Clinical features and risk factors of severely and critically ill patients with COVID-19
2022-03-07ChuZhangGFZhengYKZhongYGWenZengFuCYTongXLLongYFLiLiuYLChangZGXi
INTRODUCTION
Since the first report of coronavirus disease 2019 (COVID-19) in Wuhan, China, in December 2019, this highly infectious respiratory disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has spread rapidly throughout the world, posing a serious threat to global health. Similar to SARS-CoV, the novel SARSCoV-2 uses angiotensin converting enzyme II (ACE2) receptors to invade not only type II alveolar cells in the lung but also myocardial cells in the heart, proximal tubule cells in the kidney and other cells in organs with high ACE2 expression levels[1-4]. Several studies reported that a number of patients had rapid disease progression and died of acute respiratory distress syndrome and/or multiple organ failure[5-7].
According to the Chinese management guideline for COVID-19 (versions 1.0 through 7.0), the definition and classification of COVID-19 severity is divided into four levels: mild, moderate, severe and critical. The main parameters for classification are level of hypoxemia and progression of radiographic presentation[8]. Several studies have reported the mortality rates of different groups. In the latest Chinese Centers for Disease Control (CDC) report that included records from 44672 cases, patients with severe and critical disease accounted for 13.8% and 4.7% of confirmed cases,respectively; the crude case fatality rate among critically ill patients was 49%, and the fatality density was 0.325[9]. Feng[10] reported that the mortality rates of the moderate, severe and critically ill groups were 6.2%, 12.5% and 49.1%, respectively, in Hubei, and 0%, 0%, and 13.3%, respectively, outside of Hubei. Of 52 critically ill adult patients in the Yang[6] study, 32 (61.5%) had died at 28 d. The estimated mortality rates in the Li[5] study were 1.1% for patients with non-severe disease and 32.5%for patients with severe disease over an average of 32 d. Zhou[11] reported mortality rates of 0%, 18.2% and 79.2% for patients with moderate, severe and critically ill disease, respectively. Previous studies confirmed that older age, chronic disease, and D-dimer greater than 1 µg/L were important independent predictors of mortality from COVID-19.
However, the risk factors for patients with moderate-to-severe or severe-to-critical COVID-19 remain unclear. A comprehensive description of the clinical characteristics,laboratory changes, in addition to oxygen levels and radiographic examinations enable clinicians to provide more accurate prognoses and specific care which vary according to subclinical or latent severe cases. Here, we aim to explore the typical clinical characteristics and examination parameters of critically ill patients with COVID-19 at two campuses of Tongji Hospital affiliated with Huazhong University of Science and Technology in Wuhan, China.
鲁提辖道:“这个不妨事,俺自有道理。”便去身边出五两来银子,放在桌上,看着史进道:“洒家今日不曾多带得些出来;你有银子,借些与俺,洒家明日便送还你。”史进道:“直甚么,要哥哥还!”去包裹里出一锭十两银子放在桌上。鲁达看着李忠道:“你也借些出来与洒家。”李忠去身边出二两来银子。鲁提辖看了见少,便道:“也是个不爽利的人!
A.借助计算器或Excel。分别逐一计算各行、各列以及条件百分比,之后根据逐项算出的数据,在原有交叉分布表的基础上制作出包含百分比的二维表。在计算γ系数时,根据已知频数分布表可知:同序对数Ns=68×(36+13+41+10)+57×(13+10)+25×(41+10)+36×10=9746;异序对数Nd=16×(25+36+34+41)+57×(25+34)+13×(34+41)+36×34=7738,于是有γ系数为可看出“身份”与“态度”两个顺序变量几乎不相关。
MATERIALS AND METHODS
Study design and participants
In this retrospective study, we enrolled all inpatients who were hospitalized for COVID-19 from 1February to 8March 2020, at the B11 Zhongfaxincheng campus and E1-3 Guanggu campus of Tongji Hospital affiliated with Huazhong University of Science and Technology in Wuhan, China. These two campuses were designated hospitals treating mainly severely and critically ill patients, and according to the arrangement of the Chinese government, patients with mild to moderate COVID-19 were isolated from their families and communities and then transferred and admitted to Fangcang shelter hospitals[12]. All patients in our study were confirmed with throat swab specimens to extract viral RNA for laboratory confirmation of SARS-CoV-2 infection. The study was approved by the Research Ethics Commission of Beijing Hospital (2020BJYYEC-047-01), and the requirement for written informed consent was waived by the Ethics Commission for emerging infectious diseases.
能源效率不断提升,“十三五”、“十四五”、“十五五”期间,广东省单位GDP能耗分别下降21%、17%和15%,至2030年,单位GDP能耗降至0.31 tce/万元(2000年价),约为2005年的1/3,达到美国2013年水平。
Procedures
Epidemiological data, demographic data, clinical symptoms and outcomes, complications, laboratory examinations and imaging test information were extracted from electronic medical records, and clinical outcomes were followed until March 26, 2020.If data were missing from the medical records or clarification was needed, we obtained data by direct communication with attending doctors and other health-care providers.All data were checked by two researchers and two physicians from each campus.
当前,医疗机构的药学服务应该从“以药品为中心”转变为“以患者为中心”,从“以保障药品供应为中心”转变为“在保障药品供应的基础上,以重点加强药学专业技术服务、参与临床用药为中心”,而验票相关工作不该过多占用医疗机构日常工作时间,浪费其较多的人力物力。此外,纸质发票会占用医疗机构较大的场地空间,因此电子化验票平台无疑将会是未来发展的一个趋势,而且信息化验票能在一定程度上帮助医疗机构更快捷、更方便地开展验票工作。为此,卫生健康主管部门应积极创新监管方式,优化验票工作流程,运用便捷的信息化手段推动落实“两票制”政策。
According to COVID-19 severity defined by the Chinese management guideline for COVID-19 (version 7.0)[8], we categorized the patients into 3 groups, namely, the moderate group (level 2), severe group (level 3) and critically ill (level 4) group, to analyze the clinical features and high-risk factors of severe and critical COVID-19.
Definitions
The severity of COVID-19 (according to the Chinese management guideline for COVID- 19 (version 7.0) was classified as follows[8].
Mild (level 1): The patient had light clinical symptoms but no evidence of pneumonia on X-ray or computed tomography (CT) examination.
Moderate (level 2): The patient had fever and respiratory symptoms, and the X-ray or CT examination showed evidence of pneumonia.
Severe (level 3): Patients aged over 18 years who met the following conditions: (1)Shortness of breath, with a respiratory rate ≥ 30; (2) Resting-state oxygen saturation values from one finger of one arm of ≤ 93%; (3) Arterial partial pressure of oxygen(PaO)/fraction of inspired oxygen (FiO) ≤ 300 mmHg; and (4) Rapid progression of lesions over 50% within 24-48 h.
Critically ill (level 4): Patients aged over 18 years who met the following conditions:(1) Acute respiratory failure requiring mechanical ventilation support; (2) Shock; and(3) COVID-19 complicated by other organ failure and the need for critical care in the Intensive care unit.
Statistical analysis
EpiData 3.1 was used for the data collection and SPSS (version 22.0) for the analyses.Continuous variables are presented as the mean ± SD if they were normally distributed or the median (interquartile range, IQR) if they were not, and variables were compared by one-way ANOVA, the Mann-Whitneytest or Kruskal-Wallis test.Categorical variables are presented as(%) and were compared by thetest or Fisher’s exact test. A two-sided α of less than 0.05 was considered statistically significant. The high-risk factors for severe and critically ill COVID-19 were analyzed by logistic regression analysis. An ordinal logistic regression model was adopted and used with JMP15.0 software to explore potential risk factors associated with the severity of COVID-19. According to clinical significance, which was the most important measure, data completeness and the single-factor screening results of theanalysis were considered. Under clinician guidance, potential collinear variables were categorized to process the collinearity diagnosis by SPSS 22.0 (IBM Corp., Armonk,NY, United States). Timeline charts of laboratory parameters were plotted using GraphPad Prism version 8.0.
RESULTS
As of March 8, 126 patients with COVID-19 were included in this study, 67 from the B11 Zhongfaxincheng campus and 59 from the E1-3 Guanggu campus. There were 59 in the moderate group, 49 in the severe group, and 18 in the critically ill group.Although more than half of the infected patients in the severe and critically ill groups were men, there was no significant difference in sex between groups; however,compared with the moderate group, the difference became significant when we merged the severe and critically ill together (= 0.008). Men were more vulnerable to COVID-19.
The median age of the patients was 61.00 years (IQR 48.00-68.00), ranging from 24 years to 91 years. Patients in the critically ill group were significantly older than those in the moderate group (65.4454.76 years,0.019). The median time from onset of symptoms to first hospital admission was 8 d (IQR 3.00-14.00), and among the three groups, this duration was longest in the moderate group. The median time from onset of symptoms to COVID-19 Laboratory confirmation (throat swab samples) was 7.5 d (IQR 3.35-13.75), and there were no differences between groups (Table 1).
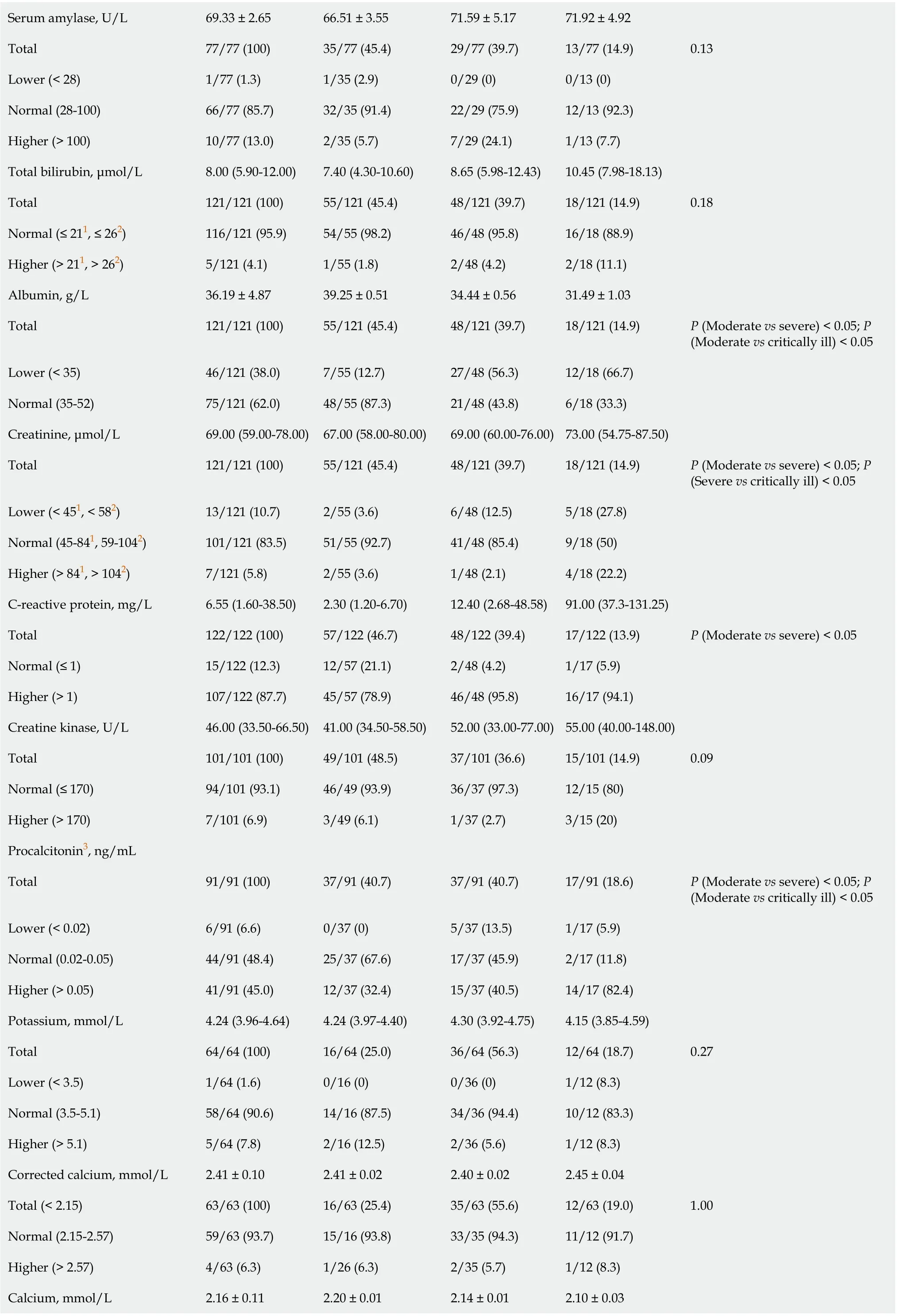
Chai[21] indicated that liver dysfunction in patients with COVID-19 might be induced by cholangiocyte damage rather than hepatocyte damage, which is consistent with our finding that elevated AST and decreased albumin were associated with progression to more severe disease. However, we did not find significant difference between groups in ALT and total bilirubin results. Further studies could investigate whether other causes might participate in liver injury, such as systemic inflammatory response or hypoxemia.


Among the 126 patients in the study, the most common symptoms at disease onset were fever [98 (77.8%)], cough [98 (77.8%)], shortness of breath [49 (38.9%)] and fatigue(43/67, 64.2%). Less common symptoms included expectoration, rigor, anorexia,myalgia, and nausea (Table 1). No significant differences in the symptoms at disease onset were found between groups (Table 1).
All patients had received radiographic examination in our study. Among 86 imaging diagnostic reports, patchy shadows were found in 45.3% and 44% of patients’early chest CT and X-ray reports, respectively, and 47.7% of the patients’ reports showed multiple area involvement. A total of 18.6% of images showed pleural adhesions, 15.1% showed emphysema, and 14.0% showed enlarged mediastinal lymph nodes. 35 patients who were admitted to the B11 Zhongfaxincheng campus of Tongji Hospital had ground-glass opacity.
(2) 厚层砂岩、软弱基座和差异风化形成的凹岩腔,构造形成的剪切裂隙及组合共同构成了滑坡活动的控制性内因,裂隙水及其补给为控制性外因,施工弃土对滑坡活动具有积极推动作用。
Neutrophil ratio, eosinophil ratio, lymphocyte count and amnio-terminal pro-brain natriuretic peptide are significantly different between each group in the two-group comparisons. Additionally, compared with the moderate group, there are 21 more laboratory terms are significantly different (details of the between-group comparisons are shown in Table 2).




Major laboratory markers were tracked in 67 patients on the B11 Zhongfaxincheng campus beginning at admission (Figure 1). During hospitalization, most patients had marked lymphopenia, and patients in the critically ill group developed more severe lymphopenia over time. The level of D-dimer was significantly higher in the critically ill group than in the other groups and rapidly increased from day 11 after admission.Levels of high-sensitivity cardiac troponin I, amino-terminal pro-brain natriuretic peptide (NT-pro BNP), and lactate dehydrogenase were clearly elevated in the critically ill group compared with the other groups throughout the early clinical course but decreased from day 11. The level of albumin was lowest in the critically ill group and decreased with illness deterioration.
刚到太平路小学的时候,我被安排到三年级语数包班。我的心理素质比较好,尤其是讲课的时候,从容沉稳,而且特别不怕领导和同事听课。慢慢地,领导和同事都觉得我是上公开课的材料。
In terms of laboratory tests, the most common laboratory abnormalities observed in the severe and critically ill groups were decreased lymphocytes and albumin, as well as elevated lactate dehydrogenase, C-reactive protein, fibrinogen and D-dimer. In our study, compared with the moderate group, patients in the severe and critically ill groups had numerous laboratory abnormalities, which suggests that COVID-19 may be associated with coagulation activation, liver dysfunction, acute kidney injury,cardiac injury, and immune deficiency. The dynamic change in laboratory findings was tracked in 67 patients with COVID-19. In the critically ill group, the D-dimer,high-sensitivity cardiac troponin I, NT-pro BNP and lactate dehydrogenase levels increased with disease progression, and lymphopenia markedly decreased. Our results were consistent with those of several other studies, which also confirmed that high levels of D-dimer, lactate dehydrogenase, and creatine kinase and the neutrophil-tolymphocyte ratio were independent risk factors for mortality among hospitalized patients with COVID-19[5,11,20].
The results showed that the total model test=17.380,< 0.001, which meant at least one β in the equation did not equal 0, and the final model was preceded to a constant value. The goodness-of-fit test showed=59.137,= 0.968 > 0.05, meaning that the final model fit well. We found that neutrophil-to-lymphocyte ratio (0.042)and high-sensitivity cardiac troponin I (0.043) were statistically significant independent risk factors (details in Table 3). Compared with patients who had normal neutrophil-to-lymphocyte ratios and high-sensitivity cardiac troponin I, the odd ratio(OR) for severe COVID-19 in patients with elevated neutrophil-to- lymphocyte ratios were 4.019 times higher [95% confidence interval (CI): 1.045-15.467] and elevated highsensitivity cardiac troponin I was 10.126 times higher (95%CI: 1.088-94.247).
As of 22March, 2020, 114 (90.5%) of 126 patients were discharged, 8 (6.3%)patients died, and 4 (3.2%) remained hospitalized. Fitness for discharge was based on abatement of fever for at least 3 d, with the disappearance of respiratory symptoms,improvement based on chest radiographic evidence, and two successive indications(interval not less than 24 h) of viral clearance in respiratory samples obtained from the upper respiratory tract. For those who were discharged, the length of hospital stay was 18 d (IQR, 10.0-26.0). For those who died, the time from admission to death was 5.00 d(IQR 1.75-16.50).
DISCUSSION
This retrospective study discovered several clinical features and risk factors for critical illness in patients who were hospitalized with COVID-19 in Tongji Hospital. As of March 8, 2020, 126 patients with COVID-19 were included in this study: 67 from the B11 Zhongfaxincheng campus and 59 from the E1-3 Guanggu campus. Of the 59(46.8%) patients in the moderate group, 24 were male. Of the 49 (38.8%) patients in the severe group, 30 were male. Of the 18 (14.3%) patients in the critically ill group, 13 were male. By 26March, according to National Health Commission statistics, there were 3460 confirmed cases (2880 cases in Wuhan) and 1034 severe cases (995 cases in Wuhan) in China, and to date, 81340 cumulative cases have been confirmed, 3292 have died and 74588 have been discharged[13]. The focus of medical services has now changed to treat patients with severe disease. In the latest Chinese CDC report, 31.1%of confirmed patients were aged over 60, and the crude mortality was highest among patients ≥ 80-years-old (14.8%) and among patients with chronic underlying diseases(5.6%-10.5%)[9]. Similar results were reported in several studies in which increased age and comorbidity were associated with death among patients with COVID-19[5,6,11,14]. Older COVID-19 patients with chronic comorbidities such as hypertension,diabetes, cardiovascular disease, cancer or other coexisting medical conditions were more likely to develop disease involving multiple systems and organs and rapidly progress to poor outcomes[9]. In our study, the median age of the patients was 61.00 years (IQR 48.00-68.00). Patients in the critically ill group were significantly older than those in the moderate group (65.44 years54.76 years,0.019). Patients with cerebrovascular disease, chronic liver disease, and cancer also presented with more severe disease; however, we did not find a significant difference in sex between the 3 groups. When we merged the severe and critically ill group together, the men in the merged group appeared to be more vulnerable to the COVID-19 than those in the moderate group. Recently, several studies have noted that more men than women were diagnosed with severe disease and that men had a higher case fatality rate[15-17]. Channappanavar[18] and Ling Ma[19] indicated that SARS-CoV-2 may affect male gonadal functionACE2 receptors and that estrogen receptor signaling may provide a protective effect during coronavirus infection.

An ordinal logistic regression model was adopted and conducted with JMP15.0 software to explore potential risk factors associated with the severity of COVID-19.Based on data completeness, the clinical significance and the single-factor screening results in Table 1 and Table 2, we first took all the variables proven to be significant in thetests as candidate variables while excluding the time from disease onset to hospital admission, thrombin time, prothrombin time, prothrombin activity and fibrinogen for incomplete data sets, as only one of our research centers had collected these data. Second, we categorized the remaining candidate variables as comorbidity,drug treatment before admission, coagulation system, inflammation markers and liver functional system to the process collinearity diagnosis. Thus, we excluded hemoglobin, chronic liver disease, lactate dehydrogenase and C-reactive protein.Remaining candidate variables included age, sex, cerebrovascular disease, cancer,neutrophil-to- lymphocyte ratio, monocyte ratio, creatinine, aspartate transaminase(AST), drug treatment before admission, albumin, calcium, hematocrit, procalcitonin,NT-pro BNP, platelet count, eosinophil ratio and high- sensitivity cardiac troponin I.Then, a step-by-step regression method (for inclusion = 0.05,for exclusion = 0.05)was applied, and 3 variables were included in the final model: age, neutrophil-tolymphocyte ratio and high-sensitivity cardiac troponin I (Table 3).

Of the 126 patients, 104 (82.5%) had 1 or more coexisting medical conditions.Hypertension [46 (36.5%)], diabetes [22 (17.5%)], cancer [11 (8.7%)], and coronary heart disease [7 (5.6%)] were the most common coexisting conditions. Compared with the critically ill group, the moderate group had fewer patients with cerebrovascular diseases or cancer (< 0.05). Compared with the severe group, the moderate group had fewer patients with chronic liver disease (< 0.05). There were more patients in the critically ill group with 1 or more underlying diseases than in the other groups.Before admission, 33 (33/67, 49.3%) patients reported having taken antibiotics, and third-generation cephalosporins, and quinolone antibiotics were the most common.Twenty-eight (28/67, 41.8%) patients reported taking oseltamivir. Two (2/126, 1.6%)patient reported taking lopinavir/ritonavir. Seventy (70/126, 55.6%) patients reported having taken arbidol. In addition, 83 patients reported having taken traditional Chinese medicine, mainly Lianhua Qingwen capsules. Regarding patients who hadtaken traditional Chinese medicine and arbidol before admission, they were more likely to be in the moderate group (< 0.05) (Table 1).
Compared to the moderate group, the severe and critically ill groups had more patients with abnormal myocardial zymograms and patients who presented with elevated levels of lactate dehydrogenase (59.6% and 88.9%), creatine kinase (2.1% and 22.2%), high-sensitivity cardiac troponin I (0% and 22.2%), and NT-pro BNP (39.6%and 77.8%). Myocardial injury associated with COVID-19 may be due to hypoxemia and systemic pro-inflammatory cytokine responses. In a fatal case of COVID-19 in China, interstitial mononuclear inflammatory infiltrates in heart tissue were confirmed, but parenchymal damage and viral detection were not evident[22].
Regarding the coagulation indicators, D-dimer was above the normal range in 79.6%of the patients in the severe group and in 100% of the patients in the critically ill group;the thrombin time was longer than normal in 11.1% of the patients in the severe group and in 33.3% of the patients in the critically ill group; and the prothrombin time was longer than normal in 16.7% of the patients in the severe group and 41.7% of the patients in the critically ill group, indicating the profound influence of COVID-19 on the coagulation system. Possible reasons for coagulation activity may be direct injury to endothelial cells by SARS-CoV- 2[23,24], which is also related to atherosclerotic plaque rupture induced by inflammation and the release of procoagulant factors released[11]. Basic studies also confirmed that an inflammatory cytokine storm induced by the virus could lead to lymphocyte apoptosis and that lymphocytes express ACE2 receptors, which make them direct targets of SARS-CoV- 2[25]. The elevation in proinflammatory factors may increase fibrin deposition in the pulmonary microvasculature, contributing to acute respiratory distress syndrome and disseminated intravascular coagulation and significantly increasing blood lactic acid and Ddimer levels[26,27]. Acute kidney injury is directly related to viral attack and cytokine storms, causing metabolic acidosis with elevated creatine and decreased serum calcium levels[1,2,11,17].
However, there are still some limitations to our study. First, the majority of our patients were transferred from local hospitals during the late phases of their illnesses,which caused the collection of medical history to be limited. Second, in this retrospective study, some of the laboratory tests were not routinely performed for all patients or were periodically conducted during the progression of the disease. Third,our study was conducted only on two campuses in one nation (China); not all the analyses were available simultaneously at both centers, and some comparisons were performed only on one campus.
CONCLUSION
In conclusion, people of all ages, both male and female, are susceptible to COVID-19.Early drug treatment is an important measure in the treatment of patients with COVID-19, and the following indicators can help clinicians identify patients with severe COVID-19 at an early stage: age, an elevated neutrophil-to-lymphocyte ratio and high sensitivity cardiac troponin I.


A total of 126 patients were enrolled. There were 59 in the moderate group, 49 in the severe group, and 18 in the critically ill group. Over 50% patients have increased levels of lactate dehydrogenase, aspartate transaminase (AST), C-reactive protein, fibrinogen,D-dimer, tumor necrosis factor-α, ferritin, as well as decreased levels of hematocrit and calcium. Compared with the moderate group, the severe and critically ill group has significant higher rates of abnormality in levels of neutrophil ratio, eosinophil ratio,lymphocyte ratio, platelets count, neutrophil to lymphocyte ratio, AST, albumin,procalcitonin, calcium, D-dimer, interleukin-6, high-sensitivity cardiac troponin,amino-terminal pro-brain natriuretic peptide (NT-pro BNP), and ferritin. Multivariate logistic regression analysis showed that no drug treatment before admission, a higher neutrophil-to-lymphocyte ratio, a higher AST level, a higher NT-pro BNP level, a higher creatinine level, and serum calcium below the normal range were high-risk factors.
People of all ages, both male and female, are susceptible to COVID-19. Early drug treatment is an important measure in the treatment of patients with COVID-19, and the following indicators can help clinicians identify patients with severe COVID-19 at an early stage: an elevated neutrophil-to-lymphocyte ratio; elevated AST, NT-pro BNP, and creatinine levels; and serum calcium below the normal range.
饮食及药物:中药中,香附、郁金、佛手、香橼、玫瑰花等可以疏肝理气,枸杞、女贞子、墨旱莲、桑葚、黑芝麻等有养阴精、补肝肾之功。中成药中的六味地黄丸有滋补肝肾之功,可用于肝肾阴虚出现的腰膝酸软、头晕目眩、耳聋耳鸣等;加味逍遥丸可治疗肝郁血虚引起的两胁胀痛、头晕目眩、月经不调等。一些药食同源之品,如菊花、桑叶、百合泡茶可以清肝明目,玫瑰花、月季花可以调经解郁,莲子、芡实可补肾固精等。
A large sample size with long-term survival data is needed in future studies.
杂志排行

World Journal of Clinical Cases的其它文章
- Lung injury after cardiopulmonary bypass: Alternative treatment prospects
- Acute myocardial injury in patients with COVID-19: Possible mechanisms and clinical implications
- Anemia in cirrhosis: An underestimated entity
- High tumor mutation burden indicates a poor prognosis in patients with intrahepatic cholangiocarcinoma
- Does delaying ureteral stent placement lead to higher rates of preoperative acute pyelonephritis during pregnancy?
- Management of retroperitoneal sarcoma involving the iliac artery: Single-center surgical experience