Bone alterations in inflammatory bowel diseases
2019-08-14DoloresSgambatoFrancescaGimiglianoCristianaDeMusisAntimoMorettiGiuseppeToroEmanueleFerranteAgneseMirandaDomenicoDeMauroLorenzoRomanoGiovanniIolasconMarcoRomano
Dolores Sgambato,Francesca Gimigliano,Cristiana De Musis,Antimo Moretti,Giuseppe Toro,Emanuele Ferrante,Agnese Miranda,Domenico De Mauro,Lorenzo Romano,Giovanni Iolascon,Marco Romano
Abstract
Key words: Inflammatory bowel diseases; Bone alterations; Bone mineral density;Osteoporosis; Osteopenia; Ulcerative colitis; Crohn’s disease
INTRODUCTION
Inflammatory bowel diseases (IBDs) are mainly represented by Crohn’s disease (CD)and ulcerative colitis (UC),both characterized by a multifactorial,partially unknown etiology that involves genetic,immunological and environmental factors including intestinal microbiota[1].A dysregulated immune response to an unknown trigger leading to a sustained pro-inflammatory response within the gastrointestinal (GI)tract seems to play a major pathogenic role.Also,10%-40% of IBD patients may suffer from at least one extraintestinal manifestation (EIM)[2],even before the occurrence of the intestinal disease[3].
Among the most frequent EIMs,there are those affecting the musculoskeletal system and in particular the bone tissue,such as osteoporosis (OP)[4].
OP is a systemic disease characterized by an increased risk of fractures even after a low energy trauma (fragility fracture).The reduction of bone strength is a consequence of a decrease in bone mineral density (BMD) and a deterioration in bone quality[5].According to the World Health Organization the operational diagnosis of OP is based on BMD values equal or lower than 2.5 standard deviations (SD) from the average values for young healthy women (T-score < -2.5 SD) in post-menopausal women and men aged ≥ 50 years,while,osteopenia is defined by BMD values between -1 to -2.5 SD (T-score -1< and > -2.5).
BMD is measured trough dual-energy X-ray absorptiometry (DXA)[6,7]; T-score is a parameter comparing the BMD of a given patient with the average bone density of young healthy adults of the same sex,while,Z-score compares each BMD with the average BMD of a person with the same age and sex[8].
OP is classified into two main groups:Primary (or idiopathic) and secondary.The first one is the most common and includes juvenile,postmenopausal and senile OP.Secondary OP might be caused by several conditions (i.e.,endocrine,hematological,GI,rheumatic or renal diseases) that negatively affect bone metabolism leading to poor bone strength.Other causes might be the chronic use of some medications,particularly glucocorticoids (GCs),anticoagulants,and anticonvulsants[9,10].Therefore,the term “secondary OP” refers to all those clinical conditions in which the bone involvement is a consequence of the primary disease or results from the related treatments (i.e.,GCs).Secondary OP affects about 60% of males and more than 50% of premenopausal women[11,12].
In IBD population,there are several pathological mechanisms that might result in low BMD and poor bone strength,thus leading to OP.
This review aims to summarize the prevalence and pathophysiology of metabolic bone alterations in IBD subjects outlining their main risk factors.We also underline the role of the screening and prophylaxis of BMD in CD and UC patients and the importance of early treatment.
EPIDEMIOLOGY
OP is one of the most common noncommunicable diseases[13]and its incidence is increasing worldwide[14].According to Svedbomet al[15],22 million women and 5.5 million men were estimated to have OP in Europe,with a reported incidence of 3.5 million new osteoporotic fractures in 2010,(620000 hip fractures,520000 vertebral fractures,560000 forearm fractures and 1800000 fractures in other skeletal sites).OP and its consequences (i.e.,fractures) carry a considerable economic burden on the health care systems[15]and,in particular,the socioeconomic costs of an osteoporotic hip fracture are equivalent to those of myocardial infarction and stroke[16].
In IBD subjects,the prevalence of low BMD ranges from 22% to 77% and that of fragility fractures from 17% to 41%[17].These wide ranges across different studies might be explained by the small number of samples and by the heterogeneity of the studies and of the populations.
Several studies have been performed to describe the relationship between IBD and bone alterations.Shethet al[2]showed that both osteopenia and OP are frequently associated with IBD,ranging from 32% to 36% for osteopenia and from 7% to 15% for OP.The same study reported an increased relative risk of fragility fractures in CD patients and a prevalence of < 0.5% for osteonecrosis,a clinical condition characterized by the death of the bone tissue,commonly described as a complication of steroid therapy in IBD patients.A study of Boubakeret al[18]reported that in a Tunisian group of 67 patients,OP represented the most frequent EIM in CD patients with a prevalence of low BMD at hip and spine in 31.8% and 40.9% of cases,respectively.OP is strongly associated with CD in females,thus suggesting that female gender might be one of the risk factors for bone loss in IBD.A prospective study in Romania found osteopenia in 48.07% of UC patients and in 56.41% of CD patients,while OP was shown in 18.26% of UC patients and in 15.38% of CD patients[19].A Swiss IBD cohort study performed on 877 patients showed a prevalence of bone density alteration in 20% of IBD patients and identified,by multivariate logistic regression analysis,corticosteroid usage,long disease duration and perianal disease as independent risk factors[4].A Japanese study reported that two-thirds of IBD patients showed a loss of BMD,with a prevalence of OP of about 13% in their cohort of patients with mean age of 43 years.The prevalence of OP is more frequent in Western IBD population than in the Asiatic one[20]and,therefore,the prevalence of bone metabolism alterations generally varies depending on study population,location and design of the study performed.
Notably,the risk of fragility fractures seems to be increased in IBD population[21]although the literature shows controversial results.Recently,Komakiet al[22]showed that there was no increase in the risk of overall fractures in IBD patients,but they reported more fractures at the spine,associated with steroids therapy.
Pediatric IBDs seem to show a similar association with osteopenia and OP as in adults.In fact,it is known that children with IBD have a higher risk of low BMD[23].The overall prevalence of osteopenia and OP in pediatric and young IBDs patients seems to vary from 20% to 50%[24].A recent study suggested a positive association between BMD and physical activity and between low BMD and fractures in the childhood[25].Incidence of fragility fractures is higher in the young IBD population and is likely to be associated to the use of GC[26,27].Pediatric CD patients appear to be more severely compromised than those with UC,probably because CD inhibits linear growth more frequently than UC[28].
CD and UC,while being both classified as IBDs,show considerable differences in the anatomic location and distribution of the intestinal lesions as well as in the underlying pathogenic mechanisms.This might have an influence on the incidence of bone alterations in each condition.Bjarnasonet al[29]described no significant differences in T scores for spine or hip between patients with CD and those with UC.On the other side,in a study by Jahnsenet al[30],BMD resulted significantly reduced in CD subjects at all measured sites compared with UC patients,and healthy subjects.Interestingly,the authors did not describe significant differences in BMD between UC and healthy subjects.Ardizzoneet al[46],in Italy,evaluated differences between CD and UC with respect to the pathogenic mechanisms underlying bone loss.Crohn’s Disease Activity Index (CDAI)[31]and Truelove and Witts’ Score[32]were used to grade disease activity of CD and UC,respectively.The distribution of normal,osteopenic and osteoporotic BMD values among CD and UC showed no significant differences also between patients with different disease activity.Also,in a study conducted in Sri-Lanka,there were no significant statistical differences in the frequency of OP between CD and UC,whereas the occurrence of OP among IBDs patients (13.5%) was higher than in healthy controls[33].Recently,Vázquezet al[34]did not find any difference between patients with CD and those with UC regarding the prevalence of alterations of bone density.
The discrepancy between different studies may be due to variability in patient selection,differences in the methods used to evaluate bone density,and the body sites studied at DEXA (i.e.,radiusvslumbar spine or hip).
PATHOPHYSIOLOGY
Both bone quality and quantity (BMD) depend on physiological mechanisms,such as bone modeling and remodeling that in turn are regulated by biochemical and mechanical factors,including osteoprotegerin (OPG),receptor activator of nuclear factor kappa-B ligand (RANKL),receptor activator of nuclear factor kappa-B (RANK),and weight bearing activities.In particular,the RANKL secreted by osteoblasts binds to the RANK receptor,located on pre-osteoclasts and mature osteoclasts,inducing osteoclast proliferation,activity and survival.OPG,a molecule secreted by osteoblasts,modulates bone turnover by inhibiting the binding of RANKL to RANK.The balance between OPG and RANKL release regulates osteoclast activity that in turn can be influenced by several hormones and cytokines,including vitamin D,estrogens,testosterone,GCs,parathormone (PTH),as well as pro-inflammatory mediators,such as interleukin-1 (IL-1) and tumor necrosis factor-alfa (TNFα).In OP,an imbalance between the serum levels of OPG and RANKL occurs,with excessive bone resorption and impaired bone formation,with consequent overall reduction of bone mass[35].
Other key modulators of bone turnover are the Wnt/β-catenin signaling and sclerostin,which acts mainly on osteoblasts and osteocytes.Sclerostin is a glycoprotein produced almost exclusively by osteocytes and its expression is influenced by many factors,including serum PTH and mechanical loading[36].Animal studies have shown that the mechanical load reduces serum sclerostin,whereas unloading increases the transcription ofSOST,the gene encoding for sclerostin.Once secreted,sclerostin through osteocyte canalicular system reaches the bone lining cells (capable of activation into mature osteoblasts),where it binds to specific co-receptors (LRP-5 and -6) to inhibit the Wnt pathway,with consequent reduction of osteoblastogenesis and bone formation.On the contrary,a reduction in sclerostin levels is associated with an activation of the Wnt/β-catenin pathway with subsequent enhancement of osteoblast activity and survival[37].Moreover,there is a correlation between hypersclerostinemia and bone loss in subjects forced to prolonged immobilization,thus supporting the key role of sclerostin in the development of OP following reduced mechanical load[38].
Among the most frequent secondary forms of OP,GCs use has been shown to decrease the number of osteoblast precursors and to increase the apoptosis of mature osteoblasts.The reduction in osteoblast differentiation is in partly mediated by the inhibition of the Wnt/β-catenin pathway along with increased expression of sclerostin,that antagonizes the Wnt signaling[39].On the other hand,GCs decrease also osteoclast proliferation,although their activity tends to increase,through both the increase in RANKL and the reduction of OPG levels[40].During GCs therapy,bone loss occurs rapidly with BMD reduction of 6%-12% within the first year,followed by a constant and gradual loss throughout the treatment period[41].These two pathways are the basis of the most modern pharmacological approaches to OP:A human monoclonal antibody against the RANKL (denosumab) and a humanized monoclonal antibody that targets sclerostin (romosozumab).
Among the most frequent causes of secondary OP there are GI disorders,including IBDs.Chronic gut inflammation in IBD may contribute to OP through the activation of T lymphocytes resulting in enhanced release of inflammatory cytokines,such as TNFα,that modulates the OPG/RANKL/RANK pathway thus inducing bone loss[42](Figure 1).Moreover,TNFα enhances sclerostin production that results in decreased bone formation.Interestingly,in patients affected by CD,bone loss occurs before GCs administration,supporting the detrimental role of systemic inflammation on bone health[43].
There is a close relationship between bone and GI system that allows calcium absorption and bone mineralization; the GI tract may communicate with bone tissue through different mechanisms such as blood,nerves and immune cells,defining a characteristic gut-to-bone signaling axis that involves also incretins,serotonin and GI microbiota[44](Figure 2).

Figure 1 Modulation of osteoclast differentiation by serum TNF-α and anti-TNF-α treatment.
Although in the general population female sex,early menopause,hormonal imbalance,smoke and old age are the main risk factors correlated with the onset of metabolic bone disease (MBD),in IBD patients the main risk factor seems to be the prolonged use of GCs[45,46].Activity and severity of gut inflammation,intestinal malabsorption and calcium and vitamin D deficiency are also directly involved in the loss of BMD[47,48].In particular,in CD the involvement of the terminal ileum may affect the bile salt enterohepatic circulation thus leading to a reduced absorption of vitamin D.Chronic inflammation seems to have a key role in the reduction of BMD as suggested in some studies that show that rat models with colitis have a drastic loss of trabecular bone and a suppression of bone formation.At resolution of colitis with mucosal healing,the bone formation regresses to normal levels.During gut inflammation some mediators that alter the deposition of new bone matrix mediated by osteoblasts are produced,such as IL-6 and RANKL[49].
Untreated inflammation may be the main determinant for the loss of BMD in IBDs.In fact,a study by Ghoshet al[43]showed that CD patients have very low T-scores at the diagnosis before any drug therapy.Several studies in last years have also demonstrated that the usage of anti-TNF agents seems to have a positive effect on BMD[50](see below).Recent studies suggest a role for the inflammatory process in the alteration of bone metabolism through the involvement of immune system cells,however it is not clear whether the inflammation is directly involved in the loss of BMD or if other factors contribute to the decline of BMD in IBD patients.
Bone alterations in IBD population appear to have a multifactorial etiology:Genetic factors,gut-bone immune signaling interaction,inflammation-related bone resorption,multiple intestinal resections,microbiota and pathogenic micro-organisms interaction,and dietary malabsorption of minerals[51,52](Figure 2).
However,the main factor that seems to directly affect bone metabolism,with consequent reduction in BMD values,is corticosteroid treatment.In the following paragraphs we will summarize the evidence linking these factors to BMD deterioration in IBD patients.
Main risk factors
Genetic factors:The literature concerning the genetic predisposition to OP in IBD patients appears rather contradictory.A number of polymorphic sites apparently associated with the increased risk of bone loss in IBD patients such asIL-6andIL-1rahave already been described[53].Todhunteret al[54]showed that the polymorphisms identified in some genes such asCOL1A1andIL-6seems to influence BMD in IBD patients,particularly those with CD.Nemetzet al[55]showed also an increased risk of bone loss in patients withIL1Bpolymorphism (IL1B-511*2) associated with hypersecretion ofIL1B.
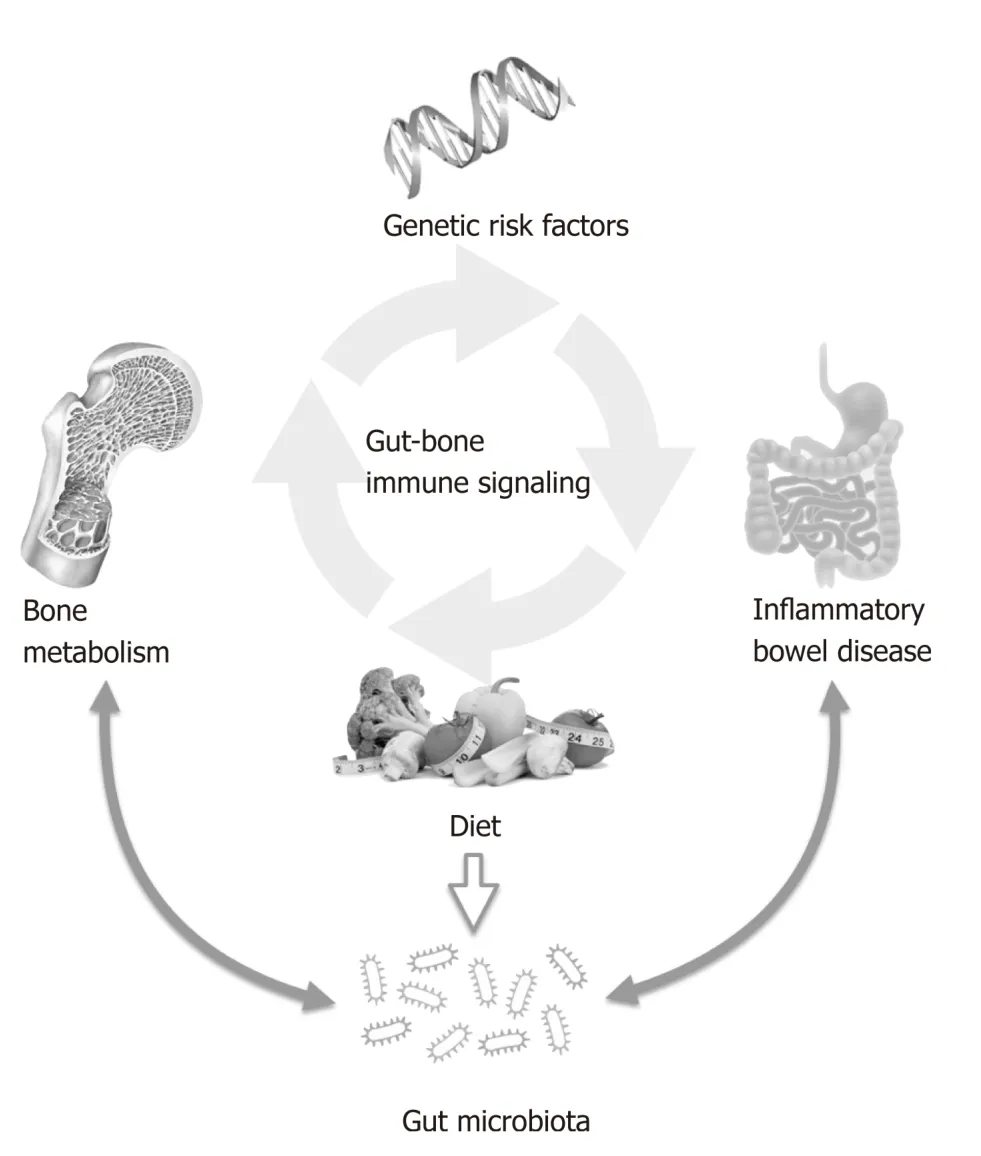
Figure 2 Gut-bone immune signaling: interplay between different factors which may affect bone metabolism in patients with inflammatory bowel diseases.
One of the latest genetic factors associated with OP development is OPG encoded by the geneTNFRS11B,where the polymorphism c.-223C>T in 5’ UTR region was identified as strongly related to OP in postmenopausal women.However,the genotyping analysis did not show unequivocal association between c.-223C>T ofTNFRS11Band a predisposition to OP in IBD patients,although this polymorphism is more frequent in IBD patients than in healthy controls[56].Krela-Kaźmierczaket al[56]studied the relationship between different polymorphic variants ofTGFB1 and bone loss in IBD,finding no significant differences in BMD values or in the risk of fragility fractures between UC and CD patients and healthy controls with different polymorphic variants of theTGFB1gene.Moreover,no association between the 29T>C polymorphic variant ofTGFB1and BMD of spongy bone and cortical bones was found[57].
The gene encoding for bone morphogenetic protein 2 (BMP2) was analyzed using restriction fragments length polymorphisms (RFLPs) to determine the association among the incidence of 570 A>T polymorphism,BMD alterations,and the incidence of fractures in IBD patients.The analysis revealed no significant association between this polymorphism and changes in bone metabolism in both UC and CD patients[58].
An interesting and recent theory correlates the presence of genetic alterations that might affect the ability to respond to endoplasmic reticulum (ER) stress and normal bone tissue physiology in IBD patients.A recent meta-analysis focused on the association between the genes involved in the response to unfolded proteins (UPR)and ER stress,which could directly correlate with the pathogenesis of IBDs[59].It was suggested that the same defects in the Paneth cells inherent in UPR may also be present in bone cells,both osteoblasts and osteoclasts (although this has not yet been confirmed in IBD)[60].Although its polymorphic variant seems to have no direct association with BMD,BMP2 activates the UPR during osteogenesis[61]allowing the production of RANKL[62].In conclusion,during osteoblast differentiation ER stress is induced and activates also the PERK-eIF2α-ATF4 pathway that appears as a potential target against bone diseases[61].To date,the association between genetic factors and bone alterations in IBD patients is not clear and other risk factors must be taken into account,such as those related to nutrition and lifestyle,as well as the ethnodemographic characteristics.
Gut-bone immune signaling:Bone structure depends on the balance between osteoblasts activity,specialized in the deposition of new bone matrix and osteoclasts,responsible for the resorption of bone tissue.Mounting evidence suggests an immunological involvement in the alteration of bone metabolism[63].Activated CD4+cells appear to be important actors in the bone loss related to IBD.In fact,in mice models,bone marrow CD4+ cells producing IL-17 and TNF-α migrate into the bone marrow during the inflammation,promoting the recruitment of monocytes as osteoclast progenitors,thus contributing to the bone loss[64].Ashcroftet al[65]reported that activated T cells,producing RANKL,are accumulated in the bone marrow during intestinal inflammation.
As already discussed,osteoclastogenesis is guided by the RANK-RANKL pathway and by the RANKL/OPG ratio.OPG produced by osteoblasts works as a decoy receptor for RANKL,thus interfering with osteoclast activation.Liet al[66]suggested that lymphocytes might work as key regulators of bone metabolism by interfering with this pathway.In particular,they found that over 60% of OPG is produced by B lymphocytes and that T lymphocytes stimulate OPG production by osteoblasts via CD40L/CD40 co-stimulation.Finally,they showed that B-cells as well as CD40 or CD40L knockout mice developed OP and OPG deficiency[66].
Current knowledge strongly suggests a dynamic interplay between skeletal and immune system which is referred to as osteoimmunology.IL-17-producing helper T cells [T(H)17] induce RANKL,stimulating osteoclastogenesis through nuclear factor of activated T cells cytoplasmic 1 (NFATc1)[67].There is evidence of activation of NFAT2 in lamina propria mononuclear cells of subjects with UC[68].
All these studies seem to show,in IBD,a direct involvement of immune system in the bone loss,mainly due to CD4+ cells that appear osteoclastogenic during inflammation.
Microbiota and pathogenic micro-organisms: The human microbiota consists of a set of about 100 trillion of commensal micro-organisms belonging to different species,which express a genome of about a hundred times greater than that expressed by the host’s cells.There is evidence that alterations of the microbiota composition influence the healthy state of the host[69].
In particular,an immune response to an altered intestinal microbiota or an alteration of the immune response leading to its activation in the face of a normal intestinal microbiota both leading to a sustained inflammatory process,have been suggested as the main pathogenic mechanisms for the development of IBD[70].
Several studies suggest a key role for microbiota in the alteration of BMD.Irwinet al[71]reported a close correlation betweenH.hepaticusinfection and bone loss.McCabeet al[72]showed that treating healthy male mice withLactobacillus reuterienhanced bone density and suppressed basal TNFα mRNA levels in male mice,but not in females.They also showed that probiotics increased male trabecular bone parameters,as mineral density in the distal femur metaphyseal region as well as in the lumbar vertebrae and increased osteoblast serum markers in male mice,although no effect on bone parameters in females was found[72].Furthermore,Schepperet al[73]investigated the effect of antibiotic treatment on gut and bone health in mice models.They found an increase in the Firmicutes/Bacteroidetes ratio,in the intestinal permeability,and a reduction of femoral trabecular bone volume.Treating the mice withL.reuterireduced the post-antibiotic elevation of the Firmicutes/Bacteroidetes ratio and prevented bone loss.Antibiotic-induced dysbiosis was associated with decreased osteoblast and increased osteoclast activities[73].
Recently,Naseret al[74]showed that the inflammation associated toMycobacterium avium subspecies paratuberculosis(MAP) infection results in elevation of undercarboxylated osteocalcin (ucOC) and downregulation of active osteocalcin (OC) in CD patients.This suggest that MAP infection may serve as a trigger factor in the development of OP in CD patients.
Nutrition and vitamin deficiency:Nutritional alterations and vitamins or minerals deficiency due to inadequate diet intake and/or malabsorption correlate with a low BMD and may contribute to the development of osteopenia and OP both in UC and CD patients.Limet al[75]assessed the nutritional status of 41 IBD patients with or without malnutrition and showed significantly higher serum C-reactive protein (CRP)and lower serum calcium in the malnourished group.No significant differences between malnourished and normal group were found as to BMD although lower bone density was more frequent in malnourished group.Also,Azzopardiet al[47]found a significant correlation between body mass index (BMI) and BMD of IBD patients[76].
Many studies measured calcium daily intake in IBD patients.Silvennoinenet al[77]assessed calcium intake and measured BMD in IBD patients and controls.They found that,although the daily intake of calcium was lower in IBD subjects than in controls,especially in male patients,there was no significant correlations between calcium deficiency and BMD[77].Verniaet al[78]analyzed by means of a questionnaire the dietary calcium intake in 187 IBD patients.They confirmed that calcium intake is frequently lower in IBD patients; moreover,most of the patients adopted some arbitrary dietary restrictions (i.e.,avoidance of milk or dairy products) which increased the risk of OP[78].Calcium supplements as well as vitamin D administration showed an improvement of BMD at lumbar spine in osteoporotic patients with IBD.On the contrary,fluoride supplementation does not seem to provide any benefit to IBD patients[79].
Vitamin D has systemic functions; it acts on regulation of the innate and adaptive immune responses and modulates calcium homeostasis involved in bone metabolism.In IBD patients a vitamin D deficiency negatively affects the immune system inducing dysregulation and inflammation-associated loss of BMD[80].Vitamin D deficiency is more frequent in IBD patients than in the general population[81].Del Pintoet al[82],in a meta-analysis involving 14 studies,with 938 IBD patients and 953 controls,showed that 64% of IBD patients had lower vitamin D serum levels than controls.Interestingly,UC appeared to be associated with more than double the odds of vitamin D deficiency compared to healthy controls.A recent study,aimed at evaluating the absorption of orally administered vitamin D in CD patients compared with healthy controls,showed a great variability in the bioavailability of vitamin D(2) in CD patients although no significant differences between patients with different location of disease or among those with or without previous surgery were found.Moreover,24 h after an oral load of vitamin D(2),the authors reported that the ability of absorption in CD patients was on average 30% lower than in normal subjects (P< 0.001)[83].Based on most of the studies,it seems reasonable that measurement of serum vitamin D levels should be included in the follow up of IBD patients both adults and children.In fact,in pediatric IBD patients a vitamin D deficiency may enhance the odds of developing osteopenia or OP[84].
IBD patients might also have a reduced absorption of vitamin K,especially CD patients with an involvement of distal ileum.Besides playing a major role in coagulation processes vitamin K prevents bone resorption,inhibiting the production of prostaglandin E2 by osteoclasts,so its deficiency may affect BMD,as reported in both adults and pediatric patients[80].However,the role of vitamin K in bone metabolism is controversial and the routine supplementation is not widely accepted yet[85].
Glucocorticoid therapy: A major risk factor associated to bone metabolism alterations in IBD patients is GC therapy,which in several occasions is administered without additional vitamin D or calcium supplementation[4].GCs are still largely used in IBD patients with moderate or severe disease[85].GC therapy causes a biphasic bone loss,firstly with a rapid decrease of BMD of about 6% to 12% in the first year,and after,with an annual loss of about 3% for as long as the therapy is administered[87]associated with an increase of the fracture risk in the first 3 mo,which can reach a percentage as high as 75%.The fracture risk then decreases in the first 3 mo after GC withdrawal,before any significant improvement in BMD values[88].GCs cause a reduction in the cortical thickness and an increased cortical porosity in mice models,associated with increased osteoclast number at the endocortical surface.Osteoclast formation in trabecular bone depends on the production of RANKL by osteocytes as well as by the increase in cortical bone resorption induced by mechanical unloading or by dietary calcium deficiency.In vitromodels showed that GC therapy directly increases the production of RANKL and reduces OPG expression levels in stromal cells and osteoblasts[89].Also,Hofbaueret al[90]reported that RANKL inhibition prevented GC-induced bone loss.
Piemonteseet al[91]examined the effects of prednisolone on cortical bone in mice lacking RANKL production in osteocytes.Prednisolone increased osteoclast number at the endocortical surface,increased cortical porosity,and reduced cortical thickness in control mice,but none of these effects were found in mice lacking RANKL in osteocytes.Moreover,in cortical bone organ cultures and primary osteoblasts,dexamethasone suppressed OPG without any variation of RANKL levels.Therefore,based on these observations,OPG,rather than RANKL,seems to play a major role in the endocortical resorption.
OPG-mediated bone loss prevention acts through the inhibition of RANK-RANKL pathway and reduction of osteocytes apoptosis,induced by GCs.Weinsteinet al[41],bothin vivoandin vitro,studied the effect of OPG administration,with or without the fragment crystallizable region of Ig heavy chains (OPG-Fc),on the bone loss and on the apoptosis of osteocytes,with or without GCs administration.They showed that in mice treated with prednisolone combined with OPG-Fc or only with OPG-Fc there was a decreased expression of both receptors of cathepsin K and OC,which are markers of osteoclast number.Moreover,OPG-Fc administration preserved the BMD at spine compared with animals who received only prednisolone.The authors also reported an increase of vertebral strength of about 29% in mice receiving OPG-Fc compared to those receiving OPG-Fc combined with prednisone.Finally,OPG-Fc administration,alone or combined with prednisolone,decreased the number of osteoclasts of about 7% and 5% respectively,compared with placebo group.Prednisolone also induced an increase of the osteocytes apoptosis of about 335%,which was prevented by OPG-Fc administration.This supports the concept that OPG administration may prevent the reduction of BMD,of vertebral cortical thickness,and of osteocytes viability induced by GCs[41].
In conclusion,GC therapy is a major determinant of bone mass alteration in IBD patients.New generation GCs,such as budesonide or beclometasone,which show a very efficient hepatic first pass metabolism may represent a valid alternative to conventional GCs in order to try to minimize GC detrimental effect in general and on bone structure in particular[92,93].
DISEASE SEVERITY/ACTIVITY AND BONE MINERAL DENSITY
Calcium is an essential ion for bone formation and its only source is diet.The absorption of dietary calcium is a vitamin D-dependent process[94].In the distal part of the intestine,70%-80% of the ingested calcium is absorbed (mostly in the ileum)[95]through the action of Vitamin D receptor which is expressed in all segments of the small and large intestine with the highest levels reported in the cecum and colon.In patients with extensive intestinal resection,calcium absorption has been reported to be significantly higher when the colon is preserved[96].In IBD,different segments of the intestine may be involved by the inflammatory process and the subsequent alterations of the absorptive processes have been suggested to be an important determinant of bone loss[97,98].Several studies evaluated the correlation between disease extension or activity according to the Montreal classification for IBD[99]and BMD.In 1997,Bjarnasonet al[29]reported that there were no significant differences in T scores for spine or hip within the patient subgroups according to disease location.Also,Jahnsenet al[30]assessed BMD in 60 patients with CD in 60 patients with UC and in 60 healthy subjects.Patients with CD had similar BMD,independently on whether the colon or the small intestine was involved.Furthermore,no differences were described between patients with CD with or without small bowel resection.In addition,no correlations between the length of small bowel resected and BMD were found.Finally,in the UC patients there was no influence of disease location and extension on MBD.More recently,the same results have been described by Vázquezet al[34]on 107 patients with IBDs (53 with CD and 54 with UC) with different location of the disease.The extension and the location of the disease did not seem to influence BMD loss or vertebral fractures prevalence.In a study conducted in 99 consecutive CD outpatients,Cravoet al[100]assessed disease activity by Harvey-Bradshaw Index(HBI).With a multivariate analysis,they described a direct and significant association between age (above 40 years),chronic active disease (HBI 4),previous colonic surgeries and the presence of OP.Both small bowel and colonic resection were similarly associated to OP.This might be explained by the major impact of inflammation due to disease severity in respect to the reduction of mineral absorption induced by short bowel syndrome,as initially hypothesized.Moreover,to support the role of chronic inflammation in the pathogenesis of bone loss,patients with active disease(HBI > 4) and those with a penetrating or structuring disease,which are usually more aggressive phenotypes,were also those with the highest rate of OP.
More recently,Limaet al[101]evaluated the correlation between disease severity and BMD in 68 patients with UC and 60 with CD of 17-40 years of age.About half CD patients had an ileocolonic disease (53.3%) while 29 subjects (48.3%) had nonstricturing non-penetrating disease and 33.3% had perianal disease,according to Montreal classification.In the UC group,29 patients (44.6%) had extensive UC according to the Montreal classification[99].The authors described a higher incidence of osteopenia in UC and CD patients than controls (OR = 14.93/OR = 24.38,respectively).At multivariate analysis in CD group,low BMD was associated with sex (M >F),perianal disease,penetrating behavior and age at diagnosis > 40 years,while,no association was described between BMD and disease activity.In the UC group,low BMD was significantly associated to sex (M > F) and left colitis.Therefore,disease activity does not seem to be a major determinant of bone density alteration in CD and UC patients,while disease severity seems to be associated with osteopenia in IBD patients.It must be emphasized that only 0.02% of UC patients and 0.26% of CD patients had active disease at the time DEXA was performed,and,therefore,the remission of the disease might have been be associated with an increase in BMD.
TNF-/ANTI-TNF- THERAPY AND BONE DENSITY ALTERATIONS
IBD is an immune-mediated inflammatory condition characterized by activation of different inflammatory pathways and abnormal secretion of different cytokines such as TNF-α[102].
Anti-TNF-α is the first available biologic therapy for IBD and,currently,its effects on BMD are not known.Moreover,it is not clear whether the effects of anti-TNFα agents on bone health are the consequence of a direct interference with the process of bone modeling or if these effects are simply due to a decreased disease activity and subsequent improvement of mineral absorption.
As previously mentioned,two members of TNF superfamily,RANKL OPG,are the key regulators of bone remodeling.RANKL,derived by osteoblasts,stimulates formation of mature osteoclasts while OPG,produced by osteoblasts,is a competitor that inhibits the interaction between RANKL and its receptor[103].TNF-α is a main actor of osteoclastogenesis by inducing activation of NF-κ B transcription and,also,reducing bone formation through the inhibition of osteoblast differentiation[104].Moreover,it increases the survival of osteoclasts by protecting them against apoptosis[105]while it induces apoptosis of osteoblasts to reduce bone formation[106].Therefore,TNF-α not only plays a central role in the pathogenesis of IBD but is also involved in bone metabolism,promoting bone resorption through regulation of osteoclast activity (Figure 1).As described by Azumaet al[107],TNF-α directly induces the differentiation of osteoclast progenitors into mature osteoclast playing an important role in local osteolysis in chronic inflammatory diseases.Based on this,many studies have evaluated the effect of infliximab,a chimeric (i.e.,half human and half murine) anti-TNF agent,on bone metabolism investigating serum bone marker,BMD or incidence of bone fractures.Only one study assessed the impact of adalimumab,another all human anti-TNF agent,on bone metabolism.In a Belgian study[108],authors evaluated markers of bone formation and resorption at eight weeks from the beginning of infliximab therapy in comparison with healthy controls.In their cohort,regardless of patients’ clinical response,anti-TNF-α increased bone formation and,in the majority of patients,strongly decreased bone resorption.In a one year follow up study[109],after starting therapy,the mean BMD resulted to be increased significantly in CD patients without any correlation with concurrent corticosteroid therapy.So,the authors suggested that amongst the factors inducing bone loss in CD,the inflammatory disease process might be predominant over the effects of treatment with prednisone.This might be especially relevant in CD patients who need to continue steroid therapy despite concurrent immunomodulatory therapy.
In 24 patients with active CD treated with infliximab,Ryanet al[110]described a significant increase of bone alkaline phosphatase,a marker of bone formation,and OC,a bone specific calcium-binding protein produced by osteoblasts,which persisted up to 4 wk after the end of treatment.As underlined by other authors,the benefits occurred independently of the clinical response of CD to biological treatment.On the other side,Mihelleret al[111]dosed serum OC and CrossLaps (bCL),a degradation product of collagen,in 27 patients with fistulizing CD treated with anti-TNF-α.In the group of patients who responded to therapy,but not in those who did not,serum bCL concentrations were significantly decreased from week 0 to week 6,while a statistically significant increase was described for OC,thus suggesting that the beneficial effect of anti-TNF therapy was related to the amelioration of the underlying inflammatory process.
More recently,a 7-year follow-up longitudinal prospective cohort study by Maldonado-Pérezet al[112]evaluated the role of anti-TNF-α in decreasing fracture risk or modifying BMD in IBD patients.The authors described no difference in the incidence of vertebral fracture and value of bone mass between the group of patients treated with anti-TNF-α and the control group which did not receive biological treatment.Despite the biological-treated patients had received GC therapy for a longer period of time compared to the control group,new fractures were more common and more severe in the control,nonbiological-treated group.After 7 years of follow-up,bone mass increased significantly in the spine and in the femoral neck in patients treated with anti-TNF-α,compared to subjects who did not receive biological therapy.
Only one study[113]evaluated the impact of adalimumab therapy on bone metabolism.Parathyroid hormone,vitamin D,bone formation and resorption marker,pro- and anti-inflammatory OPG,and sRANKL were measured in healthy controls and in CD patients pre- and post-treatment with adalimumab.Moreover,viability and differentiation of human osteoblasts (hFOB 1.19) cells after exposure to sera from CD patients pre- and post-adalimumab treatment was also analyzed.Following adalimumab therapy,a rapid increase in bone formation markers (OC and procollagen type 1 N-terminal pro-peptide) and a not significant decrease of a bone resorption marker (C-telopeptide of type-1 collagen) were observed.In thein vitrostudy,osteoblasts exposed to sera of CD patients before adalimumab therapy showed consistently higher levels of viability and lower levels of ALP compared to control group suggesting a greater viability of osteoblasts associated to a lower osteoblast function likely due to an inflammatory-driven response.After treatment,serum of CD patients induced higher levels of ALP in hFOB cells probably due to an improvement of their functionality.
In conclusion,anti-TNF seems to improve BMD in IBD patients both through a direct beneficial effect on bone metabolism and through the improvement in the underlying intestinal inflammatory process.Whether other biologic agents now available for the treatment of IBD,such as vedolizumab or ustekinumab,have any effect on bone metabolism needs to be determined.
DIAGNOSIS OF OSTEOPOROSIS
Diagnosis of OP should be based on patient clinical history,physical examination,BMD measurements,and laboratory investigations[17].In particular,because changes in bone metabolism are frequently associated with the evolution of IBD and may have a negative impact on the patient’s quality of life,assessment of BMD in all IBD patients is essential to prevent and treat appropriately MBDs.The gold standard for its assessment is DXA.Changes in BMD values are key determinants to evaluate treatment efficacy at follow-up.Moreover,FRAX algorithm by combining all the fracture risks with the hip BMD value can quantify the 10-year risk of experiencing a fragility fracture[114].Laboratory tests are necessary not only to exclude secondary forms of OP but also for the bone metabolism assessment.They should include biochemical markers of bone turnover and vitamin D status that might provide additional information regarding the patient fracture risk.
Moreover,increase in the incidence of BMD loss supports the recommendation to screen patients with IBD at an early stage of the disease.Screening recommendation of European Crohn and Colitis Organization (ECCO)[115]does not differ from those for the general population.It considers risk factors such as postmenopausal state,ongoing corticosteroid treatment,cumulative corticosteroid use > 3 mo,history of low-trauma fracture and age.Moreover,annual DXA scans is recommended in patients receiving long-term steroid therapy (in particular when there are others risk factors) if the T-score approaches the threshold for treatment with bisphosphonates(BPs) (T-score < -1.5 SD)[116].
THE PHARMACOLOGICAL MANAGEMENT OF OP
The aim of the management of OP is to reduce the risk of fragility fractures in individuals at high-risk.Therefore,pharmacological intervention thresholds should be based on the assessment of this risk deriving from the integration of densitometric data with other important clinical factors as determined by the FRAX[116].Approved pharmacological treatments for the management of OP can be classified into two categories:anti-resorption (or anti-catabolic) and anabolic drugs.Among anticatabolic drugs,biphosphonates (BPs) blocking the osteoclastic activity,manage to reduce the bone remodeling process with a consequent increase in bone density.Alendronate and risedronate are the most commonly used for the prevention of vertebral and non-vertebral fractures (including hip) based on strong scientific evidence of efficacy[117].However,they have reduced compliance and persistence to prolonged therapy,due to daily or weekly administration regimens and possible gastro-intestinal adverse events.Zoledronic acid is a BP intravenously administered with documented efficacy in reducing the risk of vertebral,non-vertebral and hip fractures[117].A meta-analysis of studies on BPs use in IBD patients showed that these drugs are effective in case of low BMD reducing the risk of vertebral but not of nonvertebral fracture[118]; so,the use of BPs should be recommended for fracture prevention in IBD patients taking always into account the possible adverse effects of treatment.
A powerful inhibitor of bone resorption is denosumab,a human monoclonal antibody capable of neutralizing RANKL,a cytokine that interacts with the RANK receptor on the membrane of preosteoclasts and mature osteoclasts,affecting their recruitment,maturation and survival.A dose of 60 mg subcutaneously every 6 months is sufficient to strongly inhibit osteoclastic activity and to reduce the risk of vertebral and non-vertebral fractures (including hip).Unlike BPs,discontinuation of denosumab is followed by a sharp increase in bone turnover and a rapid loss of BMD.Therefore,discontinuation of denosumab generally requires the patient to initiate BPs treatment at an appropriate dosage as soon as possible[119].
Among anabolic drugs,teriparatide,the active fragment of PTH (1-34 PTH) is the most widely used.It can stimulate both bone formation and resorption,with a predominant effect on the neoformation (anabolic window) which is evident above all during the first 12 mo of treatment.It is generally used as a second line antiosteoporotic drug in case of intolerance or resistance to other anti-resorption agents and as first choice in case of severe OP in patients with multiple fragility fractures[17].
All clinical guidelines agree that the pharmacological therapy of OP,independently of the prescribed treatment,should always be supplemented by the administration of vitamin D and,in case of nutritional deficient intake,of calcium[120].
ECCO guidelines[115]suggest,some recommendations concerning the management of bone alterations in IBD population (Table 1).
CONCLUSION
The prevalence of OP and/or fragility fractures in IBD patients is controversial because of different factors,such as different study population and study design,and location of the disease.Moreover,some aspects still need to be clarified,particularly the correlation between the increased risk of fragility fractures in subjects affected by IBD.
Changes in bone metabolism are frequently associated with the evolution of IBD and may have a negative impact on the patient’s quality of life.
In this context,even understanding the pathophysiological milieu seems to be quite challenging.For example,the genetic background predisposing to the development of osteopenia and OP,specific for IBD patients,since the strongly multifactorial nature of these diseases,does not allow to evaluate its pathogenic role without considering other factors,such as nutrition,lifestyle,or more simply,pharmacological therapy for IBD.On the other side,increasing evidence suggests a gut-bone signaling pathway,which is responsible for a close cross-talk between the musculoskeletal and the GI system,and whose alteration may potentially correlate with the evolution of this type of EIMs.Furthermore,because of the emerging role of intestinal microbiota in the pathogenesis of IBDs,a direct impact of dysbiotic commensal microflora on bone metabolism,as shown in the healthy population,seems to be possible.A schematic diagram summarizing the pathophysiologic mechanism,including molecular mechanisms,underlying BMD alteration in IBD patients is shown in Figure 3.
The nutritional aspects,always considered among the main factors capable of triggering bone alterations,appear once again crucial,especially regarding the intake of calcium and vitamin D,the lack of which,both in adults and children,shows a direct correlation with the increased probability of developing bone fragility,specifically linked to osteoporomalacic findings.For this reason,it is important to include the evaluation of serum vitamin D levels and of nutritional status in IBD patients,both in active phase and remission of disease,in order to avoid the establishment of malnutrition that may increase the onset of comorbidity.
Pharmacotherapy of IBD might play a major role in bone metabolism.GCs are the main determinants of bone alterations and their prolonged use is associated with OP,osteopenia and increased risk of fractures.Therefore,their use should be limited and,whenever possible,new generation corticosteroids with a safer profile should be used.Finally,anti-TNF agents seem to improve bone health in IBD patients both by directly interfering with the metabolic pathways involved in bone modeling and by decreasing the disease activity and severity.Whether new biologic agents exert any beneficial effect on bone tissue in IBD patients remains to be determined.
Finally,and more important,a thorough evaluation of bone metabolism including serological markers should be part of the follow-up of IBD patients in order to prevent and/or promptly treat any bone alteration which may alter their quality of life and increase the risk of fractures.

Table 1 European Crohn and Colitis Organization guidelines for the management of bone alterations in inflammatory bowel diseases population
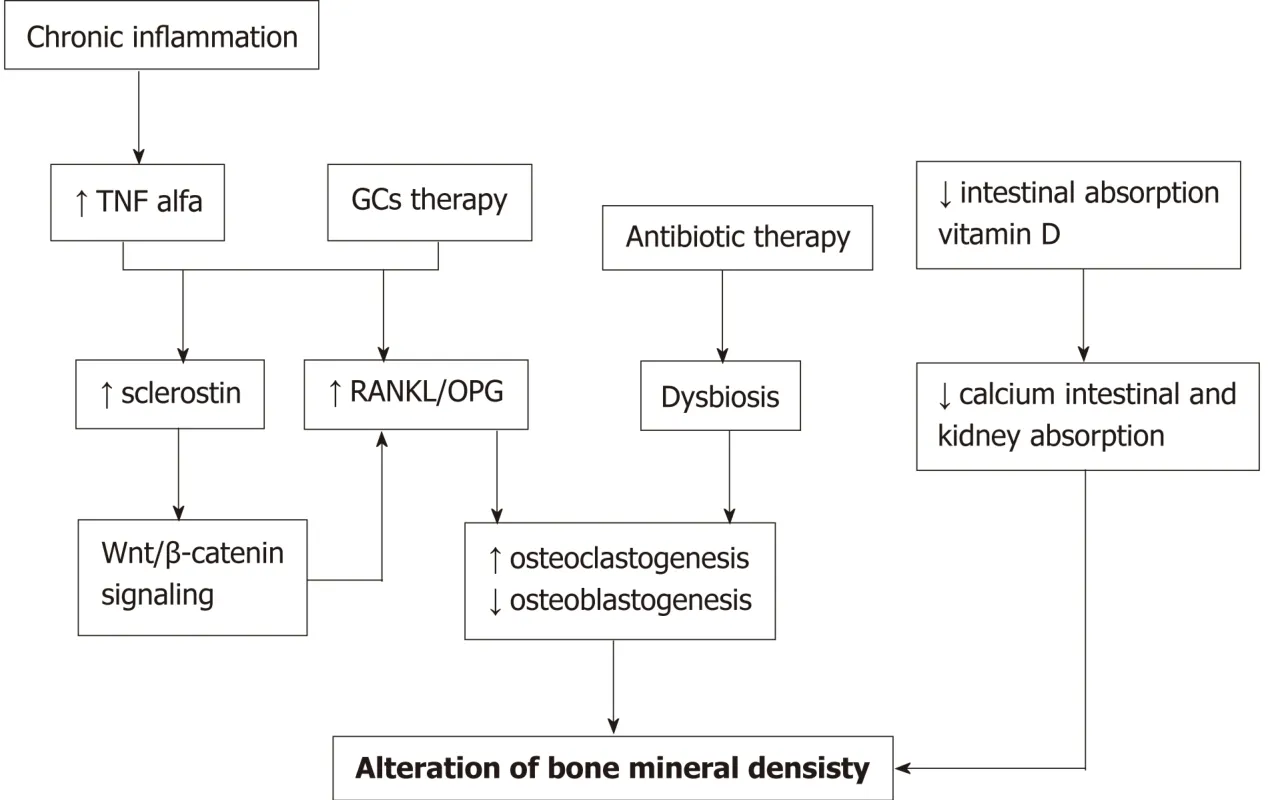
Figure 3 Diagramatic representation of the pathogenic mechanisms involved in alteration of bone mineral density in inflammatory bowel diseases.
杂志排行

World Journal of Clinical Cases的其它文章
- Extrahepatic hepcidin production: The intriguing outcomes of recent years
- Neoadjuvant endocrine therapy: A potential strategy for ER-positive breast cancer
- Vestigial like family member 3 is a novel prognostic biomarker for gastric cancer
- HER2 heterogeneity is a poor prognosticator for HER2-positive gastric cancer
- Changes in corneal endothelial cell density in patients with primary open-angle glaucoma
- Myocardial bridge-related coronary heart disease: lndependent influencing factors and their predicting value