Tumor-feeding artery diameter reduction is associated with improved short-term effect of hepatic arterial infusion chemotherapy plus lenvatinib treatment
2022-07-30WuDDHeXFTianPengChenCLLiuXHPangHJ
Wu DD, He XF, Tian C, Peng P, Chen CL, Liu XH, Pang HJ
Abstract
Key Words: Hepatocellular carcinoma; Hepatic arterial infusion chemotherapy; Lenvatinib; Short-term effect;Hepatic artery; Vessel diameter
lNTRODUCTlON
Hepatocellular carcinoma (HCC) is one of the most common malignant tumors, with 850000 new cases reported per year worldwide[1,2]. In total, 70%-80% of patients with HCC in China are ineligible for surgical resection at the time of onset[3]. Recently, hepatic arterial infusion chemotherapy (HAIC) has been increasingly used to treat patients with unresectable HCC (uHCC) in Asian countries[4,5]. HAIC is recommended as a major treatment option in patients with intermediate and advanced HCC by current Japanese and Chinese guidelines[6].
Lenvatinib is an oral multi-target tyrosine kinase inhibitor (TKI) with antiangiogenic effects. Previous studies demonstrated the survival benefit of lenvatinib plus HAICvslenvatinib alone in patients with advanced HCC[7]. This combination therapy often requires 6-8 cycles, and early assessment of the antitumor response appears essential for both patients and physicians[8].
Recently, a clinical study demonstrated that the diameters of hepatic arteries are significantly reduced after TKI therapy[9]. Since the early imaging response is often associated with survival benefits, it should be clarified whether the changes in hepatic vessel diameters are related to the efficacy of HAIC combined with lenvatinib. As a result, we conducted a retrospective study of patients with uHCC treated with HAIC plus lenvatinib. The aim of this study was to: (1) Explore the changes in hepatic arteries after combination treatment; and (2) Determine the relationship between the hepatic artery changes and early therapeutic effects.
MATERlALS AND METHODS
Patient eligibility
This was a single-center, retrospective analysis of data from 67 patients with uHCC treated at our institution from January 2019 to October 2020. Approval for the study was obtained from the local ethics committee on human research. The HCC diagnosis was based on the findings of pathological, imaging,and clinical assessments using the European Association for the Study of the Liver criteria[10]. Eligible patients were those aged 18 years or older with uHCC (including patients with large/multifocal HCC and/or with vascular invasion and extrahepatic spread) who received HAIC plus lenvatinib as an initial treatment. Patients who underwent transcatheter arterial chemoembolization or received other TKIs before combination therapy were excluded. Enrolled patients who discontinued treatment during the follow-up period were also excluded.
Treatments
HAIC was repeated at an interval of 3 wk in enrolled patients in our hospital. A catheter was initially advanced into the celiac or superior mesenteric artery for digital subtraction angiography from the femoral artery; then, a microcatheter was left in the tumor-feeding artery (TFA) for subsequent treatment.
The patients received the following regimen for HAIC through the indwelling microcatheter connected to an artery infusion pump in the ward: oxaliplatin 85 mg/m2administered intraarterially for 2 h, leucovorin 400 mg/m2administered intraarterially for 1 h, and 5FU 400 mg/m2intra-arterial bolus injection on day 1, followed by 5FU 2400 mg/m2continuous arterial infusion for 46 h. Three days after the first HAIC course, patients began to take lenvatinib (Eisai, Tokyo, Japan) orally at the recommended doses of 12 mg/day for patients weighing ≥ 60 kg and 8 mg/day for patients weighing < 60 kg[11].Dose adjustment or termination of lenvatinib therapy was allowed when drug-related adverse events(AEs) occurred. Discontinuation of the combination treatment was also allowed for potentially fatal AEs, clinical tumor progression, or the need for conversion therapy.
Evaluations and measurement
Therapeutic responses after 1, 3, and 6 mo of combination treatment were assessed according to the modified Response Evaluation Criteria in Solid Tumors using CT (Philips Brilliance iCT; Philips Medical Systems, Best, the Netherlands) images. Treatment responders were defined as patients with a complete response (CR) or partial response (PR). Non-responders were defined as patients with stable disease(SD) or progressive disease (PD). AEs were assessed using the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0[12].
Both the measurement of artery diameters and the evaluation of therapeutic efficacy were individually conducted by two physicians with experience in gastroenterological diagnostics, and differences were resolved by a more experienced physician.
Immunohistochemistry
Tumor angiogenesis was evaluated by measuring microvessel density (MVD) after staining using an anti-CD34 antibody. Punch biopsy samples were obtained from tumor lesions before and 1 mo after the start of HAIC plus lenvatinib therapy. The tumor samples were fixed in 10% formalin and embedded in paraffin. After routine laboratory procedures, immunohistochemistry was performed to detect the expression of CD34 (endothelial cell marker) through the avidin-biotin-peroxidase complex[14,15].MVD was measured at × 100 magnification in five regions of interest using a light microscope. All endothelial cells, including individual cells and grouped cells, were counted as a single vessel if they were separated from the surrounding tumor and other connective tissues[16].
Statistical analysis
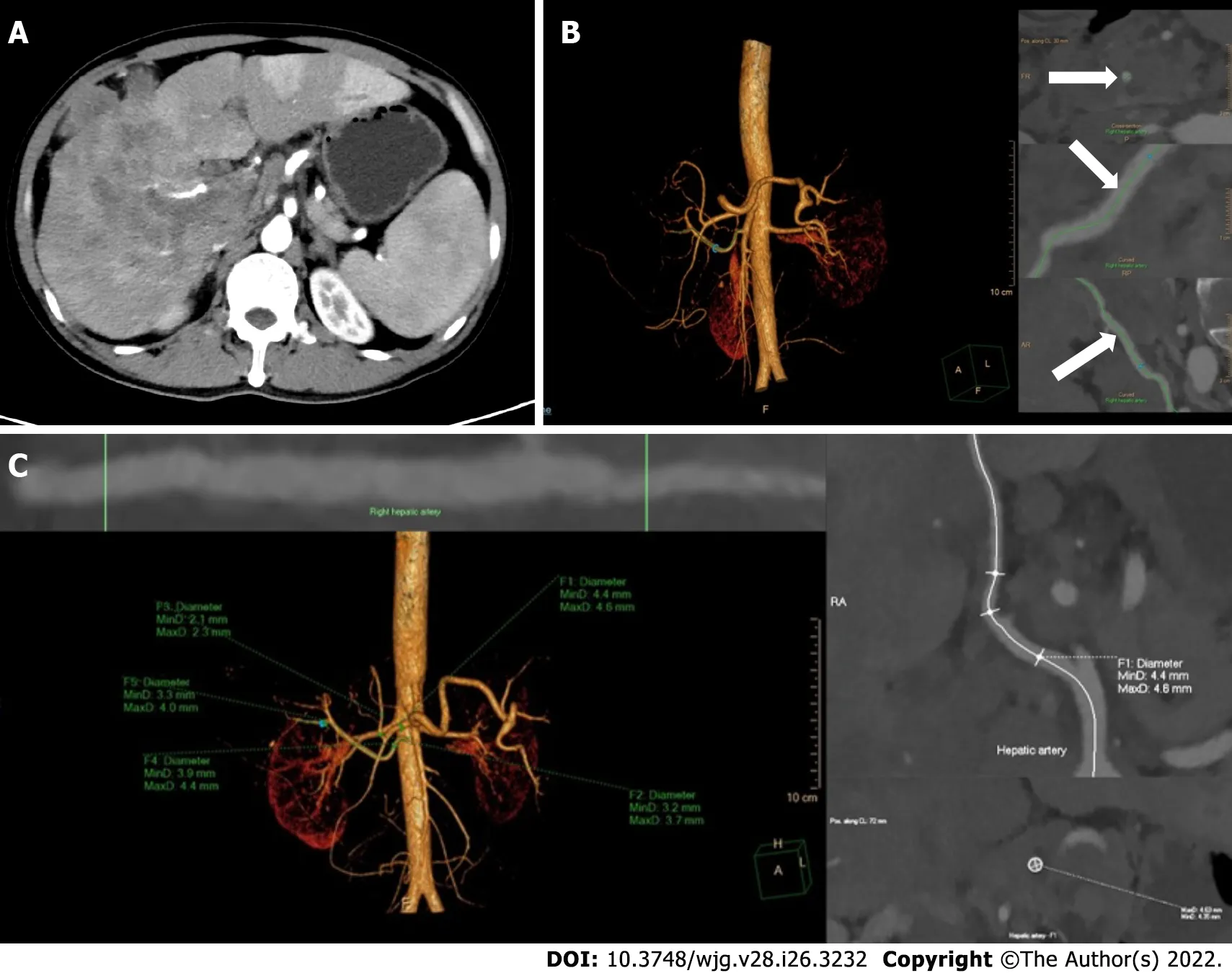
Figure 1 Reconstruction and measurement of the hepatic arteries. A: The thickest branch of tumor-feeding arteries generated from the right hepatic artery; B: Three-dimensional reconstruction of hepatic arteries in an image post-processing workstation and the adjustment of center line (arrows) on multiple layers;C: The hepatic artery diameters are measured automatically by drawing the region of interest. F1-5, the opening of the common hepatic artery, the proper hepatic artery, the left hepatic artery, the right hepatic artery and the tumor-feeding artery.
Statistical analyses were performed using IBM SPSS Statistics 26.0. The measurement data were presented as the mean ± SD, andP< 0.05 indicated statistical significance. Considering the loss to follow-up, the changes in the artery diameters were compared using the mixed linear model for repeated measured data, and follow-up pairwise comparison was conducted among the three periods.The independent-samplest-test was used to analyze the changes in MVD. Receiver-operating characteristic (ROC) analysis was used to evaluate the changes in the diameter of all hepatic arteries to differentiate between responders and non-responders and identify the cutoff values. The cutoff was calculated for any factors that were statistically significant in the ROC analysis, which were candidates for univariate and multivariable logistic regression analyses with baseline data.
RESULTS
Participant characteristics
During the study period, patients meeting the inclusion criteria were followed up for 6 mo after the start of the combination treatment. The study population was predominantly male (59/67, 88.1%), and most of the enrolled patients were infected with hepatitis B virus (53/67, 79.1%). In total, 45 (67.2%) patients were estimated to have Child-Pugh stage A liver function, and 22 (32.8%) patients were categorized as Child-Pugh stage B. Portal vein tumor thrombosis was diagnosed in 44 (65.7%) patients, hepatic vein tumor thrombus in 17 (25.4%) patients, and extrahepatic spread occurred in 13 (19.4%) patients. The characteristics of the patients are summarized in Table 1.
Treatment-related AEs
There were no treatment-related deaths in our study. According to CTCAE, grade 1-2 events were observed in 37 patients (55.2%) and grade 3 events in 2 (3.0%) patients, whereas no grade ≥ 4 AEs occurred. The most common grade 1-2 events were abdominal pain (17/67, 25.4%), fever (8/67, 11.9%),and transient nausea and vomiting (8/67, 11.9%). The grade 3 events were liver dysfunction and decreased leukocyte counts, both of which normalized after treatment.
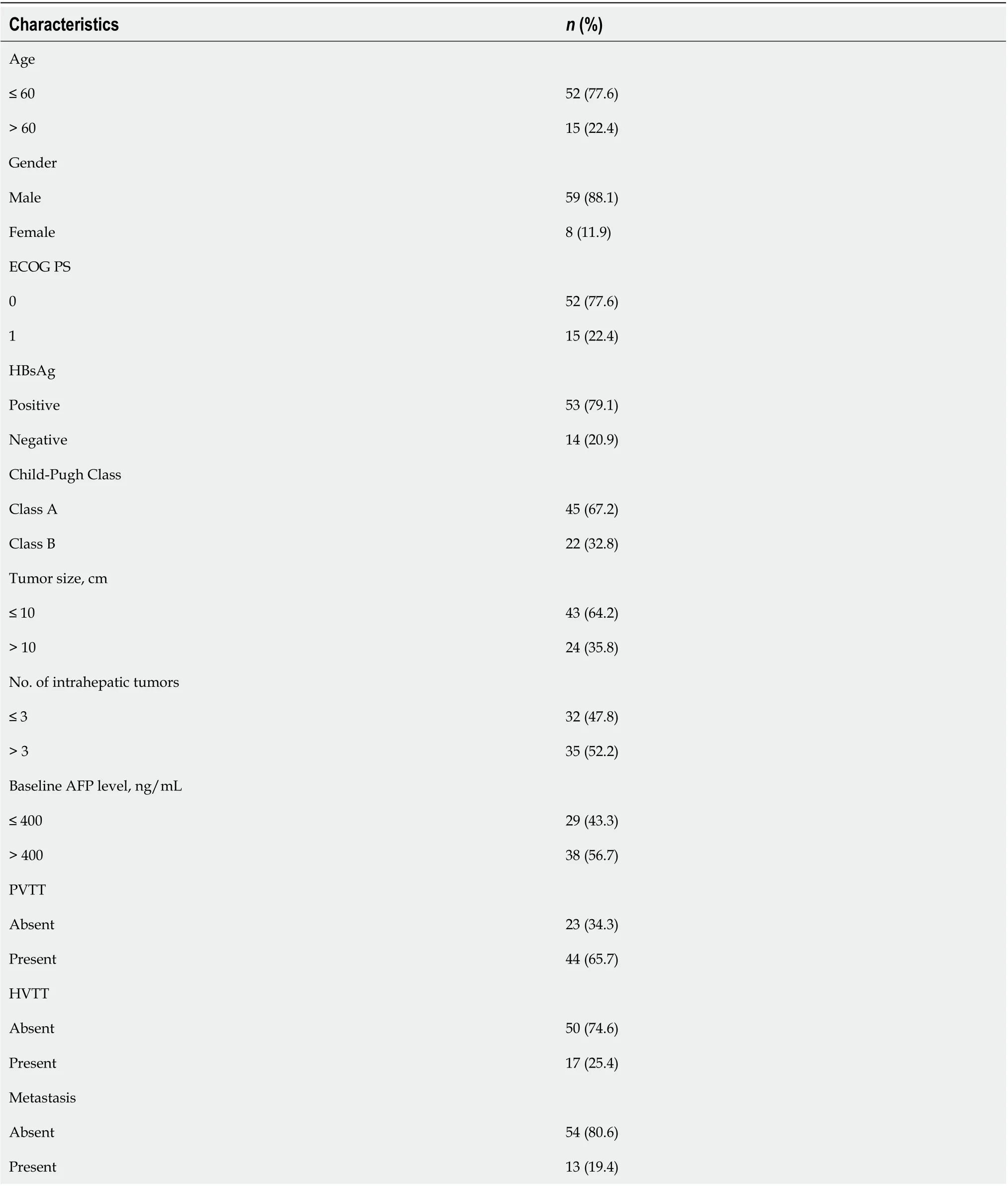
Table 1 The baseline characteristics of patients
Efficacy
Five patients missed the 3-mo imaging evaluation, and 11 patients missed the 6-mo evaluation because of loss to follow-up. In total, 46, 41, and 24 patients were classified as responders (CR + PR) after 1, 3,and 6 mo of treatment, respectively, whereas the numbers of non-responders (SD + PD) at these time points were 21, 21, and 32, respectively. The overall response rates (ORR) in this study at 1, 3, and 6 mo were 68.7%, 66.1%, and 42.9%, respectively. Eight patients received downstaging therapy within 1 year after treatment, of which six patients underwent hepatectomy and the other two patients underwent radiofrequency ablation.
Artery diameters
Vessel diameters were measured in all patients before treatment and after 1 mo of treatment, whereas six patients missed the 2-month measurement. After 1 and 2 mo of treatment, all vessel diameters had gradually decreased compared with the baseline (P< 0.001), but the difference in vessel diameters between 1 and 2 mo was not significant (P> 0.05, Figure 2). According to the ROC analysis, the change in the TFA diameter was significantly different between the responders and non-responders at 1, 3, and 6 mo (P< 0.001,P= 0.004, andP= 0.023, respectively), and the corresponding cutoff values were -0.169,-0.169, and -0.264, respectively. Meanwhile, there were no significant differences in the diameters of other hepatic arteries between the groups (Table 2). Considering the unclear clinical meaning of continuous changes in vessel diameters, the change in the TFA diameter was classified as reduced or unchanged based on the cutoff values.
The results of the univariate and multivariable logistic regression analyses of tumor response are listed in Table 3. According to the multivariable analysis, the change in the TFA diameter was an independent factor for the efficacy of HAIC plus lenvatinib after 1 [odds ratio (OR) = 0.12; 95%confidence interval (CI): 0.03-0.43;P= 0.001], 3 (OR = 0.06; 95%CI: 0.01-0.29;P= 0.001), and 6 mo (OR =0.14; 95%CI: 0.04-0.47;P= 0.002) of treatment. Other independent factors included the alpha-fetoprotein level (OR = 0.17; 95%CI: 0.04-0.73;P= 0.018) at 1 mo and tumor size (OR = 7.65; 95%CI: 1.36-42.88;P=0.021) at 3 mo.
式中,Dxx为纵向弥散系数主值;Dyy为横向弥散系数主值;Dzz为横向弥散系数主值;c为溶质浓度,mol/l;u为实际平均流速,m/d。
MVD
The MVD of tumor lesions after the administration of lenvatinib was robustly smaller than that before treatment, suggesting that angiogenesis was strongly suppressed by lenvatinib (P< 0.001, Figure 3).
DlSCUSSlON
In the present study, significant shrinkage of hepatic arteries was observed in patients with uHCC after 1 mo of HAIC plus lenvatinib therapy for the first time. We also confirmed that the morphological change in the TFA was closely related to the tumor response after 1, 3, and 6 mo of combination treatment, and this change was an independent factor for improved short-term therapeutic efficacy.These findings would be of great significance to physicians for evaluating the effectiveness of this combination therapy earlier in the course of treatment and altering the treatment plan as needed.
Hepatic arteries were shown to be markedly thin following TKI treatment, and Chenet al[17]attributed these morphological changes to the anti-angiogenic effect of targeted drugs. Notably,lenvatinib more effectively suppresses angiogenesis and inhibits tumor growth than sorafenib by targeting both vascular endothelial growth factor (VEGF) and fibroblast growth factor[18,19]. In our study, shrinkage of hepatic vessels was observed early after the start of HAIC plus lenvatinib therapy,and the powerful antiangiogenic effect of lenvatinib was proven by the decrease in the MVD of the tumor lesions. Meanwhile, anti-VEGF therapies can reverse vessel abnormalities and improve the tumor microenvironment[20]. The decline in local tumor perfusion secondary to the decrease in tumor capillaries and the “normalization hypothesis” may be the main reasons for the conspicuous reduction of hepatic arteries with the combination regimen.
The efficiency of HAIC combined with lenvatinib for intermediate and advanced HCC has been confirmed in previous studies[21,22]. In this study, the ORR reached 68.7%, 66.1%, and 42.9% at 1, 3,and 6 mo, and conversion therapy was achieved in eight patients, which further verified the effectiveness of the combination therapy. Thus, it was necessary to explore the mechanism of action of this combination therapy. A reduction in hepatic artery diameters was observed in most patients in the present study. Kuordaet al[23] also reported that local tumor perfusion declined significantly after oral lenvatinib administration. These findings illustrated that lenvatinib reduces the tumor blood supply after combination therapy. Meanwhile, HAIC has the advantage of achieving high local concentrations in the tumor during arterial infusion[24]. According to the pharmacokinetic characteristics of the intraarterial infusion[25], a decrease in tumor blood flow can increase the dose of the drug in the target organ, thus enhancing the antitumor effect of HAIC. Furthermore, the normalization and improved functionality of tumor vessels including reduced hypoxia, reduced vascular leakage, and improved vascular permeability can improve the delivery of local chemotherapeutic drugs in tumors[26,27]. The increased drug accumulation in the target organ often results in improved therapeutic efficacy. Since the combined therapy could improve the therapeutic effect, it may also expand the scope of HAIC, which is limited to patients with HCC and multinodule lesions or vascular invasion.
In clinical practice, HAIC often requires 6-8 courses. Moreover, repetitive and inefficient treatment is harmful to patients with uHCC. Therefore, early evaluation of the treatment response is of great significance. In this study, we found that the reduction in the TFA diameter after combination therapy was an independent factor for improved therapeutic efficacy within 6 mo. The morphological change in the TFA is easy to observe during HAIC, and it can help in estimating the early therapeutic effect. Since an improved short-term effect often results in a good prognosis, the observation on thinning of the TFA is significant and more practical for patients with uHCC who are receiving HAIC plus lenvatinib.
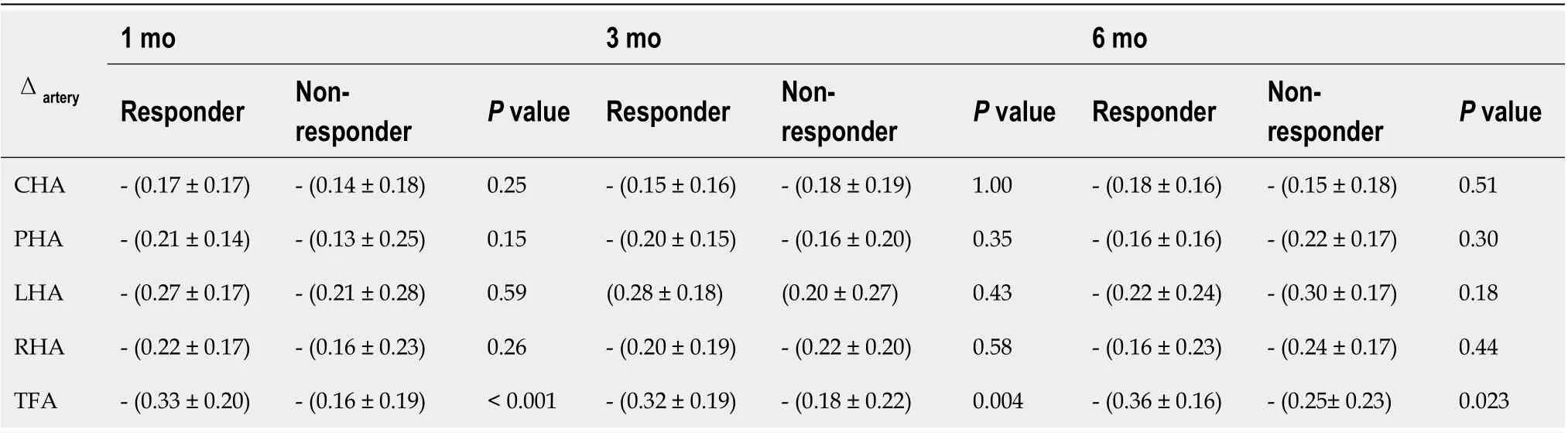
Table 2 Receiver-operating characteristic analysis for antitumor response
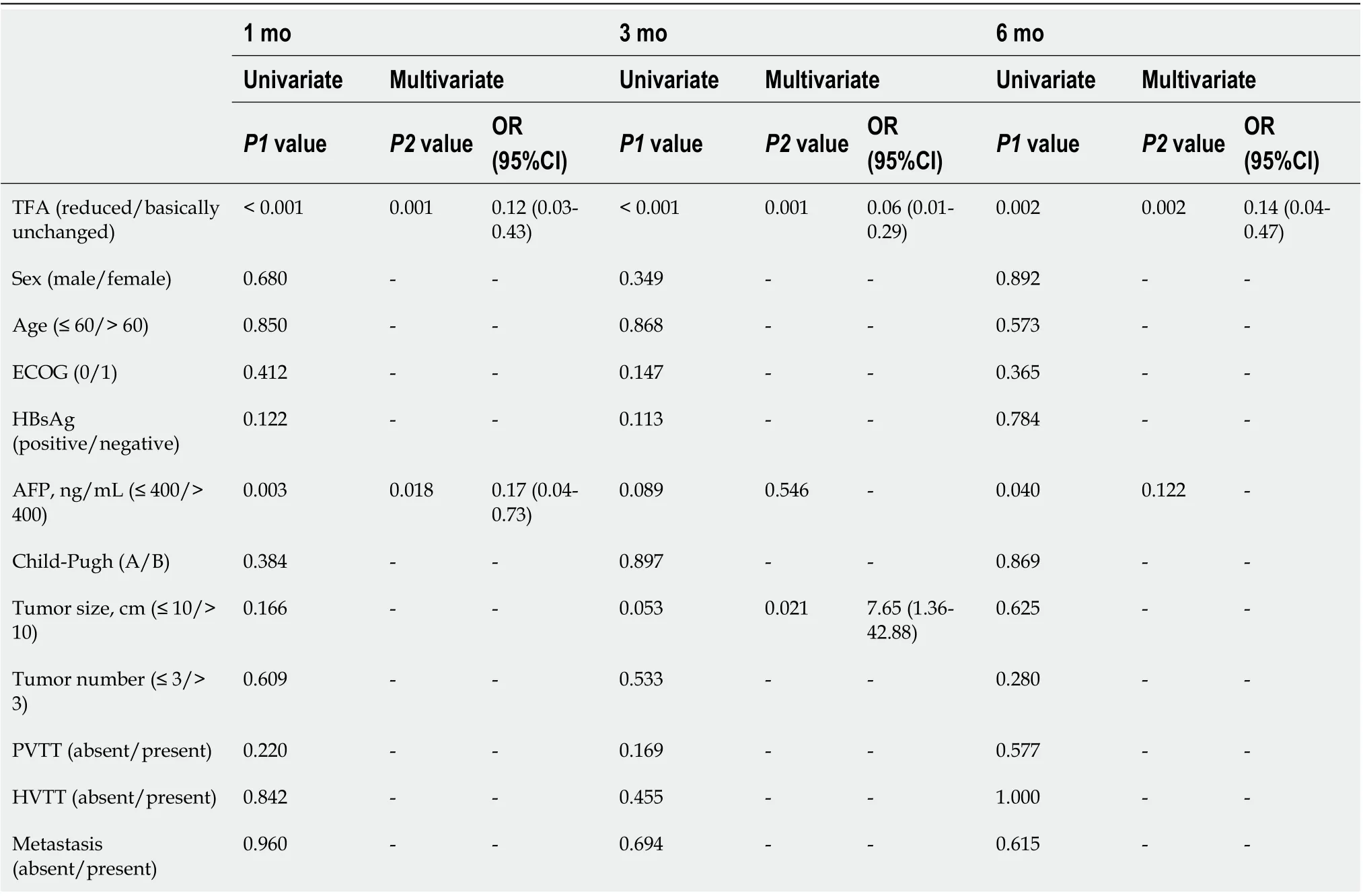
Table 3 Univariate and multivariate logistic regression analysis for efficacy of treatment with hepatic arterial infusion chemotherapy plus lenvatinib
The present study had some limitations. This was a single-center retrospective study, and the sample size was small.
CONCLUSlON
In conclusion, lenvatinib can reduce the diameters of hepatic arteries and thus enhance the effect of HAIC. Shrinkage of the TFA after HAIC plus lenvatinib therapy was linked to improved short-term outcomes in patients with uHCC.
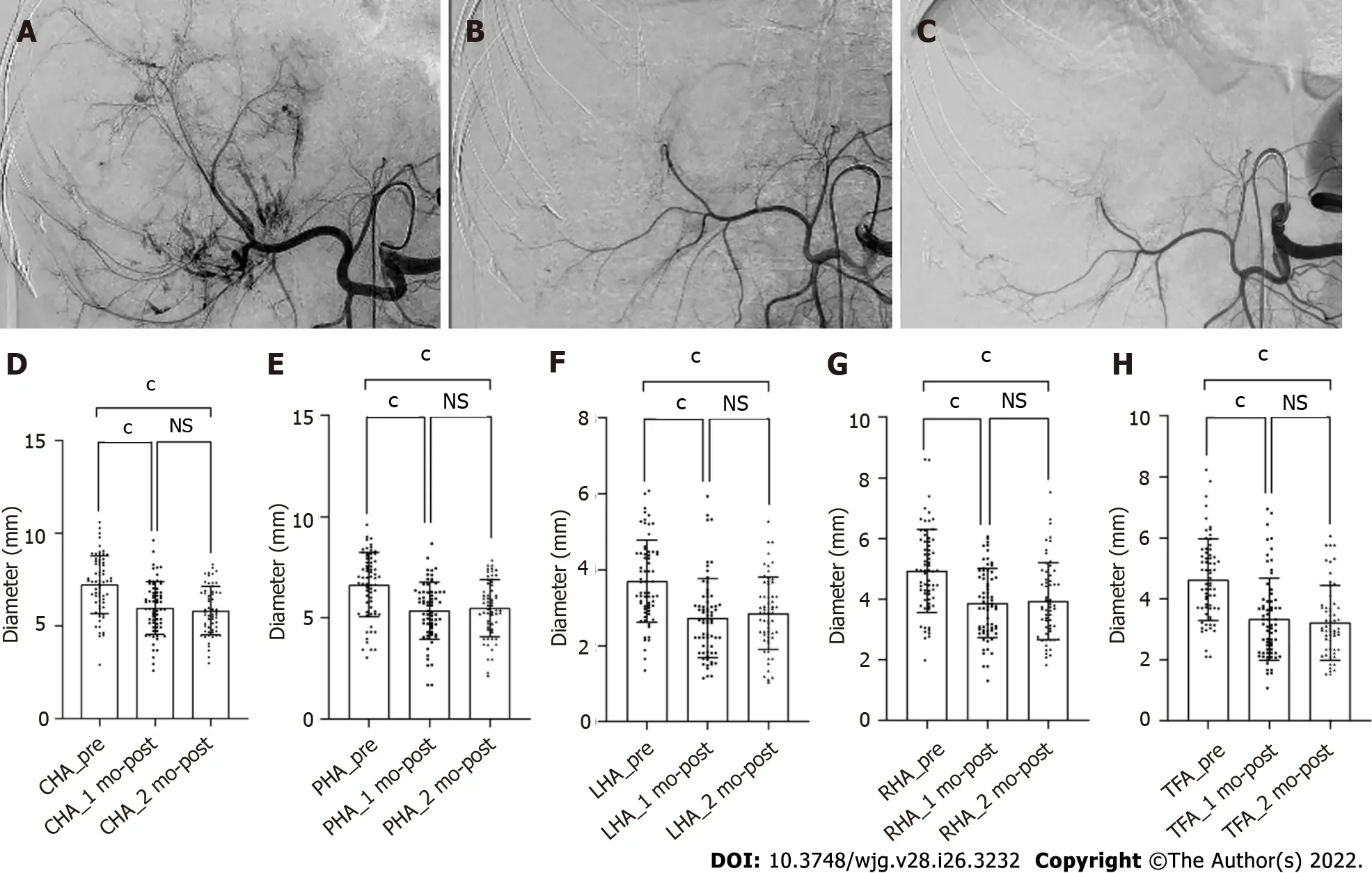
Figure 2 Shrinkage of the hepatic artery diameters in patient with unresectable hepatocellular carcinoma after treatment with hepatic arterial infusion chemotherapy plus lenvatinib. A-C: Digital subtraction angiography performed before treatment (A), after 1 (B) and 2 (C) mo of treatment;D-H: Bars represent the vessel diameters before treatment, at 1 and 2 mo after treatment. P-values are calculated using the mixed linear model for repeated measured data. cP < 0.001. NS: Not significant (P > 0.05); CHA: Common hepatic artery; PHA: Proper hepatic artery; LHA: Left hepatic artery; RHA: Right hepatic artery; TFA: Tumor-feeding artery.
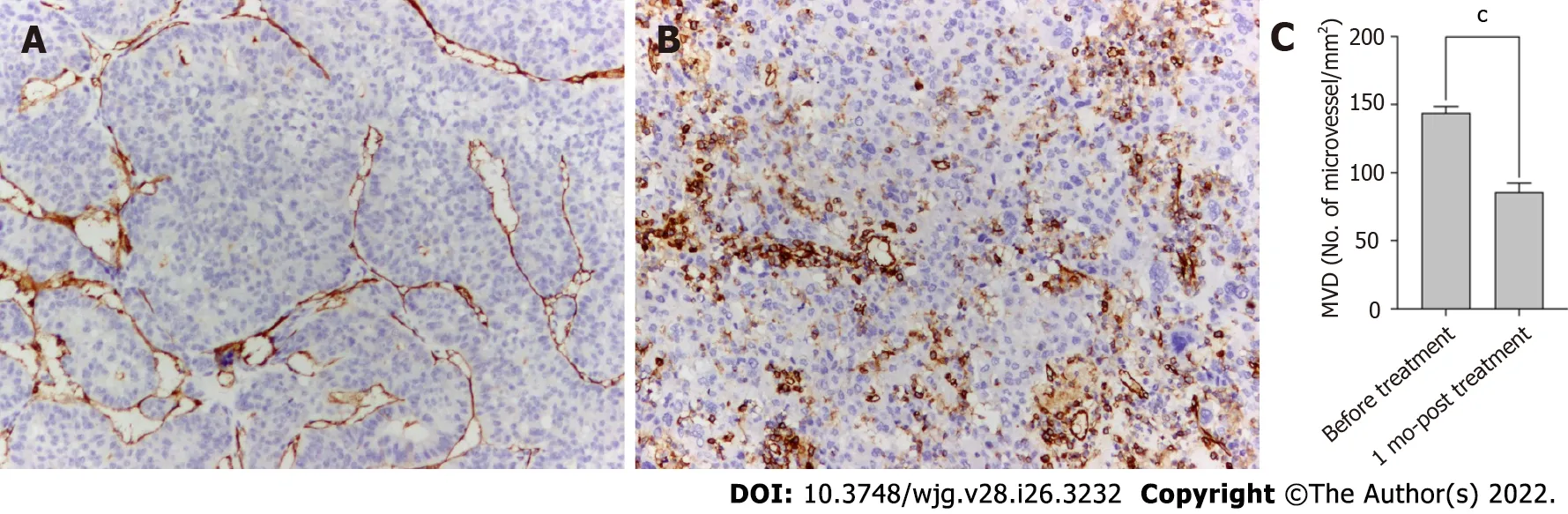
Figure 3 Anti-angiogenic activities of lenvatinib in tumor lesions. A and B: The microvessels in the tumor lesion collected before (A) and after 1 mo (B)of treatment with lenvatinib are stained with anti-CD34 antibody (× 100); C: Bars represent the microvessel density that decreased sharply after administration of lenvatinib. Data are presented as means ± SD. cP < 0.001 vs before treatment. MVD: Micro-vessel density.
ARTlCLE HlGHLlGHTS
Research objectives
To investigate the relationship between hepatic artery diameters reduction and the short-term efficacy of HAIC plus lenvatinib.
Research methods
Sixty-seven patients with uHCC receiving HAIC plus lenvatinib were analyzed retrospectively. The modified Response Evaluation Criteria in Solid Tumors was used to assess the antitumor response after 1, 3, and 6 mo of treatment. The measurement of hepatic artery diameters before treatment and after 1 and 2 mo of treatment were conducted in a computed tomography image post-processing workstation.Meanwhile, the changes in tumor capillaries were also examined on pathological specimens before and after 1 mo of treatment.
Research results
All the hepatic artery diameters and the microvessel density in the tumor lesions were significantly decreased after the combination treatment (allP< 0.001). Shrinkage of the tumor-feeding artery (TFA)was significantly associated with the antitumor response after 1, 3, and 6 mo of treatment (P< 0.001,P=0.004, andP= 0.023, respectively) and an independent factor for treatment efficacy (P= 0.001,P= 0.001,andP= 0.002 and 1, 3, and 6 mo, respectively).
Research conclusions
The retrospective study demonstrated that the shrinkage of the TFA diameter was closely related to improved short-term efficacy of treatment with HAIC plus lenvatinib for the first time.
Research perspectives
We believe the findings in this paper will be of interest to the researchers in uHCC. Further, prospective randomized multicenter trials are needed to confirm the relationship between the morphological change in TFA and the early therapeutic effect of uHCC treatment.
ACKNOWLEDGEMENTS
All authors are grateful to Dr. Fan XY for assisting with the reconstruction of the CT images.
FOOTNOTES
Author contributions:Wu DD and Pang HJ designed this study; Wu DD, Tian C, and Chen CL performed the reconstruction and measurement; Wu DD, Liu XH, and Pang HJ analyzed the data; Peng P collected the clinical data;Wu DD wrote the paper; He XF and Pang HJ made critical revisions to the paper; all authors approved the publication of the paper.
lnstitutional review board statement:The research was conducted in accordance with the 1975 Declaration of Helsinki and approved by the medical ethics committee of Nanfang Hospital, Southern Medical University.
lnformed consent statement:The requirement for informed consent was waived owing to the retrospective nature of the study.
Conflict-of-interest statement:There was no conflict of interest to disclose.
Data sharing statement:No additional data are available.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:De-Di Wu 0000-0001-8409-9770; Xiao-Feng He 0000-0001-8255-1874; Chen Tian 0000-0003-4260-290X;Peng Peng 0000-0001-9864-0580; Chuan-Li Chen 0000-0001-7610-5966; Xue-Han Liu 0000-0002-8966-7172; Hua-Jin Pang 0000-0001-7367-5701.
S-Editor:Yan JP
L-Editor:A
P-Editor:Yan JP
杂志排行

World Journal of Gastroenterology的其它文章
- Involvement of Met receptor pathway in aggressive behavior of colorectal cancer cells induced by parathyroid hormone-related peptide
- Role of gadoxetic acid-enhanced liver magnetic resonance imaging in the evaluation of hepatocellular carcinoma after locoregional treatment
- Clinical implications and mechanism of histopathological growth pattern in colorectal cancer liver metastases
- Bifidobacterium infantis regulates the programmed cell death 1 pathway and immune response in mice with inflammatory bowel disease
- Impact of sodium glucose cotransporter-2 inhibitors on liver steatosis/fibrosis/inflammation and redox balance in non-alcoholic fatty liver disease
- Endoscopic techniques for diagnosis and treatment of gastro-entero-pancreatic neuroendocrine neoplasms:Where we are