Atypical presentation of SARS-CoV-2 infection:A case report
2020-04-23RuiLinLiShuGuangChuYuLuoZhenHaoHuangYingHaoChengHuiFan
Rui-Lin Li,Shu-Guang Chu,Yu Luo,Zhen-Hao Huang,Ying Hao,Cheng-Hui Fan
Rui-Lin Li,Yu Luo,Zhen-Hao Huang,Ying Hao,Cheng-Hui Fan,Department of Cardiology,Shanghai East Hospital (East Hospital affiliated to Tongji University),Tongji University,Shanghai 200123,China
Shu-Guang Chu,Department of Medical Imaging,Shanghai East Hospital (East Hospital affiliated to Tongji University),Tongji University,Shanghai 200123,China
Abstract
Key words: SARS-CoV-2;COVID-19;Pneumonia;Ground-glass opacity;Atypical symptoms;Diarrhea
INTRODUCTION
The first case of coronavirus disease 2019 (COVID-19) was reported in Wuhan,Hubei Province on December 8,2019.The symptoms included fever,coughing,and breathing difficulties[1-3].Subsequently,more cases emerged,clustering from the Huanan Seafood Market in Wuhan[4].On January 2,2020,the first 41 cases of COVID-19 were confirmed.The Wuhan Institute of Virology collected severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) samples,and on January 2,2020,its genome was successfully sequenced.The virus strain was then successfully isolated on January 5,2020.However,the origin of coronaviruses remains unclear,although many reports in the literature suggest that they are likely to be fromRhinolophus sinicus[5].Coronaviruses are a family of RNA viruses that have been previously identified as having six subtypes,with SARS-CoV-2 now thought to be the seventh.Four of the six subtypes are less pathogenic and usually result in mild catarrhal presentation after infection.Two previously identified viral subtypes,known as the viruses causing Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS)[6-8].On January 12,the World Health Organization named the virus discovered in Wuhan “Novel Coronavirus 2019 (2019-nCoV),” which is able to cause an acute respiratory disease[9-11].Subsequently the virus was named SARS-CoV-2 and the disease COVID-19.On January 21,China's National Health Commission (NHC) issued a notice that the novel coronavirus pneumonia virus was included in the Class B infectious diseases,but the prevention and control measures were adopted for Class A infectious diseases.Understanding the diagnostic criteria for SARS-CoV-2 is particularly important,as it can lead to an appropriate clinical diagnosis and treatment.The fourth version of the COVID-19 diagnostic criteria issued by the NHC are as follows:(1) Two weeks prior to the onset of the disease,the patient had travelled to Wuhan City,has a history of residence in Wuhan,has been exposed to patients with respiratory symptoms in Wuhan,or has been near a disease cluster;and (2) Clinical manifestations:(a) Fever;(b) Having imaging features of pneumonia;and (c) The total number of white blood cells in the early stages of the disease is normal or decreasing,or the number of lymphocytes has decreased.The disease can be considered ascertained if the patient has one of the epidemiological features and shows two clinical manifestations.Here,we report a patient diagnosed with SARS-CoV-2 infection who had atypical symptoms of diarrhea and did not have any respiratory symptoms.
CASE PRESENTATION
Chief complaints
A 74-year-old woman presented with severe diarrhea for 3 d.
History of present illness
The patient was visiting Shanghai from Wuhan.She presented to the Outpatient Department of Shanghai East Hospital on January 26,2020 and complained of three days of severe diarrhea,with watery stools passed five to six times per day and sometimes blood-stained.The cause of these symptoms was unknown.The diarrhea was accompanied by anorexia and fatigue.The patient had taken eight pills of Huo Xiang Zheng Qi Wan,a natural herbal supplement that helps restore energy,three times a day,but without any symptomatic improvement.She denied having had any unhygienic food,seafood,or visiting the seafood market in Wuhan.The patient had no fever or cough,no sore throat,no chest tightness,and no shortness of breath.
Epidemiological history
On January 9,the patient's son visited a colleague who lived in downtown Wuhan and who was reported to have not visited the Huanan Seafood Market within at least 2 wk.The son's colleague was diagnosed with severe pneumonia,which was later confirmed to be COVID-19 and was put on a ventilator.The patient's son had not taken any preventative measures on January 9 while meeting with his colleague.The patient travelled with her son,daughter,and granddaughter from Wuhan to Shanghai by train on January 23 after hearing about a possible Wuhan lockdown.Her son showed symptoms of anorexia and fatigue on January 21,and diarrhea with bloody stools on January 23,which lasted for several consecutive days and improved after taking oral moxifloxacin for four days.The patient's husband developed fever on January 27 and was diagnosed with SARS-CoV-2 infection on January 30 (Table 1).The patient's daughter and granddaughter remained asymptomatic.
History of past illness
The patient had been hypertensive for more than 10 years.Her blood pressure was well controlled at 120-130/80-90 mmHg (15.99-17.33/10.66-11.99 kPa) with oral amlodipine 5 mg/d.The patient had no history of chronic digestive diseases,or other systemic diseases.
Personal and family history
The medical history of the patient was unremarkable.
Physical examination upon admission
Blood pressure was 153/94 mmHg,respiratory rate 24/min,heart rate 93/min,temperature 36.7 °C,and oxygen saturation was 99%.The patient was conscious and had a clear mind.She was low in spirit but had smooth breathing,no features of anemia,regular heart rhythm without any obvious murmur,no obvious moist crackles or wheezing sounds during auscultation of both lungs,and a soft abdomen.The patient felt pain when pressure was applied on the upper and middle abdomen although no rebound tenderness and no obvious lumps were detected.
Laboratory examinations
Routine blood test results were as follows:White blood cells,3.50 × 109/L;neutrophils:58.5%;lymphocytes,33.9%;total number of lymphocytes,1.19 × 109/L;fast C-reactive protein,34.18 mg/L;serum amyloid proteins,45.96 mg/L;potassium,3.6 mmol/L;sodium,136 mmol/L;chlorine,97.0 mmol/L;creatinine,43 µmol/L;urea,3.1 m/L;total protein,77 g/L;albumin,44 g/L;alanine aminotransferase,48 U/L (reference value 9-52 U/L);aspartate aminotransferase,44 U/L↑(reference value 14-36 U/L).Blood tests for rapid detection of influenza A,influenza B,respiratory syncytial virus,mycoplasma pneumonia and adenovirus were all negative.
Clinical diagnosis
The patient was first diagnosed with gastrointestinal dysfunction,which is commonly seen in the Emergency Department and may be due to a cold,long-distance travels,an irregular diet,change in eating habits.However,considering her close proximity to the epidemic area,atypical pneumonia virus infection had to be ruled out.A computed tomography (CT) scan was performed on January 26,and showed small ground-glass nodules scattered along the two lungs,suggesting viral pneumonia(Figures 1 and 2).Given the clinical characteristics,epidemiological history,and examination,the patient was hospitalized with the diagnosis of suspected SARS-CoV-2 infection.
FINAL DIAGNOSIS
On January 27,nucleic acid testing by the Centers for Disease Control and Prevention(CDC) gave positive results.Thus,the diagnosis of SARS-CoV-2 infection was confirmed.Then,in accordance with the CDC's advice,the patient was transferred to the Shanghai Public Health Center for further comprehensive treatment.
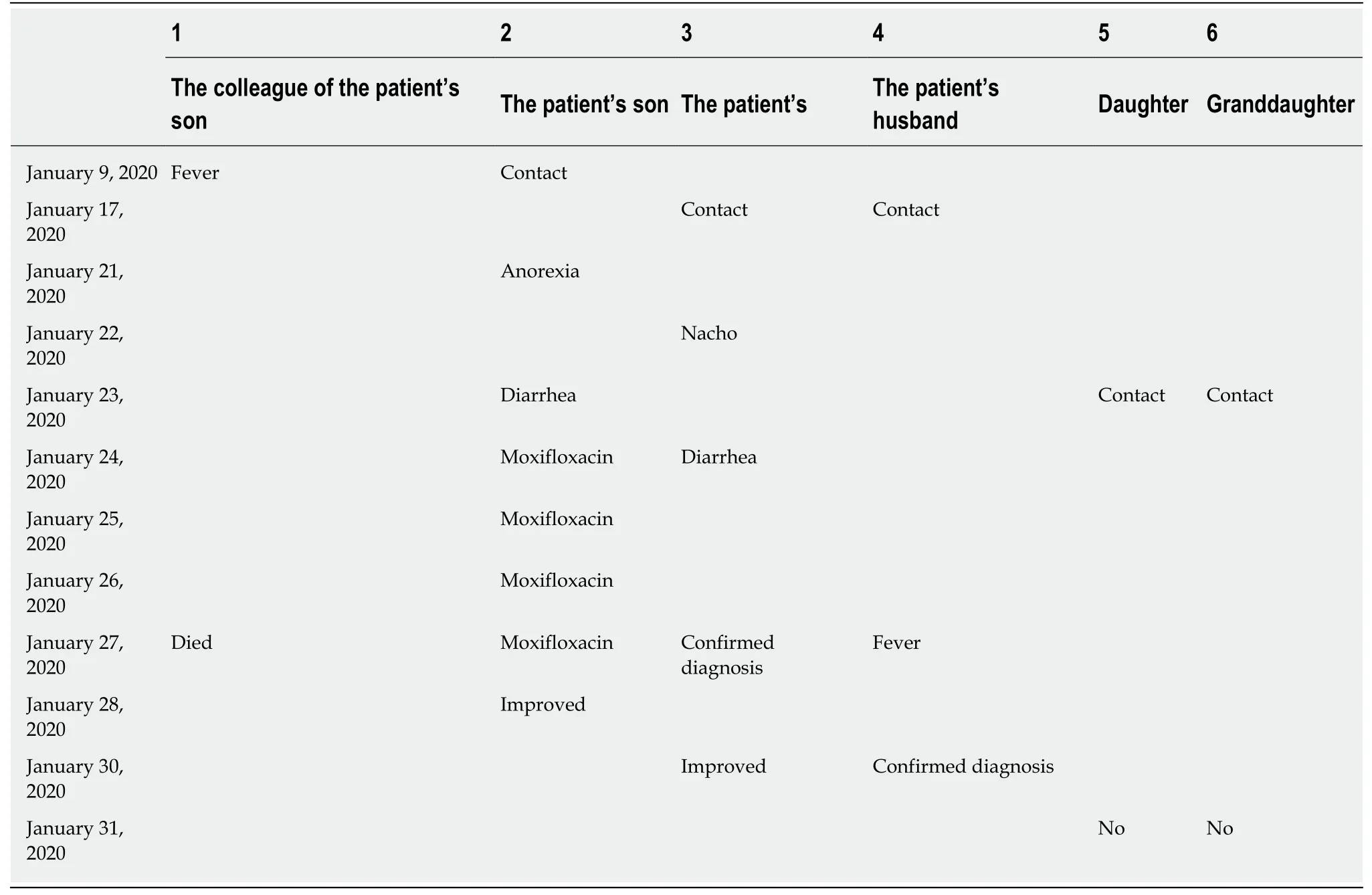
Table1 Timeline of symptoms
TREATMENT
The patient was given 0.4 g QD moxifloxacin i.v.and 0.2 g TID oral Arbidol during inhospital treatment.She was also treated with lopinavir/ritonavir (200/50 mg)(Kaletra) according to the fourth version of the NHC treatment plan.
OUTCOME AND FOLLOW-UP
After eight days of treatment,the patient's symptoms improved significantly,and she recovered with negative nucleic acid test.By the time of this paper submission,she was waiting to be discharged from hospital.
DISCUSSION
SARS-CoV-2-infected patients rarely show intestinal symptoms,such as diarrhea,while lacking respiratory signs/symptoms,whereas about 20%-25% of patients infected with MERS-CoV or SARS-CoV have diarrhea.According to current reports,COVID-19 has different clinical manifestations,such as fever,cough,fatigue,and breathing difficulties.A small proportion of patients have sore muscles,headache and a sore throat.In rare cases,patients have no typical symptoms and can only be confirmed by nucleic acid testing and/or a CT scan.Therefore,clinicians should be aware of the atypical characteristics of SARS-CoV-2 infection,especially in patients with epidemic contact history.By February 7,the number of confirmed cases had surged to more than 33000 with a further 27657 awaiting confirmation.The rate of both newly confirmed and suspected cases has been declining.No drug has been definitively shown to be effective for the treatment of this virus and thus only a small number of patients have been cured and discharged.The local and central government of China have implemented strict measures in order to curb the outbreak.However,it is an enormous challenge to trace all the people who might have been in contact with the virus after hundreds of thousands of cases have been confirmed or remained to be confirmed.It may be that the virus can spread not only via respiratory droplets,but also through fecal-oral transmission,contact transmission,and aerosol transmission.Asymptomatic patients seem to be able to also spread the virus via the above-mentioned routes.Patients presenting with atypical symptoms can be misdiagnosed,causing further spread of the virus.Current medical care includes inhaling nebulized interferon (five million BID) and Lopinavir/Ritonavir (200/50 mg)(Kaletra),even though there is no proof of their effectiveness.However,there is a report of a 35-year-old man that returned to the United States after visiting his family in Wuhan and was treated with Remdesivir (Gilead),a nucleotide analogue that inhibits the RNA-dependent RNA polymerase (RdRp).After the treatment,the patient showed significant improvement[12,13].This drug was previously used to treat Ebola,which also has an RdRp activity.Therefore,this drug may also inhibit SARSCoV-2[13,14].However,the drug is still under a clinical trial,and its true effects need to be verified.Doctors have also verified the presence of SARS-CoV-2 (positive RT-PCR results) in stool samples of patients with diarrhea,which confirms the possibility of fecal-oral transmission.

Figure1 Ground-glass nodules are randomly distributed in the upper and lower lobes of the two lungs and the pleural membrane.
CONCLUSION
COVID-19 symptoms include fever,cough,dyspnea,and atypical manifestations such as diarrhea.Therefore,detailed medical history taking,careful physical examination,and critical clinical evaluation will enable a correct diagnosis.

Figure2 Magnified image of typical ground-glass computed tomography characteristics.
杂志排行

World Journal of Clinical Cases的其它文章
- Sarcopenia in patients with colorectal cancer:A comprehensive review
- Thoracic hydatid disease:A radiologic review of unusual cases
- Clinical significance and prognostic value of tumor necrosis factor-α and dickkopf related protein-1 in ankylosing spondylitis
- Reconstruction of Paprosky type lllB acetabular bone defects using a cup-on-cup technique:A surgical technique and case series
- Depression and myocardial injury in ST-segment elevation myocardial infarction:A cardiac magnetic resonance imaging study
- Long-term survival of two patients with recurrent pancreatic acinar cell carcinoma treated with radiofrequency ablation:A case report