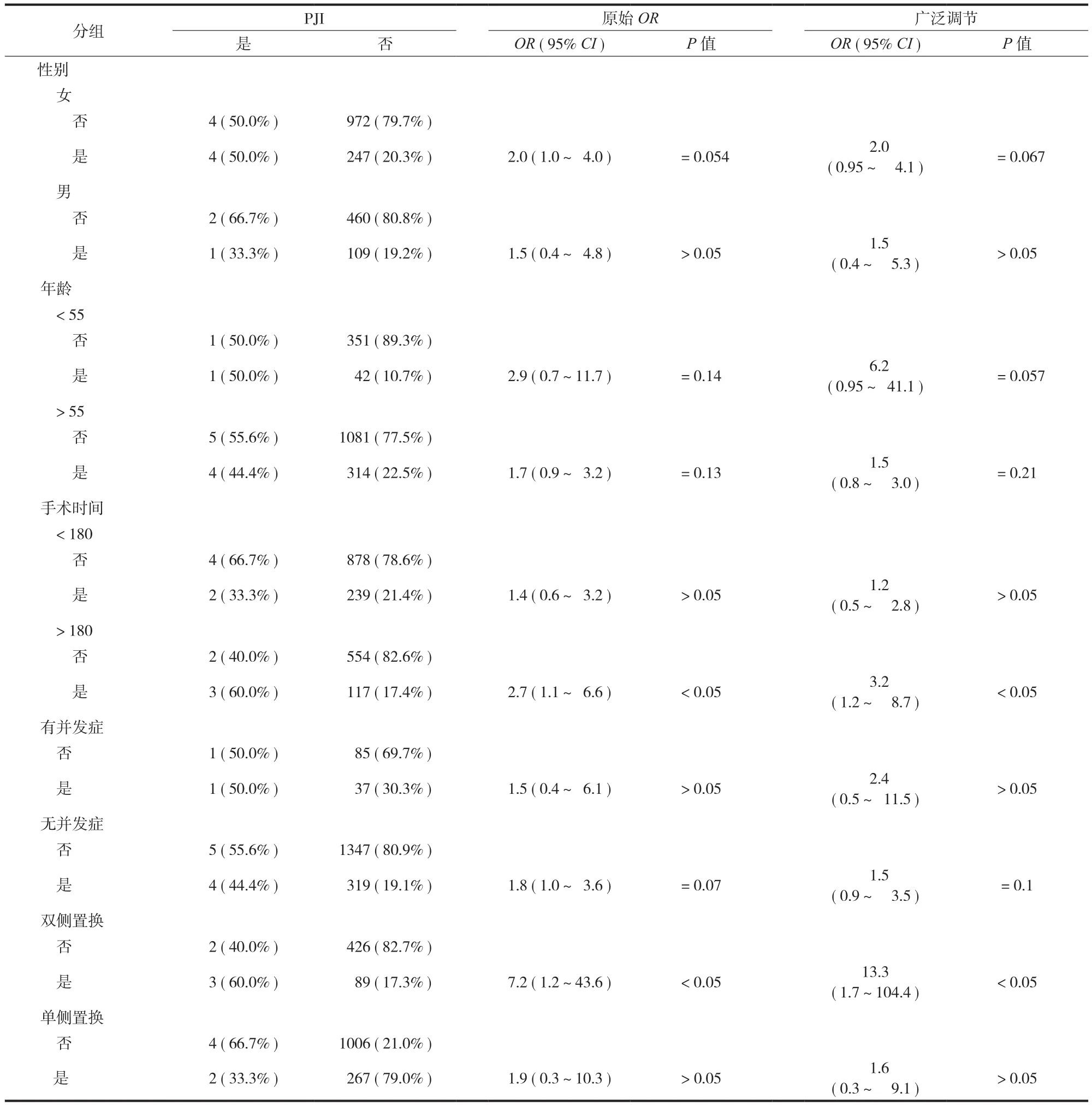
表3 糖尿病与 PJI 相关性的分层分析Tab.3 Stratified analysis of the relationship between diabetes mellitus and periprosthetic infection
糖尿病组患者的糖耐量异常,血糖正常组患者在性别、手术时间、吸烟史及炎性关节病方面差异无统计学意义 (P>0.05 )。糖尿病组中高龄人群、高血压患者、患有其它并发症比例高于糖耐量异常组及血糖正常组患者 (P<0.05 ) ( 表4 )。
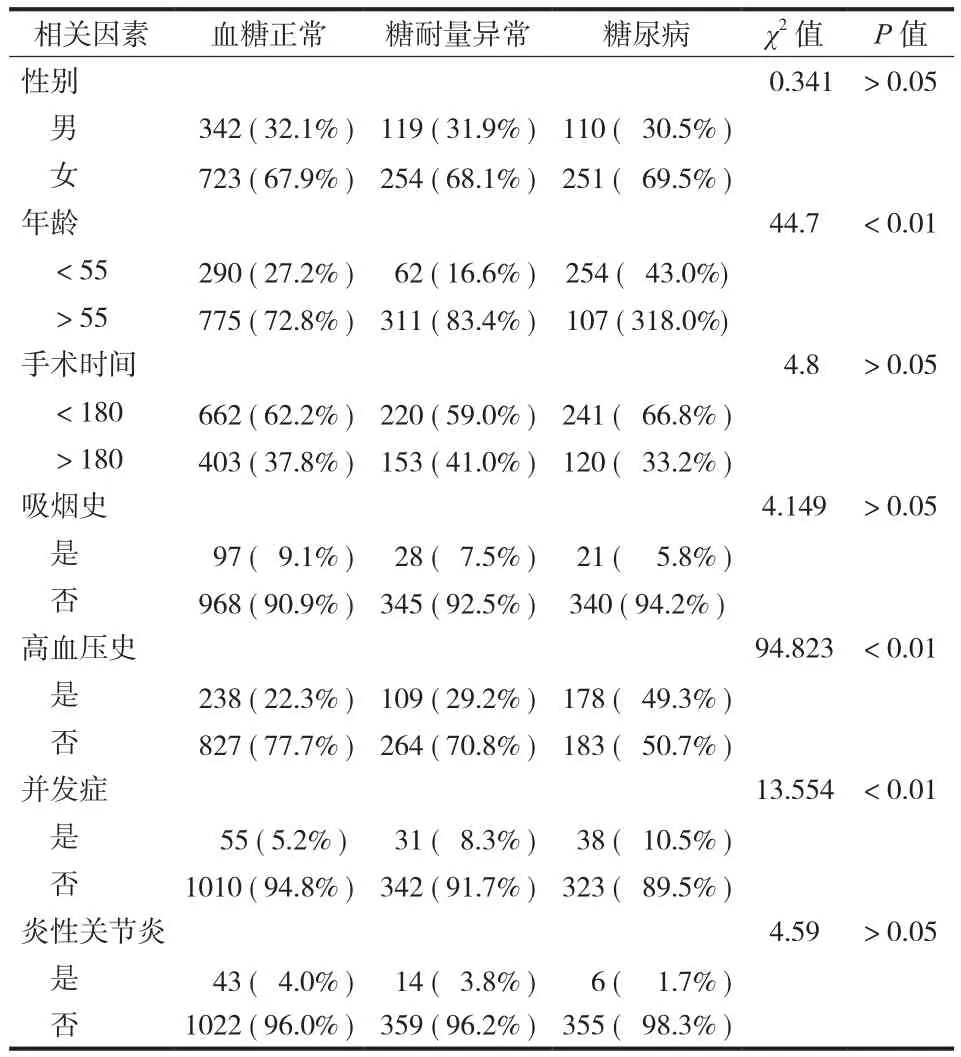
表4 按照血糖正常、糖耐量异常、糖尿病分组患者基线资料特点Tab.4 Baseline characteristics in different groups: normal blood glucose, abnormal glucose tolerance and diabetes mellitus
糖尿病组患者及糖耐量异常患者 PJI 发生风险提高了 7.5 倍 ( 95%CI:1.4~38.7,P<0.05 ) 和 5.8 倍( 95%CI:1.1~31.6,P<0.05 );调节性别、年龄、手术时间、吸烟、高血压、并发症、炎性关节炎等因素后OR值分别为 7.2 ( 95%CI:1.3~39.2,P<0.05 ) 和 5.6 ( 95%CI:1.0~31.0,P<0.05 ) ( 表5 )。
讨 论
本研究结果显示,糖尿病及糖耐量异常患者TJA 术后发生 PJI 的风险会显著增加,糖尿病患者双侧同时行 TJA 时,更容易发生 PJI。
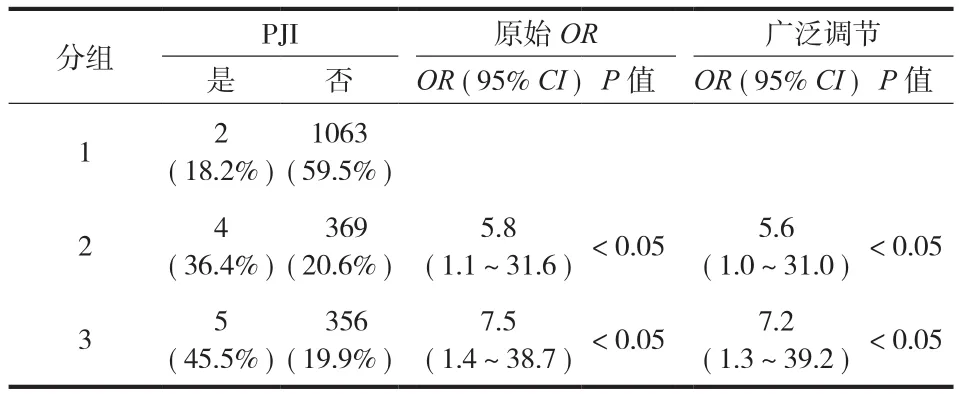
表5 糖尿病及糖耐量异常与 PJI 相关性的比较Tab.5 Comparison of the relationship between diabetes mellitus,abnormal glucose tolerance and periprosthetic infection
Namba 等[7]回顾性分析了 56 216 例 TKA 患者,发现糖尿病患者 TKA 术后发生 PJI 的风险是无糖尿病患者的 1.28 倍。同时 Iorio 等[18]报告 4241 例关节置换患者的回顾性队列研究,发现糖尿病患者感染的风险比非糖尿病患者高 4.027 倍。Kong 和 Kunutsor等[24]对 TKA 或 THA 后 PJI 危险因素的 Meta 分析证明,糖尿病与 TKA 或 THA 后 PJI 相关。来自中国的临床研究也有类似的结论,上海第九人民医院的 Wu等[23]进行的病例对照研究显示糖尿病患者较非糖尿病患者 PJI 的风险增加 (OR=5.47;95%CI,1.77~16.97 )。与此不同的是,Bozic 等[16]通过病例对照研究,得出糖尿病与 THA 后 PJI 关系无统计学意义的结论。Maradit 等[2]进行了包含 20 171 例 TJA 的回顾性队列研究,发现调整了 BMI、手术类型、ASA 评分、手术时间后,糖尿病与 PJI 不再具有显著相关性。本研究发现,相较于非糖尿病患者,糖尿病患者发生假体感染的概率增加了 1.8 倍,进一步发现糖尿病患者及糖耐量异常患者发生 PJI 风险是血糖正常患者的 7.2 倍和 5.6 倍。
围手术期血糖值为糖尿病患者围手术期血糖控制的直观指标,反映血糖控制的实时水平。Hwang等[28]回顾性分析了 3112 例 TKA 患者,发现空腹血糖 FBG>11.1 mmol / L 可以作为糖尿病患者 TKA 术后感染的预测因素。同时 Jämsen 等[29]发现无论是否糖尿病患者,随着术前空腹血糖升高,PJI 发生率均有明显的提升。Maradit Kremers 等[2]也发现术前 1 天血糖值升高对于糖尿病患者和非糖尿病患者术后 PJI 风险升高均相关。与此同时,Boris 等发现糖尿病患者术后第 1 天清晨高血糖 ( BG>11.1 mmol /L ) 增加的 PJI 的风险超过 2 倍。而即使患者无糖尿病,如果术后第 1 天空腹血糖>7.8 mmol / L,感染的几率将增加 3 倍[30]。本研究同样发现糖尿病患者及糖耐量异常患者发生 PJI 风险均会显著提高。因此糖尿病患者实现最佳的血糖控制是很重要的,同时,糖耐量异常患者围手术期血糖控制也值得重视。围手术期高血糖可能比糖尿病本身对术后 PJI的发生有更强的预测性,应努力保持在整个围手术期中充分控制血糖水平。而最佳的血糖状态水平,尚未确立,还须进一步研究提供更多的证据,笔者推荐将糖尿病及糖耐量异常患者的术前及术后血糖尽量控制在正常血糖水平,即空腹血糖<6.1 mmol /L,餐后 2 h 血糖<7.8 mmol / L。进一步分层分析发现双侧同时行人工关节置换患者组中,糖尿病患者PJI 发病率明显高于仅行单侧人工关节置换组患者,因此对于糖尿病患者应谨慎评估术后感染的风险,尽量避免双侧同时行 TJA。
相较于前人对于糖尿病和 PJI 相关性的研究报道,本研究有如下优势。首先,这是第一个针对中国人糖尿病和 PJI 发病率相关性的队列研究;其次,引入糖耐量异常组,这可以更全面地了解患者血糖异常和 PJI 的相关性。同时,本次研究的不足是:首先,病例数相对较小,降低了本研究结论的普遍性。其次,由于本研究为回顾性研究,部分临床资料不足,如血糖控制情况及 BMI 等信息收集不全,这将会降低本次研究结论的可靠性。希望有越来越多的针对中国人的此类研究,还须进行大量的前瞻性研究,完全随机临床试验来进一步证实糖尿病及血糖异常与 TJA 术后的 PJI 发生率的关系。
[1]Guariguata L, Whiting DR, Hambleton I, et al. Global estimates of diabetes prevalence for 2013 and projections for 2035[J].Diabetes Res Clin Pract, 2014, 103(2):137-149.
[2]Maradit Kremers H, Lewallen LW, Mabry TM, et al. Diabetes mellitus, hyperglycemia, hemoglobin A1C and the risk of prosthetic joint infections in total hip and knee arthroplasty[J].J Arthroplasty, 2015, 30(3):439-443.
[3]O’Toole P, Maltenfort MG, Chen AF, et al. Projected increase in periprosthetic joint infections secondary to rise in diabetes and obesity[J]. J Arthroplasty, 2016, 31(1):7-10.
[4]Pruzansky JS, Bronson MJ, Grelsamer RP, et al. Prevalence of modifiable surgical site infection risk factors in hip and knee joint arthroplasty patients at an urban academic hospital[J].J Arthroplasty, 2014, 29(2):272-276.
[5]Toor AS, Jiang JJ, Shi LL, et al. Comparison of perioperative complications after total elbow arthroplasty in patients with and without diabetes[J]. J Shoulder Elbow Surg, 2014, 23(11):1599-1606.
[6]Neuman D, Grzebieniak Z. Surgical site infection- the authors’own prospective research[J]. Pol Przegl Chir, 2014, 86(1):26-32.
[7]Namba RS, Inacio MCS, Paxton EW. Risk factors associated with deep surgical site infections after primary total knee arthroplasty[J]. J Bone Joint Surg Am, 2013, 95(9):775-782.
[8]Adams AL, Paxton EW, Wang JQ, et al. Surgical outcomes of total knee replacement according to diabetes status and glycemic control, 2001 to 2009[J]. J Bone Joint Surg Am, 2013,95(6):481-487.
[9]Maoz G, Phillips M, Bosco J, et al. The otto aufranc award:modifiable versus nonmodifiable risk factors for infection after hip arthroplasty[J]. Clin Orthop Relat Res, 2015, 473(2):453-459.
[10]Rezapoor M, Parvizi J. Prevention of periprosthetic joint infection[J]. J Arthroplasty, 2015, 30(6):902-907.
[11]Kapadia BH, Berg RA, Daley JA, et al. Periprosthetic joint infection[J]. The Lancet, 2016, 387(10016):386-394.
[12]Kurtz SM, Lau E, Watson H, et al. Economic burden of periprosthetic joint infection in the united states[J].J Arthroplasty, 2012, 27(8):61-65.
[13]Poultsides LA, Ma Y, Della Valle AG, et al. In-hospital surgical site infections after primary hip and knee arthroplastyincidence and risk factors[J]. J Arthroplasty, 2013, 28(3):385-389.
[14]Chrastil J, Anderson MB, Stevens V, et al. Is hemoglobin a1c or perioperative hyperglycemia predictive of periprosthetic joint infection or death following primary total joint arthroplasty[J]?J Arthroplasty, 2015, 30(7):1197-1202.
[15]Kunutsor SK, Whitehouse MR, Blom AW, et al. Patient-related risk factors for periprosthetic joint infection after total joint arthroplasty: a systematic review and meta-analysis[J]. PLOS ONE, 2016, 11(3):e150866.
[16]Bozic KJ, Ward DT, Lau EC, et al. Risk factors for periprosthetic joint infection following primary total hip arthroplasty: a case control study[J]. J Arthroplasty, 2014, 29(1):154-156.
[17]Jämsen E, Nevalainen P, Eskelinen A, et al. Obesity, diabetes,and preoperative hyperglycemia as predictors of periprosthetic joint infection[J]. J Bone Joint Surg Am, 2012, 94(14):e101.
[18]Iorio R, Williams KM, Marcantonio AJ, et al. Diabetes mellitus,hemoglobin A1C, and the incidence of total joint arthroplasty infection[J]. J Arthroplasty, 2012, 27(5):726-729.
[19]Bozic KJ, Kurtz SM, Lau E, et al. The epidemiology of revision total knee arthroplasty in the united states[J]. Clin Orthop Relat Res, 2010, 468(1):45-51.
[20]Everhart JS, Altneu E, Calhoun JH. Medical comorbidities are independent preoperative risk factors for surgical infection after total joint arthroplasty[J]. Clin Orthop Relat Res, 2013,471(10):3112-3119.
[21]Parvizi J, Cavanaugh PK, Diaz-Ledezma C. Periprosthetic knee infection: ten strategies that work[J]. Knee Surg Relat Res,2013, 25(4):155-164.
[22]Bozic KJ, Lau E, Kurtz S, et al. Patient-related risk factors for postoperative mortality and periprosthetic joint infection in medicare patients undergoing TKA[J]. Clin Orthop Relat Res,2012, 470(1):130-137.
[23]Wu CL, Qu XH, Liu FX, et al. Risk factors for periprosthetic joint infection after total hip arthroplasty and total knee arthroplasty in chinese patients[J]. PLoS One, 2014, 9(4):e95300.
[24]Kong L, Cao J, Zhang Y, et al. Risk factors for periprosthetic joint infection following primary total hip or knee arthroplasty:a meta-analysis[J]. Int Wound J, 2016, 14(3):529-536.
[25]Chun Y, Lee S, Lee S, et al. Clinical implication of diabetes mellitus in primary total hip arthroplasty[J]. Hip Pelvis, 2014,26(3):136-142.
[26]Mm D, Pf C. Obesity is a major risk factor for prosthetic infection after primary hip arthroplasty[J]. Clin Orthop Relat Res, 2008, 466(1):153-158.
[27]Bozic KJ, Ward DT, Lau EC, et al. Risk factors for periprosthetic joint infection following primary total hip arthroplasty: a case control study[J]. J Arthroplasty, 2014, 29(1):154-156.
[28]Hwang JS, Kim SJ, Bamne AB, et al. Do glycemic markers predict occurrence of complications after total knee arthroplasty in patients with diabetes[J]? Clin Orthop Relat Res, 2015,473(5):1726-1731.
[29]Jämsen E, Nevalainen P, Kalliovalkama J, et al. Preoperative hyperglycemia predicts infected total knee replacement[J]. Eur J Intern Med, 2010, 21(3):196-201.
[30]Boris Mraovic MDDS. Perioperative hyperglycemia and postoperative infection after lower limb arthroplasty[J].J Diabetes Sci Technol, 2011, 5(2):412-418.