Electronic moxibustion apparatus and traditional moxibustion in treating knee osteoarthritis: a randomized controlled trial
2020-08-29XueKun薛堃XingQiujuan邢秋娟WangYaqiong王雅琼WuJi吴佶ZhaoHaiyin赵海音LuWang鲁望
Xue Kun (薛堃), Xing Qiu-juan (邢秋娟), Wang Ya-qiong (王雅琼), Wu Ji (吴佶), Zhao Hai-yin (赵海音), Lu Wang (鲁望)
1 Tianshan Hospital of Traditional Chinese Medicine, Changning District of Shanghai, Shanghai 200051, China
2 Yangpu Hospital, Tongji University, Shanghai 200090, China
3 Longhua Hospital Shanghai University of Traditional Chinese Medicine, Shanghai 200032, China
Abstract
Keywords: Moxibustion Therapy; Moxa Stick Moxibustion; Electronic Moxibustion Apparatus; Osteoarthritis, Knee; Pain Measurement; Visual Analog Scale
Knee osteoarthritis (KOA) is a chronic progressive knee joint disease mostly affecting the mid-aged and elderly population. Degenerative knee cartilage and secondary hyperosteogeny are the major changes in KOA and it clinically presents as joint pain, stiffness and limited range of motion. As a result of the increasing aging population in China, the high incidence rate and low recovery rate of KOA have seriously affected the motor function and quality of life of the mid-aged and elderly people. The latest epidemiological study showed that the incidence rate of KOA had reached 9.56% in China[1], which gradually rose with the increase of age. Currently, the prevalence rate has reached as high as 78.5% among people over 60 years old[1]. In traditional Chinese medicine (TCM), moxibustion therapy is a safe effective and convenient intervention. Moxibustion has been proved effective for KOA by numerous clinical trials worldwide[2-4]. A study reported that moxibustion therapy has showed great advantages in treating KOA[5], and has achieved satisfactory efficacy when used alone in treatment of KOA[6-8].
With the development of modern scientific technology and gradual deepening of innovative concept, multidisciplinary research of green, easy-to- operate and effective novel moxibustion diagnosis and treatment techniques has become a new development direction. Some clinicians have already analyzed and summarized the shortcomings of traditional moxibustion therapy. They have also attempted to establish novel moxibustion apparatuses and compared them with traditional moxibustion regarding the efficacy.
By conducting a randomized controlled trial, this study was to observe the efficacy and safety of DZWJY-1 type electronic moxibustion apparatus and traditional moxibustion, and to provide certain evidences for the clinical application of electronic moxibustion apparatus.
1 Materials and Methods
1.1 Diagnostic criteria
1.1.1 Diagnostic criteria of Western medicine It was based on the diagnostic criteria of KOA stipulated by the American College of Rheumatology (ACR) in 1995[9]. ① Knee pain occurred for most of the time during the previous 1 month; ② formation of osteophyte; ③ age >40 years old; ④ morning stiffness ≤30 min; ⑤ bony crepitus during joint motion. KOA can be diagnosed when items ①+② or ①+③+④+⑤ were met.
1.1.2 Syndrome differentiation standard in TCM
It referred the syndrome differentiation standard for Gu Bi (bone Bi-impediment) set up in theCriteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine[10].
1.2 Inclusion criteria
Conformed to the above diagnostic criteria for KOA of both Western medicine and TCM; aged 40-75 years old; agreed and signed the informed consent form; did not use any Chinese or Western medications or other treatments related to KOA during the recent 1 month.
1.3 Exclusion criteria
Patients with acute knee joint injuries, tuberculosis or tumor in knee joint, rheumatic diseases or rheumatoid arthritis affecting the knee joint; imaging tests discovered significant narrowed joint space or formation of bone bridge or even bony ankyloses; notable knee joint deformities, such as varus and valgus; the affected limb had a history of neurovascular injuries; coupled with severe diseases involving the cardiocerebral vascular system, liver, kidney and hematopoietic system; mental disorders; women during pregnancy or lactation period.
1.4 Rejection and dropout criteria
Dropout: Patients who failed to complete 12 sessions of treatments regardless of reason.
Rejection: Those who took drugs containing calcium during the intervention; did not successfully follow the treatment or daily living requirements of the trial, making it impossible to evaluate the therapeutic efficacy; received other treatments during the intervention.
1.5 Adverse events and managements
In this trial, adverse event was defined as adverse reactions caused directly or indirectly by the electronic moxibustion apparatus or traditional moxibustion, such as dizziness due to moxibustion treatment or burns; skin allergies or other discomforts. For fatal adverse events, immediate rescue interventions needed to be applied. All the adverse events that happened in the trial should be recorded in details by case report form (CRF), including the beginning and ending times, severity level, intervention and outcome, etc.
1.6 Statistical methods
The SPSS version 21.0 statistical software was adopted. All the data were examined using the two-sided hypothesis test with the standard set atα=0.05, andP<0.05 indicated statistical significance. Measurement data in normal distribution were expressed as mean ± standard deviation (±s), andt-test or analysis of variance was used. Median was used to present the mean level of the measurement data not meeting normal distribution and rank-sum test was employed. In respect of numeration data, the non-ranked data were examined using Chi-square test or non-parametric test, while the ranked data were examined using rank-sum test orRiditanalysis. Blinding method was applied during data analyses.
1.7 General data
The subjects recruited in this trial were all the outpatients from the Rehabilitation Department of Tianshan Branch and the TCM Treatment Department of Pudong Branch of Longhua Hospital Shanghai University of Traditional Chinese Medicine between May 2017 and April 2019. Seventy-six patients conforming to the inclusion criteria were randomized into an electronic moxibustion apparatus group and a traditional moxibustion group, with 38 cases in each group. The SPSS version 21.0 software was used to generate sufficient random numbers. In this trial, those with an odd ending number were classified into the electronic moxibustion apparatus group and those with an even number were recruited into the traditional moxibustion group. The numbers were put into coded non- transparent envelopes. The recruited subjects were all given an envelope according to their recruitment sequence and rigorously entered into the corresponding group.
Four patients in the traditional moxibustion group failed to complete the required treatments due to their own reasons and thus were considered as dropout cases. Finally, there were 72 valid cases, including 38 cases in the electronic moxibustion apparatus group and 34 cases in the traditional moxibustion group. Statistical analyses of the general data such as age, height, body weight, gender and disease duration showed no significant differences between the two groups (allP>0.05), indicating the comparability (Table 1). There was no significant difference comparing the pre-treatment joint function grading between the two groups (P>0.05), suggesting the comparability (Table 2). There was no significant difference comparing the pre-treatment radiographic staging of osteoarthritis between the two groups (P>0.05), also indicating the comparability (Table 3).

Table 1. Comparison of the general data between the two groups

Table 2. Comparison of the pre-treatment joint function grading (case)

Table 3. Comparison of the pre-treatment radiographic staging of osteoarthritis (case)
2 Treatment Methods
Points: Neixiyan (EX-LE 4), Dubi (ST 35), Xuehai (SP 10) and Liangqiu (ST 34) on the affected side.
Point selection was same in the two groups and the points were all located following theNomenclature and Location of Acupuncture Points(GB/T 12346- 2006)[11].
2.1 Electronic moxibustion apparatus group
This group was treated using DZWJY-1 type electronic moxibustion apparatus (invented by Shanghai University of Traditional Chinese Medicine, Patent Number: 201410320973.3). The apparatus had been tested by Shanghai Medical Device Testing Center and its action mechanism and technical parameters were referenced[12]and put on file by Shanghai Food and Drug Administration [File Number: Hu Xie Lin (20160082)].
Methods:Patient took a supine position with the affected lower limb putting straight naturally. The electronic moxibustion apparatus was turned on with the temperature set at the range of 46-50 ℃ and within the patient’s endurance and treatment duration was 30 min. After standard sterilization, one round moxa essential oil patch of 1 cm in diameter was placed at each of the four points and fixed using a 15 cm wide strap, making sure that the treatment head was fully in contact with the point. Connected the wires and pressed ‘on’ to start to work and it would stop 30 min later automatically. The treatment was conducted 3 times a week for a total of 12 sessions.
2.2 Traditional moxibustion group
Method: Patient took a supine position and naturally put the affected limb straight. A 4-hole moxibustion box of proper size was placed on the affected knee, with the holes pointing at the knee, and fixed by medical adhesive tape. Four moxa stick segments of 4-5 cm long were inserted into the holes respectively when successfully ignited. The ignited end of the moxa stick was 1-2 cm away from the skin. It usually took about 30 min for the moxa stick to burn completely, indicating the end of the treatment. The treatment was also conducted 3 times a week, for a total of 12 sessions.
3 Observation of Therapeutic Efficacy
3.1 Observation items
The two groups were evaluated using the visual analog scale (VAS) and Western Ontario and McMaster Universities osteoarthritis index (WOMAC) before treatment and after 6 and 12 sessions of treatment. The adverse reactions were also recorded.
3.1.1 VAS score
VAS was adopted to assess the improvement of pain. The scope of score was 0-10 points, ‘0’ indicating no pain while ‘10’ indicating unbearable pain. The higher the score, the more intensive the pain.
3.1.2 WOMAC score[13-14]
WOMAC consists of three domains, i.e. pain, stiffness and motor difficulty, covering all the primary symptoms and body signs of KOA. Among them, the domain of pain has 5 items, making a full score of 20 points; the domain of stiffness has two items, making a full score of eight points; the domain of motor difficulty has 17 items, making a full score of 68 points. The three domains together contribute 24 items, making a full score of 96 points. The higher the score, the more serious the disease condition.
3.1.3 Safety evaluation
The adverse reactions were recorded. Possible adverse reactions including topical and general symptoms were on close inspection, such as the treated site getting swollen and burns. Attention should also be paid in case there happened any other unexpected or significant adverse events.
3.2 Evaluation criteria of clinical efficacy
The weighed value of VAS score was calculated and clinical efficacy was evaluated on a 3-level scale: markedly effective, effective and invalid. The markedly effective rate and effective rate were counted. Nimodipine method was adopted for calculation[11]: Weighed value of VAS score = (Pre-treatment VAS score - Post-treatment VAS score) ÷ Pre-treatment VAS score × 100%.
Markedly effective: Weighed value of VAS score ≥50%.
Effective: Weighed value of VAS score ≥25% but <50%.
Invalid: Weighed value of VAS score <25%.
Markedly effective rate = Number of markedly effective cases ÷ Total number of group cases × 100%.
Total effective rate = (Number of markedly effective cases + Number of effective cases) ÷ Total number of group cases ×100%.
3.3 Results
3.3.1 Comparison of the VAS score
There was no significant difference comparing the VAS score between the two groups before treatment (P>0.05). Since the data conformed to spherical symmetry, two-factor repeated measurement analysis was applied. The intra-group comparisons of VAS score at different time points showed significant differences (P<0.01). The between-group comparisons of VAS score showed insignificant differences at different time points (P>0.05). The interaction between the two factors, group and time, did not produce statistical significance (F=1.451,P=0.795). The details are shown in Table 4.
The results showed that the electronic moxibustion apparatus and traditional moxibustion both can reduce pain in KOA patients, and the number of treatment sessions was notably associated with the relief of pain, i.e., the pain reduced with the increase of treatment sessions. Electronic moxibustion apparatus and traditional moxibustion produced similar efficacy in reducing pain in KOA.
3.3.2 Comparison of the WOMAC score
There was no significant difference comparing the WOMAC score between the two groups before treatment (P>0.05). Since the data conformed to spherical symmetry, two-factor repeated measurement analysis was applied. The intra-group comparisons of WOMAC score at different time points showed significant differences (P<0.01). The between-group comparisons of WOMAC score showed insignificant differences at different time points (P>0.05). The interaction between the two factors, group and time, did not produce statistical significance (F=2.143,P=0.137). The details are shown in Table 5.
The results showed that the electronic moxibustion apparatus and traditional moxibustion both can improve the joint function in KOA, and the number of treatment sessions was notably associated with the improvement of joint function, i.e., the joint function showed gradual improvement with the increase of treatment sessions. Electronic moxibustion apparatus and traditional moxibustion produced similar efficacy in ameliorating joint function in KOA.
Table 4. Comparison of the VAS score (±s, point)

Table 4. Comparison of the VAS score (±s, point)
Group n Pre-treatment After 6 sessions After 12 sessions F-value P-value Electronic moxibustion apparatus 38 5.95±1.08 4.53±1.16 3.07±1.27 234.736 0.000 Traditional moxibustion 34 5.68±1.17 4.45±1.22 3.22±1.30 F-value 0.068 P-value 0.241 Global analysis (HF coefficient) 0.756
Table 5. Comparison of the WOMAC global score (±s, point)

Table 5. Comparison of the WOMAC global score (±s, point)
Group n Pre-treatment After 6 sessions After 12 sessions F-value P-value Electronic moxibustion apparatus 38 46.58±11.38 32.18±10.39 19.71±10.36 406.54 0.000 Traditional moxibustion 34 42.53±11.84 30.91±12.60 19.53±11.04 F-value 0.523 P-value 0.472 Global analysis (HF coefficient) 0.733
There were no significant differences comparing the WOMAC component scores (pain, stiffness and motor difficulty) between the two groups before treatment (P>0.05). Since the data conformed to spherical symmetry, two-factor repeated measurement analysis was applied. The intra-group comparisons of WOMAC component scores (pain, stiffness and motor difficulty) at different time points showed significant differences (allP<0.01). The between-group comparisons of WOMAC component scores (pain, stiffness and motor difficulty) showed insignificant differences at different time points (allP>0.05). The interaction between the two factors, group and time, did not produce statistical significance. The details are shown in Table 6.
The results showed that the electronic moxibustion apparatus and traditional moxibustion both can improve the joint pain, stiffness and motor difficulty in KOA, and the number of treatment sessions was notably associated with the improvements, i.e., the improvements were gradually shown with the increase of treatment sessions. Electronic moxibustion apparatus and traditional moxibustion produced similar efficacy in ameliorating joint pain, stiffness and motor difficulty in KOA.
3.3.3 Comparison of the clinical efficacy
According to the weighed value of the VAS score, the markedly effective rate was 47.4% and the total effective rate was 89.5% in the electronic moxibustion apparatus group, and the markedly effective rate was 50.0% and the total effective rate was 94.1% in the traditional moxibustion group. There was no significant difference in the clinical efficacy between the two groups (P>0.05). The details are shown in Table 7.
3.3.4 Comparison of the clinical efficacy based on joint function grading
Prior to treatment, the patients in the two groups were classified into mild cases and severe cases based on joint function grading, i.e., those with joint function assessed higher than grade Ⅱ were taken as severe cases and those with joint function of grade Ⅱ or lower were taken as mild cases. There were no significant differences in the clinical efficacy in both mild cases and severe cases between the two groups (bothP>0.05), (Table 8). The results showed that electronic moxibustion apparatus and traditional moxibustion produced similar efficacy in treating KOA patients regardless of mild or severe cases based on joint function grading.
3.3.5 Comparison of the clinical efficacy based on radiographic staging of osteoarthritis
Prior to treatment, the patients in the two groups were classified into mild cases and severe cases based on radiographic staging of osteoarthritis, i.e., those with radiographic staging of osteoarthritis assessed higher than stage 2 were considered as severe cases and those of stage 2 or lower were taken as mild cases. There were no significant differences in the clinical efficacy in mild cases and severe cases between the two groups (bothP>0.05), (Table 9). The results showed that the two groups produced similar efficacy in treating KOA patients regardless of mild or severe cases based on radiographic staging of osteoarthritis.
3.3.6 Safety assessment
There did not happen any adverse events such as burns in the two groups during this trial, suggesting that the electronic moxibustion apparatus should be relatively safe taking master of the correct operation as the precondition.
Table 6. Comparison of the WOMAC component scores (±s, point)

Table 6. Comparison of the WOMAC component scores (±s, point)
Domain Group n Pre-treatment After 6 sessions After 12 sessions F-value P-value Pain Electronic moxibustion apparatus 38 9.68±2.81 7.00±2.76 4.05±2.40 423.15 0.000 Traditional moxibustion 34 8.94±2.90 6.68±2.78 4.35±2.53 F-value 0.617 P-value 0.219 Interaction 0.835 0.458 Stiffness Electronic moxibustion apparatus 38 2.92±1.48 1.89±1.20 1.13±1.07 402.96 0.001 Traditional moxibustion 34 2.65±1.30 1.76±1.10 1.03±0.97 F-value 0.811 P-value 0.324 Interaction 1.263 0.628 Motor difficulty Electronic moxibustion apparatus 38 33.92±8.44 23.24±7.43 14.37±7.57 398.95 0.000 Traditional moxibustion 34 30.97±8.65 22.56±9.27 14.15±8.09 F-value 0.472 P-value 0.237 Interaction 0.384 0.169

Table 7. Comparison of the clinical efficacy (case)

Table 8. Comparison of the clinical efficacy based on the joint function grading (case)
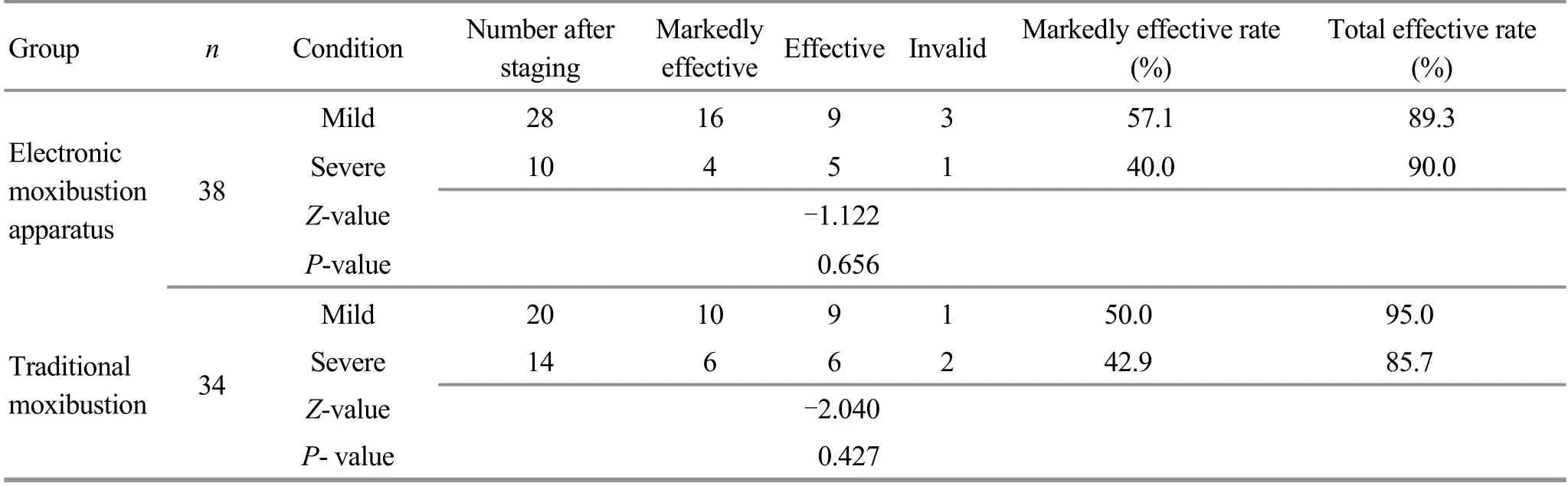
Table 9. Comparison of the clinical efficacy based on the radiographic staging of osteoarthritis (case)
4 Discussion
Moxibustion is a convenient and effective traditional external therapy. Either a moxa stick or a moxa cone, its major ingredient is mugwort. Mugwort is of warm nature, spicy and bitter in taste, going to the Liver, Spleen and Kidney Meridians. Its functions include dispersing cold with its spicy and warm nature, warming-unblocking meridians, warming meridians to cease pain, activating blood flow to treat pain or numbness, recuperating depleted yang, dissipating stasis and lumps, eliminating dampness to stop itching, and disease prevention and health protection.
KOA pertains to bone Bi-impediment or sinew Bi-impediment in the general scope of Bi-impediment syndrome, located in the bones and joints. It is reported that moxibution produces significant efficacy in treating KOA even used as monotherapy[5-8]. In recent years, researchers in both Chinese and Western medicine fields have conducted a large amount of studies and analyses discussing its action mechanism from multiple perspectives such as physics, molecular biology, metabolomics, genomics and imaging, which have successfully provided more theoretical and scientific evidences for treating KOA with moxibustion[15-17].
Though effective, traditional moxibustion has several shortcomings and is potential for modification. For example, patient having to stay in a limited position, difficulty unifying the treatment time and temperature, possible safety concerns, inhaling smog, and environmental pollution, etc. With the development of modern science and technology and widespread innovative concept, multi-disciplinary study to seek a greener, more environment-friendly, more convenient and effective moxibustion method has become the trend[18-20]. While summarizing the shortcomings of traditional moxibustion method, some scholars tried to innovate and develop novel moxibustion apparatuses. Li HJ,et al[21]invented DAJ-4 multi-functional moxibustion apparatus which can imitate and produce thermal effect, casting electromagnetic waves on acupoints and assisting to diffuse mugwort essential oil. Based on the study of thermal effect variance, they believe that this multi-functional moxibustion apparatus has physics foundation to produce more rapid effect than traditional moxibustion method. Moreover, its electromagnetic waves can directly strengthen the neurohumoral microcirculation in human body, an effect that the traditional moxibustion therapy cannot exert. Le XY[22]also used novel DAJ multi-functional moxibustion apparatus to treat KOA, and the results showed that there was no significant difference in the efficacy between the moxibustion apparatus and traditional warm needling method, but a significant difference was found between the moxibustion apparatus and electroacupuncture.
In this trial, DZWJY-1 type electronic moxibustion apparatus invented by Yang XM,et al[12]was adopted. This apparatus is composed of 8 treatment headers, electronic temperature controller on the inside and a color touch LCD on the outside. The treatment headers can imitate traditional moxibustion to produce thermal infrared radiation; mugwort essential oil patches are applied during treatment; the electronic temperature controller can precisely modulate the treatment temperature of the heads, which is somewhat innovative regarding unification; the color touch LCD makes it convenient to set the temperature and time, which enables to simplify the operation.
The current study has found the following advantages of DZWJY-1 electronic moxibustion apparatus. First, it is relatively standardized. This apparatus has imitated the thermal infrared radiation of the traditional moxibustion and concurrently achieves the standardization of temperature and time that traditional moxibustion cannot do. Second, it is more environment-friendly. Traditional moxibustion produces ‘smoke’ and ‘dust’ during the treatment process, which makes patients and physicians avoid to use moxibustion, so that the application of moxibustion has shrunk. Electronic moxibustion apparatus has solved these problems and is greener and more environment- friendly. Third, it is comparatively safer. Traditional moxibustion has a naked flame at the ignited part and the dust may burn the sheet when falling on the bed. Therefore, it is a big fire and security concern for moxibustion treatment room. However, the electronic moxibustion apparatus produces a maximum temperature of 55 ℃ at the treatment header, which is a relatively safe temperature that will not cause burn of fabrics. Fourth, it is easy-to-operate. During the treatment with traditional moxibustion, medical staff need to stay closely to monitor the treatment condition, to make sure that the moxa is neither too far to lessen the treatment efficacy nor too close to cause a burn, which restricts the number of patients at one treatment time. Electronic moxibustion is more convenient since it offers a stable topical temperature and turns off automatically at the end of treatment, and there is no need for medical staff to take care of it repeatedly. Fifth, the human-centered design. The five treatment headers of this electronic moxibustion apparatus can adjust its temperature separately, which allows it to set the temperature to satisfy the needs of different body parts according to the sensitivity to temperature. Sixth, economical advantage. Although traditional moxibustion method costs lower, the hospital needs to pay for it continually. By contrast, once this electronic moxibustion apparatus is purchased, it is almost once and for all and the maintenance cost is lower.
This study has proven that electronic moxibustion apparatus and traditional moxibustion method both can effectively reduce pain and improve joint function in KOA patients and they are equivalent comparing the clinical efficacy. This study has also managed to provide certain supports for further study, systemization and standardization in using electronic moxibustion apparatus to treat KOA.
Conflict of Interest
There is no potential conflict of interest in this article.
Acknowledgments
This work was supported by Natural Science Foundation of Shanghai ( 上海市自然科学基金课题, No. 18ZR1436200); Shanghai Project of Dominant Disease in Chinese Medicine [上海市中医优势病种培育项目, No. ZY(2018-2020)-ZYBZ-24]; The Third Batch of ‘Famous Doctor’s Studio’ of Changning Health and Family Planning Commission, Shanghai (上海市长宁区卫生计生行业第三批“名医工作室”,2018 年度“名医”计划); Science Foundation of Changning Health and Family Planning Commission, Shanghai (上海市长宁区卫生和健康委员会科研课题, No. 20194Z006).
Statement of Informed Consent
Informed consent was obtained from the patients in this study.
Received: 24 October 2019/Accepted: 18 December 2019
猜你喜欢
杂志排行

Journal of Acupuncture and Tuina Science的其它文章
- Effect of electroacupuncture at Lower He-Sea points including Yanglingquan (GB 34) on nuclear factor-κB and interleukin-1β in guinea pigs with acute cholecystitis
- Study on the differences between moxibustion at different points in the effects on the anti-fatigue ability of rats undergoing one-time exhaustive swimming
- Clinical observation on herb-partitioned spreading moxibustion at Baliao points plus climen for diminished ovarian reserve
- Therapeutic efficacy of moxibustion plus medicine in the treatment of infertility due to polycystic ovary syndrome and its effect on serum immune inflammatory factors
- Clinical study on auricular point sticking plus Western medicine for moderate gastric cancer pain
- Clinical observation on filiform fire-needling plus continuous passive motion therapy for frozen shoulder