Thalidomide for refractory gastrointestinal bleeding from vascular malformations in patients with significant comorbidities
2020-09-10AlexisMaeBayudanChienHuanChen
Alexis Mae Bayudan, Chien-Huan Chen
Alexis Mae Bayudan, Department of Medicine, Washington University School of Medicine, St.Louis, MO 63108, United States
Chien-Huan Chen, Division of Gastroenterology, Department of Internal Medicine, Washington University School of Medicine, St.Louis, MO 63110, United States
Abstract
Key words:Vascular malformation;Thalidomide;Refractory gastrointestinal bleeding;Gastric antral vascular ectasia;Angiodysplasia
INTRODUCTION
Gastrointestinal vascular malformations (GIVM) consist of several types such as gastrointestinal angiodysplasias (GIAD) and gastric antral vascular ectasias (GAVE).The pathogenesis of vascular malformations remains unclear, but is thought to be due to an imbalance of pro-angiogenic factors, such as vascular endothelial growth factor(VEGF), and anti-angiogenic properties leading to neovascularization[1].In vitrostudies have also demonstrated hypoxic conditions leading to increased expression of hypoxia-inducible-factor-1-α (HIF-1α) and HIF-2α, which upregulate VEGF and participate in the formation of GIVM[2].Patients with GIVM can present with overt gastrointestinal bleeding (GIB) or iron deficiency anemia (IDA) due to chronic occult blood loss, and can be associated with significant morbidity and mortality.
GIAD are abnormal, dilated, tortuous vessels within the mucosal and submucosal layers and are the most common GIVM seen throughout the gastrointestinal tract.GIAD can account for up to 40% of occult GIB episodes[3].Several chronic conditions have been associated with GIAD such as aortic stenosis, which can cause an acquired von Willbrand disease leading to increased GIB, also known as Heyde’s Syndrome.GIAD has also been shown to increase risk of GIB in patients with left ventricular assist devices (LVAD) as well as chronic renal failure.
GAVE is generally found in patients with chronic illnesses, such as liver disease,connective tissue diseases, and chronic renal failure.Bleeding from GAVE accounts for 4% of upper GIB and is commonly found in women.Endoscopically, GAVE appears as either punctate lesions throughout the stomach or as red lesions radiating from the pylorus in stripes, known as “watermelon stomach”.Generally, it is found in the antrum with rare presentations in the proximal stomach.Histologically, GAVE is characterized by vascular ectasia of mucosal capillaries, focal thrombosis, spindle cell proliferation, and fibrinolysis.
Endoscopic therapy primarily with argon plasma coagulation (APC) is the mainstay of treatment for GIVM.However, GIVM refractory to endoscopic treatment is common and medications such as octreotide[7], tranexamic acid[8,9], hormonal therapy (estrogenprogesterone)[10], and thalidomide[8,11-23]have all been studied in the management of recurrent GIB refractory to endoscopic therapy.
采用“明沟加集水坑”进行基坑内排水主要方法,依据实际情况确定排水沟间距,坡度控制在1.5%,排水沟宽、深分别为300mm与200~600mm;要求排水沟距离坡脚1.1m以上;将“截水沟”排水系统设置在坑顶处,及时对地面流水、雨水进行疏通与排除,雨季要准备抽水设施。
Thalidomide, known to have antiangiogenic properties by suppressing VEGF, has been shown in several studies (Table 1) to be a promising treatment option for refractory GIB from GIVM[11-22].However, only one randomized control trial has beenreported by Geet al[8]in a Chinese population in 2011.In addition, this study has an extensive exclusion criteria, such as comorbidities of cardiac, pulmonary, liver, renal,hematologic, and rheumatologic disorders;history of thromboembolic disease;or patient on antiplatelet agent or anticoagulation.Given that patients with recurrent GIB from GIVM are frequently elderly with several comorbidities, it is unclear whether the results of this study can be extrapolated to other patient populations.Whereas there are several reported case series on the effects of thalidomide on patient with cirrhosis or LVAD[13,20-22], many other studies excluded patients with significant comorbidities(Table 1).We therefore decided to conduct a retrospective study of thalidomide in treating refractory GIB from GIVM in a Western population with significant comorbidities at a tertiary medical center.

NSAID:Non-steroidal anti-inflammatory;ASA:Aspirin;HE:Hepatic encephalopathy;LVAD:Left ventricular assist device;GIB:Gastrointestinal bleeding.
MATERIALS AND METHODS
Study population
This is a retrospective study of patients diagnosed with GIVM at the Division of Gastroenterology, Washington University Medical Center/Barnes-Jewish Hospital,from January 2012 to November 2018 who were treated with thalidomide.The institutional review board at Washington University in St.Louis, Missouri approved the study.
Inclusion criteria
Aged ≥ 18 years old;male and post-menopausal females;>3 episodes of GIB with >1 episode of refractory bleeding;documented vascular malformation (either GIAD or GAVE) on either upper endoscopy (esophagogastroduodenoscopy) or colonoscopy and if bleeding was not initially found, subsequent balloon enteroscopy or capsule endoscopy;and treated with thalidomide for at least 3 months.Refractory bleeding was defined as recurrent bleeding requiring >2 transfusions after failing 2 treatments with endoscopic therapy using APC or medical therapies, such as octreotide, estrogen,or aminocaproic acid.Exclusion criteria:Patients with other causes of GIB, patients with allergy to thalidomide, women who were pregnant or lactating, and premenopausal women.
Thalidomide treatment
All of the patients included in this study were prescribed thalidomide (Thalomid®) by a single certified provider (Chen CH) according to the Thalomid Risk Evaluation and Mitigation Strategy (REMS) program of Celgene (NJ, United States).Patients were started on thalidomide for more than 3 episodes of GIB requiring blood transfusion with recurrent GIB after failing at least two treatments with endoscopic therapy or medical therapy.Patients were started on thalidomide 50 mg twice daily or 100 mg once daily.This initial dose was increased or decreased depending on patient’s response and ability to tolerate the medication.During the treatment period, patients were monitored by phone every 4 wk and in the outpatient clinic every 3 to 6 mo.Complete blood count and comprehensive metabolic panel were monitored every 3 to 6 mo.
In the event of an adverse side effect, thalidomide was temporarily or permanently discontinued depending on the severity of the side effect and the patient’s tolerability.During treatment with thalidomide, adjunct therapy such as blood transfusions or repeat endoscopic treatment were performed as necessary at the discretion of treating physicians.Transfusion was given to patients when hemoglobin level fell below 7.0 g/dL.Patients were continued on antiplatelet or anticoagulation or iron supplementation if they were taking it prior to initiation of thalidomide.
Data collection
Data collected from electronic medical records included patient’s demographics,medical history, comorbidities, medications, number of hospitalizations, endoscopic treatment, and number of blood transfusions.
Assessment
The primary endpoint was to assess the recurrence of GIB 6 mo after the initiation of thalidomide.The secondary endpoints were the number of hospitalizations, blood transfusion requirements, and endoscopic treatments.A bleeding recurrence was defined as a GIB episode with hemoglobin level less than 7.0 g/dL resulting in a blood transfusion.All bleeding episodes of the patients studied were due to GIVM.Patients were encouraged to keep in close contact with patient care coordinators to update the team on their progress, possible side effects from thalidomide, and any bleeding episodes requiring blood transfusions or hospitalizations that occurred in between office visits.
RESULTS
A total of 15 patients were included in this study.Table 2 details the demographic and clinical characteristics of patients included in this study.Mean age was 69 (range:58-83) years old.There were 6 women (40%) and 9 men (60%).Eleven patients were Caucasian (73.3%) and four patients were African American (26.7%).Body mass index median was 28.6 (range:21-48).All patients in this study had multiple comorbidities.Six patients had cirrhosis (n=5) or non-cirrhotic portal hypertension;Child-Pugh class A (n=2), class B (n=3).Three had end stage renal disease (ESRD) on hemodialysis, 3 had chronic kidney disease, stage 3 (n=2), stage 5 (n=1).Three had a LVAD, 10 had hypertension, 5 had diabetes, 1 had myelodysplastic syndrome (MDS) and non-Hodgkin’s lymphoma, 1 had polyclonal gammopathy, 2 had aortic stenosis, and 1 had hereditary hemorrhagic telangiectasias.
The cause of GIB was GIAD in 10 patients (66.6%) and GAVE in 5 patients (33.3%).Prior to treatment with thalidomide, 6 patients were previously treated with octreotide, 1 treated with estrogen, and 1 treated with aminocaproic acid.All patients received at least two treatments of APC before starting thalidomide, except for one whose source of bleeding was not reachable via endoscopy.All patients prior to the initiation of thalidomide had anemia with average hemoglobin level of 7.9 g/dL.Five patients were on iron supplement when referred to our care and 3 patients with iron deficiency were not on iron supplement.Eight patients continued with iron supplementation after initiation of thalidomide treatment.Five patients remained on antiplatelet or anticoagulation such as aspirin, warfarin, clopidogrel, or cilostazol.Twopatients discontinued thalidomide:One due to cost and another due to drug interaction with methadone, after being treated with thalidomide for 17 mo and 3 mo respectively.Two other patients were lost to follow up.
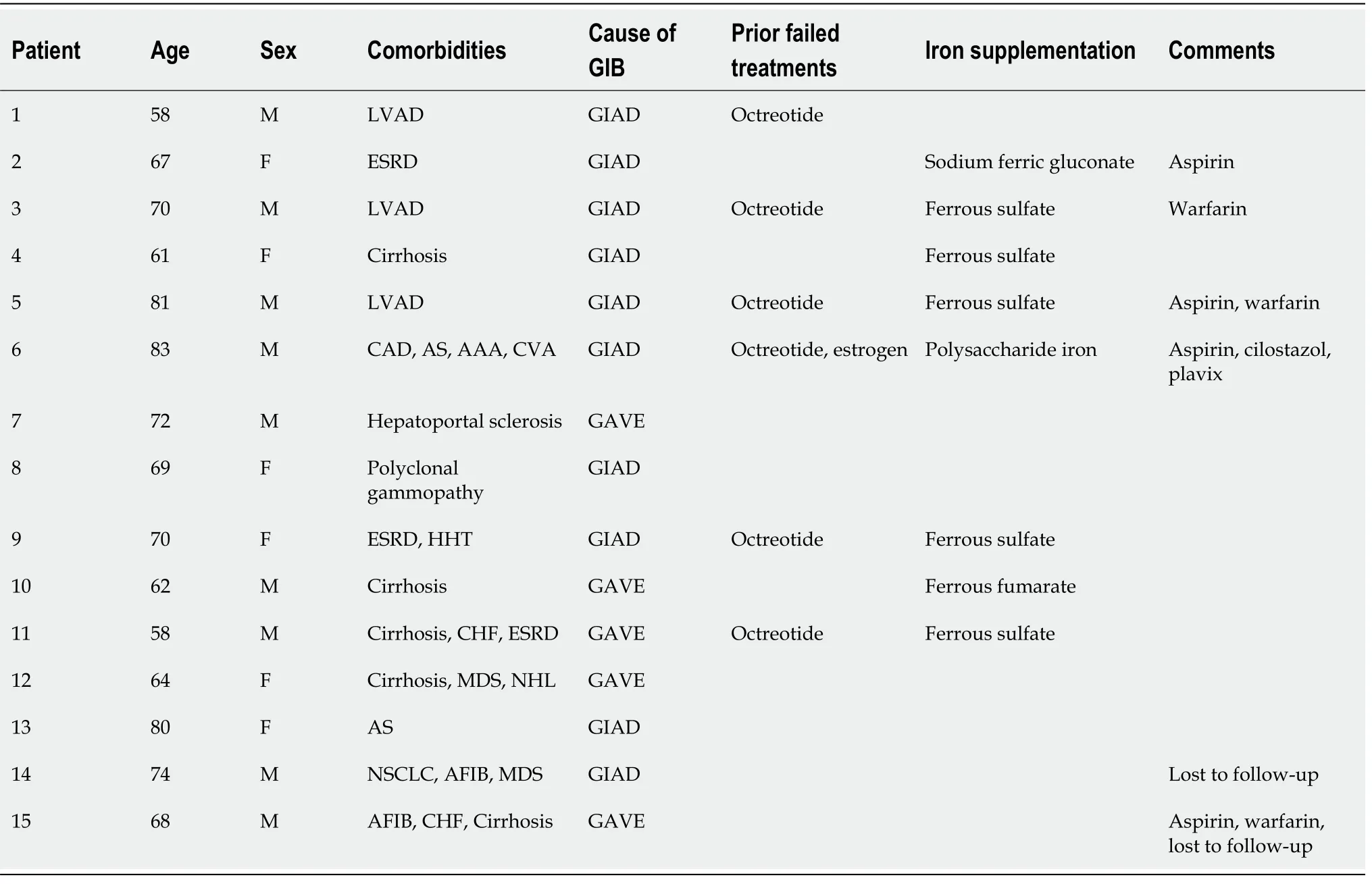
Table 2 Patient characteristics
During the one year prior to starting thalidomide, of the 13 patients who remained in the study, the mean number of hospital admissions for GIB was 5.46 (range, 1-20 admissions), the mean number of packed red blood cell (PRBC) transfusions was 31 units (range, 8-99 units) and the mean number of endoscopic treatments was 4.54(range, 0-12 endoscopic treatments).
Thalidomide was started at either 50 mg twice daily or 100 mg once daily.Ultimately the dose of thalidomide ranged from 50 mg to 200 mg daily, titrating to patients’ response and tolerability.The average duration of treatment on thalidomide was 28 mo (range, 3-45 mo).
Of the 13 patients followed (range 3-45 mo), 9 patients had GIAD and 4 patients had GAVE.GIAD were located in the gastric fundus (n=1), duodenum (n=3), jejunum (n=5), ileum (n=1), and hepatic flexure of colon (n=1).After initiation of thalidomide treatment for 6 mo, 5 patients (38.5%) met our primary endpoint with no recurrent GIB episodes during follow-up (Figure 1).Of these 5 patients, 2 had an LVAD and GIAD, 2 had cirrhosis and GAVE, and 1 had cirrhosis and GIAD.Another 6 patients (46.2%)had both marked reduction in transfusion requirements and hospitalizations for GIB(Figure 1 and Table 3).Two patients had increased transfusion after treatment with thalidomide for 3 and 30 mo.The requirement of endoscopic treatments decreased in 11 patients (84.6%) after the initiation of treatment.Of the 11 patients who responded favorably to treatment, the effect of thalidomide could be observed after 3 mo of treatment.Significant reduction of GIVM could be seen during follow-up endoscopies,as demonstrated in a patient with GAVE who underwent esophagogastroduodenoscopy 3 and 8 mo after treatment with thalidomide (Figure 2).
All 4 patients who remained on anticoagulation or antiplatelet therapy, including 2 with an LVAD, had a significant decrease in GIB as demonstrated by a decreased transfusion requirements and hospitalizations.Additionally, all 4 patients withcirrhosis had a marked decrease in hospitalizations, blood transfusions, and endoscopic treatments.The 3 patients with ESRD on dialysis and 3 patients with chronic kidney disease all showed improvement in transfusion requirements after treatment.
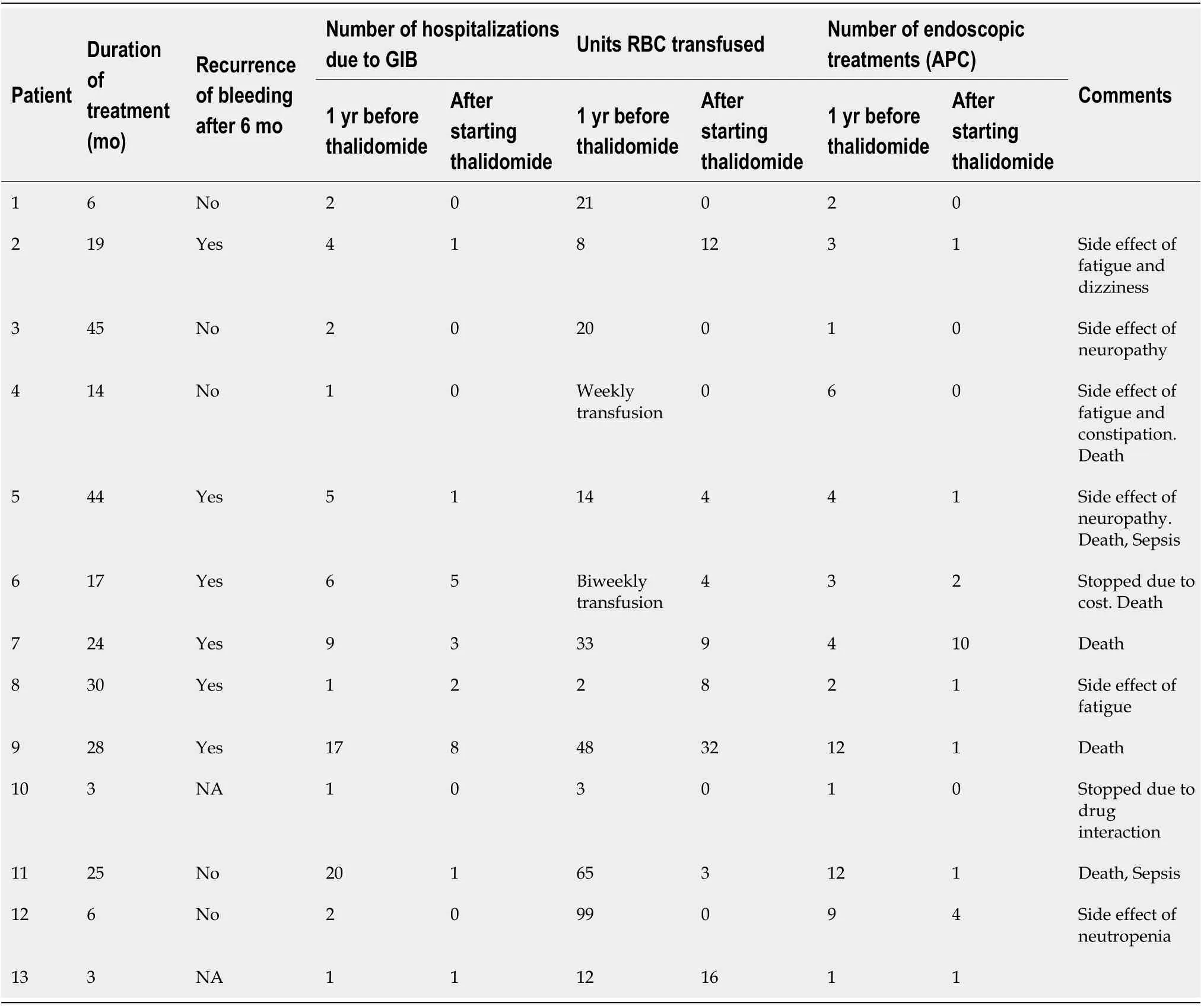
Table 3 The effect of thalidomide treatment on refractory gastrointestinal bleeding due to vascular malformation
Reported adverse reactions were documented in 6 of the 13 patients (46%),including fatigue (n=3), neuropathy (n=2), constipation (n=1), and dizziness (n=1).Worsening neutropenia was observed in a patient with concurrent MDS, with stabilization of white blood cell counts after a dose reduction of thalidomide from 100 mg to 50 mg daily.GIB did not recur after this dose reduction.Six patients died during the follow-up period of this study.Five patients died while on thalidomide due to causes unrelated to recurrent GIB and one patient died from unknown causes after discontinuing thalidomide due to cost.All patients who died while taking thalidomide had been treated for over 1 year.Of the 5 patients who died while taking thalidomide,2 died from complications due to sepsis, 1 sustained a traumatic fall and passed away in hospice, and 2 died from unknown causes.
DISCUSSION
This retrospective study aimed to examine the effect of thalidomide on refractory GIB due to GIVM.Our results demonstrated that thalidomide appears to be an effective medical therapy for this very challenging patient population.Five out of 13 patients(38.5%) followed in our study had no recurrent GIB after treatment with thalidomide,while overall 11 out of 13 patients (86.4%) had decrease in recurrence of GIB,hospitalizations, blood transfusions and endoscopic therapies.
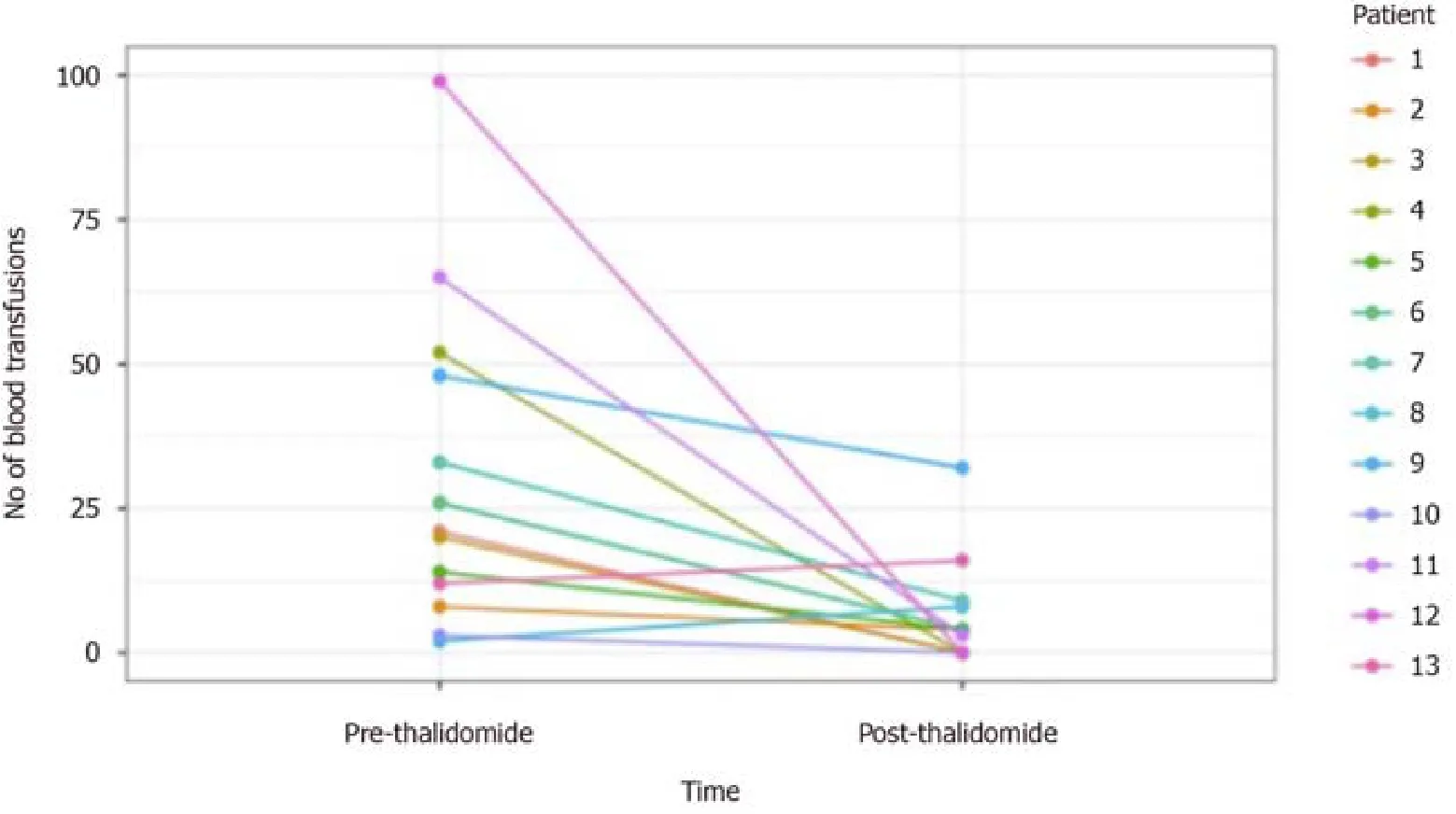
Figure 1 Units of packed red blood cell transfused before and after initiation of thalidomide.
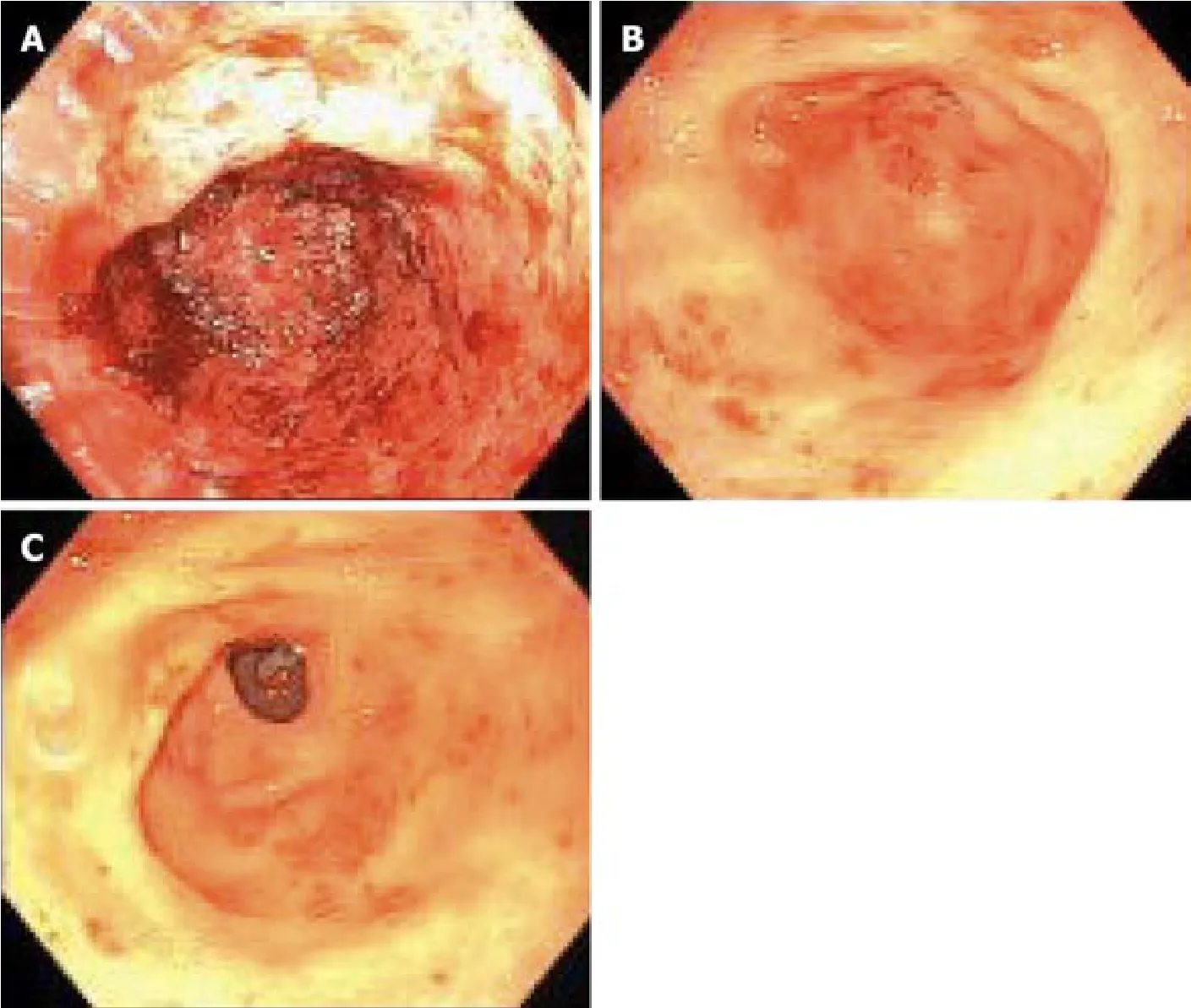
Figure 2 Endoscopic pictures of gastric antral vascular ectasia before and after treatment with thalidomide.
Previous studies and case reports have reported similar results with thalidomide in treating recurrent GIB from GIVM[8,10-22].Whereas the only randomized controlled trial so far by Geet al[10]from China found a response rate of 71.4%, patients with cardiac,pulmonary, hepatic, renal, and other comorbidities were excluded from the study.In a follow-up retrospective study by the same group with 80 patients, the response rate to thalidomide in patients with or without comorbidities was 76.7% and 78%respectively, although this study again excluded patients with severe comorbidities such as cirrhosis and severe cardiac and renal conditions[14].Therefore, it is unclear whether these results could be applied to other patient populations with significant comorbidities.Three previous case series of patients with an LVAD[13]and one case study of patients with liver cirrhosis[17]found thalidomide effective in treating refractory GIB patients with these comorbidities.The response rate in our study was 84.6%, comparable to other previous studies.The patients in our study represent the most challenging recurrent GIB patients we encounter in a tertiary referral medical center, as evidenced by their multiple comorbidities, and the average number of admissions (5.46) and transfusions (31 units of PRBC) one year before the initiation of thalidomide.Our study demonstrated that thalidomide remains an effective treatment for refractory GIB from GIVM in a Western population, including patients with severe comorbidities such as LVAD, cirrhosis, and ESRD on dialysis.
Anticoagulation or antiplatelet agents are frequently discontinued in the setting of GIB.However, this increases the risk of thromboembolism especially in patients with significant cardiovascular comorbidities and patients with LVAD.Four of our patients continued their anticoagulation or antiplatelet agents such as warfarin, aspirin,clopidogrel, or cilostazol, and still responded favorably to thalidomide.Our results suggest that it may not be necessary to discontinue anticoagulation or antiplatelet agents in this group of patients with severe multiple comorbidities while on thalidomide.One patient with severe GAVE and platelet count <30000/mL due to MDS received 99 units of PRBC in the one year before thalidomide treatment, and required no transfusion after treatment.More data is needed to determine whether correcting thrombocytopenia is necessary when treating GIVM with thalidomide.
Thalidomide is thought to inhibit angiogenesis by suppressing VEGF.In our study,the effects of thalidomide became apparent after about 3 mo of treatment, consistent with the observation of previous studies[15,17,19].The interval between the initiation of thalidomide and the decrease of GIB likely reflects the time it takes to change the balance between anti- and pro- angiogenesis factors in the existing GIVM and suppressing new GIVM formation.The effectiveness of thalidomide in treating GIB from GIVM as shown in this and other studies suggests that we could potentially explore other angiogenesis inhibitors to treat GIVM.
The dose of thalidomide in previous studies ranged from 50 mg to 400 mg per day.Dosing and efficacy could possibly be related to a patient’s body mass index (BMI), as was suggested by Senget al[20]where BMI median was 18.The initial dose of thalidomide in their study was 50 mg daily for all patients, whereas other studies typically used at least 100 mg daily[16,20].In our study, the dose of thalidomide was started at 100 mg daily, with the final dosage ranged from 50 to 200 mg daily.The median BMI of our patients was 28.Seven of our patients improved on thalidomide 100 mg daily, whereas two patients did not see improvement of bleeding until the dose of thalidomide was increased to 150 and 200 mg daily, with a BMI of 28 and 48 respectively.Two non-responders in our study were treated with 200 mg daily with a BMI of 30, and 100 mg daily with BMI of 24.We do not see a clear association of dose,BMI, and effectiveness based on our data.Further study is needed to elucidate the relationship between the response to thalidomide and BMI.
The common side effects of thalidomide include drowsiness, fatigue, dizziness,neuropathy, skin rash, and constipation.The most common side effect reported in our study was fatigue (n=3).Fatigue and dizziness were reported in one patient who mistakenly took double dose of thalidomide, and resolved once she went back to the prescribed dose.Neutropenia (n=1) occurred in a patient with MDS, and resolved upon reducing the dose of thalidomide to 50 mg daily and without recurrence of GIB.Neuropathy was described in 2 patients, one of which had a history of parkinsonism and another with a history of diabetes.No thromboembolism was observed in our study, although the reported risk of thromboembolism associated with thalidomide is mainly seen in patients with multiple myeloma on chemotherapy.Five patients died while on thalidomide and one patient died after discontinuation of thalidomide due to cost.The cause of death does not appear to be associated with thalidomide (sepsis 2,fall 1) in 3 patients.The cause of death in 2 patients was unknown and therefore unclear if it is related to thalidomide.
The major limitations of this study are the limitations inherent with a retrospective study, such that we were not able to control for variables like the degree of IDA or whether patients were taking iron supplement.Another limitation is our small sample size (n=15).Most of our patients with refractory GIB were elderly with limited income.Many patients could not receive treatment with thalidomide due to cost or lack of insurance coverage.Even more patients declined treatment with thalidomide due to concern of potential side effects in the context of their multiple comorbidities after reading the patient medical information from REMS.Nevertheless, our sample size is the second largest from the Western World in the literature.In addition, our primary and secondary outcomes were objective measures and less susceptible to reporting bias.With more data published on thalidomide in recurrent GIB, we may see improvement in its coverage or patients’ acceptance.
In conclusion,the treatment of patients with refractory GIB due to GIVM remains a daunting task with limited options.Our study suggests that thalidomide appears to be an effective treatment for refractory GIB due to GIAD or GAVE in a Western population with significant comorbidities such as LVAD, portal hypertension, and ESRD.
ARTICLE HIGHLIGHTS
Research background
Gastrointestinal vascular malformations (GIVM) consist of several types such as gastrointestinal angiodysplasias (GIAD) and gastric antral vascular ectasias (GAVE).GIAD are abnormal, dilated, tortuous vessels within the mucosal and submucosal layers and are the most common GIVM seen throughout the gastrointestinal tract.GAVE is generally found in patients with chronic illnesses, such as liver disease,connective tissue diseases, and chronic renal failure.Refractory gastrointestinal bleeding (GIB) secondary to GIVM remains challenging to treat when endoscopic therapy fails.Endoscopic therapy with argon plasma coagulation (APC) is the mainstay of treatment for GIVM.However, GIVM refractory to endoscopic treatment is common and medications such as octreotide, tranexamic acid, hormonal therapy such as estrogen-progesterone, and thalidomide have all been studied in the management of recurrent GIB refractory to endoscopic therapy.Thalidomide, known to have antiangiogenic properties by suppressing VEGF, has been suggested recently as a treatment option for refractory GIB.
Research motivation
Only one randomized control trial demonstrating the efficacy of thalidomide for treating refractory GIB due to GIVM has been published in 2011 in a Chinese population.However, the study had extensive exclusion criteria and it is unclear whether the results of the study can be extrapolated to other patient populations.We therefore decided to conduct a retrospective study of thalidomide in treating refractory GIB from GIVM in a Western population with significant comorbidities at a tertiary medical center.
Research objectives
To evaluate thalidomide as a treatment option for patients who suffer from refractory GIB due to GIVM.
Research methods
Single center, IRB approved, retrospective review of electronic medical records from January 2012 to November 2018.Patients age >18 years old, who had >3 episodes of GIB refractory to medical or endoscopic therapy and documented to be due to GIVM,and who had been treated with thalidomide for at least 3 months were included.Refractory bleeding was defined as recurrent bleeding requiring >2 transfusions after failing 2 treatments with endoscopic therapy using APC or medical therapies, such as octreotide, estrogen, or aminocaproic acid.The primary endpoint was recurrence of GIB 6 mo after initiation of thalidomide.The secondary endpoints were the number of hospitalizations, blood transfusion requirements, and endoscopic treatments.
Research results
Fifteen patients were included in the study, all with significant cardiac, hepatic, or renal comorbidities.The cause of GIB was GIAD in 10 patients and GAVE in 5 patients.Two patients were lost to follow up.Of the 13 patients followed, 38.5% (n=5)had no recurrent GIB or transfusion requirement after treatment with thalidomide.Furthermore, 84.6% (n=11) of patients had a reduction in transfusion requirements and hospitalizations for GIB.Thalidomide was discontinued in 2 patients due to cost (n=1) and medication interaction (n=1).Reported adverse reactions included fatigue (n=3), neuropathy (n=2), dizziness (n=1), and constipation (n=1).Six patients died during follow up due to unknown cause (n=4) and sepsis (n=2).
Research conclusions
Our results demonstrated that thalidomide appears to be an effective medical therapy for refractory GIB due to GIVM.The response rate in this study was 84.6%,comparable to other previous studies.The patients in our study represent the most challenging recurrent GIB patients in a tertiary referral medical center, as evidenced by their multiple comorbidities, and the average number of admissions (5.5) and transfusions (31 units of PRBC) one year before the initiation of thalidomide.Our study demonstrated that thalidomide remains an effective treatment for refractory GIB from GIVM in a Western population, including patients with severe comorbidities such as left ventricular assist device, cirrhosis, and end-stage renal disease on dialysis.
Research perspectives
Based on the results of this study, future research should include prospective randomized control trial with a larger patient population so that we can examine the effect of thalidomide on each comorbidity with sufficient power.
猜你喜欢
杂志排行
World Journal of Clinical Cases的其它文章
- Impacts and challenges of United States medical students during the COVID-19 pandemic
- Recent advances in the management of gastrointestinal stromal tumor
- Medical research during the COVID-19 pandemic
- Progress of intravoxel incoherent motion diffusion-weighted imaging in liver diseases
- Typical and atypical COVID-19 computed tomography findings
- Review of possible psychological impacts of COVID-19 on frontline medical staff and reduction strategies