Effect of restoration technique on resistance to fracture of endodontically treated anterior teeth with f l ared root canals
2019-05-17SarySBorzangySamahSakerWalidAlZordk
Sary SBorzangy,Samah M Saker,Walid A Al-Zordk
1 Department of Substitutive Dental Sciences,College of Dentistry,Taibah University,Medina 42353,Saudi Arabia;
2 Department of Fixed Prosthodontics,Faculty of Dentistry,Mansoura University,Mansoura 35516,Egypt.
Abstract Thisstudy wasdesigned to comparetheimpactof postand coresystemson resistanceto fractureof endodontically treated anterior teeth with f l ared root canals and to assess their fracture pattern.Sixty central incisors were cut horizontally 2 mm coronal to thecementoenamel junction(CEJ).After root canal therapy,teeth wereassigned into 6 groups(n=10 each)based on apostsystemand used asfollows:Group C,non-f l ared rootreceived size#1 glass f i ber posts(Control);Group AP,f l ared rootrestored with anatomical post;Group RC,f l ared root restored with size#1 f i ber post and cemented with thick layer of resin cement;Group CR,f l ared root restored with size#1 and reinforced with composite resin;Group CM,cast post-core;Group CP,CAD/CAM polymer-in f i ltrated ceramic post and core.Following post cementation,core build-up and crown insertion,the specimens were thermo-cycled up to 10,000 cycles(5C/55C;30 seconds dwell time,6 seconds transition time)and then statically loaded at 1 mm/minute crosshead speed using auniversal testing machine.One-way ANOVA and Tukey HSD post hoc test(α=0.05)were used for dataanalysis.Group Crecorded signi f i cantly higher resistanceto fracturevalues[(826.9±39.1)N]followed by group CP[(793.8±55.6)N]whilegroup RCyielded the lowest fracture resistance values[(586.7±51.4)N].The resistance to fracture of wide root canals can be enhanced by using one-piece CAM/CAM post and core as an alternative to the use of either glass f i ber post,relined with composite resin increasing thethickness of luting cement or the use of cast post and core system.However,this was an in vitro investigation and further in vivo studies are necessary.
Keywords:anatomical post,customized post,endodontically treated teeth,f l ared root canal
Introduction
Long-term clinical performance of root-canal treated teeth depend primarily on the amount of the tooth’s remaining structure.Teeth with extensive tooth loss have reduced capacity to resist forces during function and a post is essential to hold an arti f i cial core that will restore the tooth loss[1-5].For many years,many dental practitioners believed that a post would“reinforce”the tooth structure[6-7],however,the volume of dentin remaining is of most relevance to tooth strength[8-11].During post space preparation procedure,it is recommended that the remaining dentin should be preserved asmuch aspossible.Resistanceto fractureof rootcanalf i lled teeth depends primarily on the remaining root dentin thickness,especially in the bucco-lingual direction[12].The cervical portion of the root canal may be left widely prepared and surrounded only by a thin dentinal wall.And asaresultof over-preparation of root canal,removal of extensive caries,and recurrent caries around the post into the root canal dentin thus,reduce the fracture resistance[2,9,13-14].Vertical root fracture of endodontically treated teeth,with wide root canals,represents a critical clinical dilemma[15],although the use of f i ber posts(FP)has improved the long-term clinical success[8].
Many studies have been conducted in order to develop a reliable technique of reinforcing endodontically treated teeth with wideroot canals[16-19].Grandini et al.[20]described a technique for reconstruction of compromised endodontically treated tooth by using an“anatomical post”,where a composite resin was used for FP relining so the shape of the post-core matched those of a f l ared post space.This technique is undoubtedly effective to minimize the volume of luting cement,and reduce its polymerization shrinkage[21-29].
In addition,various materials have been recommended in order to f i ll f l ared root canal with a biocompatible material with similar physical properties to those of dentin to increase the resistance fracture of weakened rootslikecompositeresinsand glassionomer cements[19,27,29].The post system chosen to retain a restoration must present biomechanical properties similar to dentin and provide adequate retention and stiffness to prevent any micro-movement between an arti f i cial crown and aroot face.Glass f i ber post systems were introduced with advantages in respect to their biomechanical propertiesand to transmit lightsimilar to that of tooth structure[6-9].
Recently,Chen et al.[30],studied anovel techniqueto fabricate a custom glass f i ber post-and-core with CAD/CAM system for restoration of compromised endodontically treated root canal in vivo and they reported the effectivenessof thistechniqueto beused for restoration of f l ared root canal-treated teeth.
Therefore,this investigation was conducted to evaluate fracture resistance of anterior teeth with f l ared root canalsrestored with glass f i ber posts,cast post and core and CAD/CAM post and core fabricated from VITA Enamic.The null hypothesis tested was there would beno signi f i cant difference in fracture resistance between the four different materials used.Fracture pattern were also evaluated for each test group.
Materials and methods
Specimens preparation
Sixty extracted intact human maxillary central incisors of similar-sized,devoid of caries or cracks,with straight root canal were used in this study.The teeth were debrided,cleaned with ultrasonic scaler and brush and residual tissue tags were scraped from the roots.After cleaning,the teeth were stored in a 0.1%thymol solution at 4°C up to 3 months following extraction beforeuse.Coronal portionsof theteeth were transversely cut 2 mm incisal to the cementoenamel junction(CEJ)with alow-speed,water-cooled diamond disk followed by f l attening of the sectioned surfaces with silicon carbide paper(600 grit).
Root canal obturation
After pulpal tissue removal,a step-back technique was used for root canal preparation using f i nal f i le size number 50(Dentsply Maillefer,Ballaigues,Switzerland)at the working length that was set at 1 mm away from the apical foramen.A 5.25%NaOCIirrigant was used after each f i le and up to the f i nal size,followed by rinsing with distilled water.The prepared root canals were obturated with gutta-percha cones(Dentsply Maillefer,Ballaigues,Switzerland)after completely drying with paper points using a lateral condensation technique and AH-Plussealer(Dentsply IH Ltd,United Kingdom).After obturation,the coronal opening of the root canal was closed with a temporary restorative material(Cavit-G,3M ESPE,Minnesota,United States)and the teeth were stored for 7 days at 37°C and at 100%humidity.
Study groups
To simulate the periodontal ligaments effect,a thin coat of polyvinylsiloxane impression material was painted on the root surface.With the aid of a centralization device,the specimens were embedded vertically in an epoxy resin(Kemapoxy,CMB chemicals,Giza,Egypt)at adepth of 2 mm apical the CEJ.To standardize the post space preparation,the endodontically treated canal were initially prepared to receive a size#1 post(RelyXTM,3M ESPE,St.Paul,Minnesota,United State)of 1.3 mm diameter using matching stainless steel low-speed reamers and the depth was limited to 10 mm using a rubber stopper as a reference(Fig.1).The preparation drill was changed after f i ve preparations so each group used two drills.The specimens were assigned into 6 groups(n=10).Group C:control,non-f l ared roots;groups AP,RC,CR,CM and CP:f l ared rootsin which therootswerefurther prepared to simulate roots with f l ared post space using 2.5 mm diamond burs(#413,KG Sorensen,São Paulo,SP,Brazil)in a low speed hand piece limited to 10 mm vertical length to achieve approximately 1 mm wide coronal root dentinal wall(Fig.1).
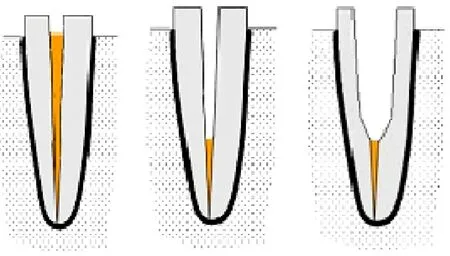
Fig.1 Schematic diagram showing the steps of root canal obturation,gutta-percha removal and f l aring of the post space.
Restoration of the prepared post space
Beforepostinsertion,thepostswereairborne-particle abraded with 50-µm aluminaparticles(Heraeus Kulzer)using a custom-made revolving wheel at 250 kPa pressure for 5 seconds.
Group C(Control,n=10):the specimens of this group were restored with size#1 f i ber posts(RelyXTM,3M ESPE,St.Paul,Minnesota,United State).
Group AP(n=10):f l ared post spaces were restored using size#1 f i ber posts,relined with composite resin.The f i ber post wascoated with alayer of silanecoupling agent(Prosil,FGM)for 1 minute,and it was gently air dried for 5 seconds and coated with two-step etch-andrinse bonding agent(Tetric N-Bond,Ivoclar Vivadent),followed by solvent evaporation and f i nally light cured for 10 seconds.The f i ber posts were covered with composite resin(Tetric N-Ceram,Ivoclar Vivadent)then inserted into the canal that previously lubricated with a water-soluble gel(KY,Johnson&Johnson).A customized centralization device was used to aid in guiding and positioning of thelined postin thecenter of the prepared post space with an even thickness of the composite resin around the post.To insure accurate f i tness,the relined f i ber post wasremoved and replaced twice.After removal of the excess resin composite material,therelined f i ber post waslightcured for 20 sec with the post inside the post space followed by additionally curing for 20 seconds from the buccal,lingual,mesial,and distal surfaces outside the post space.The root canals and the relined f i ber posts were then rinsed abundantly with water to remove the lubricant gel(Fig.2).
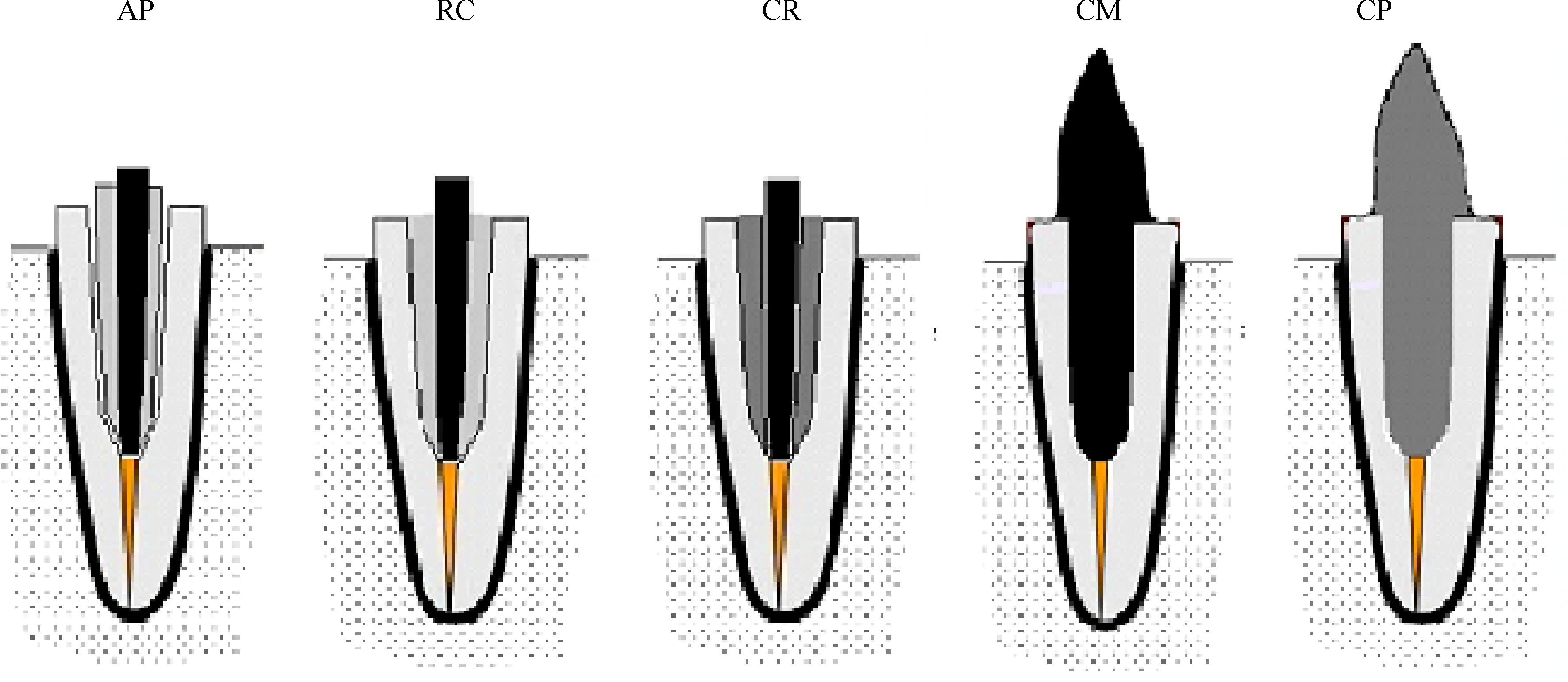
Fig.2 Schematic illustration of the f l ared roots restored with:anatomical post(AP);size#1 f i ber post cemented with thick layer of resin cement(RC);size#1 f i ber post reinforced with composite resin(CR);cast post and core(CM);CAD/CAM polymer-in f i ltrated ceramic post and core.
Group RC(n=10):f l ared post spaces were restored using size#1 f i ber posts cemented with self-adhesive dual-polymerizing resin luting material RelyX Unicem(3M ESPE,See f l ed,Germany).Thecementcapsulewas activated and mixed for 15 seconds according to manufacturer’s instructions.The mixed cement was injected into the prepared post space through the elongation tip of the capsule to ensure void-free cementation of the posts(Fig.2).The centralization device was used for positioning of the post within the center of the post space.After removal of excess cement,f i nal light-polymerization was done for 20 seconds on each surface as mentioned previously.
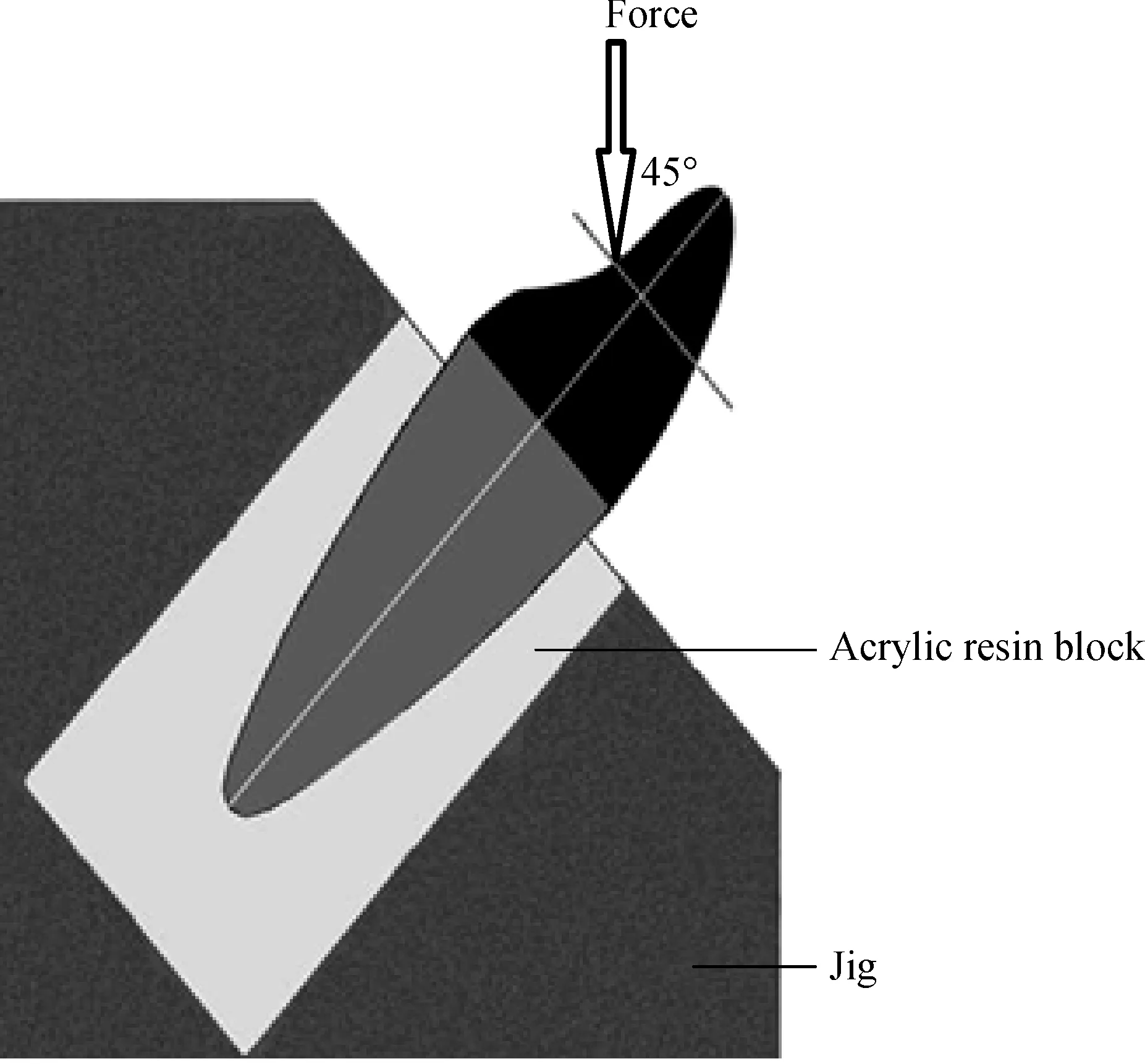
Fig.3 Schematic illustration of the fracture resistance test showing the load applied at 135-degree from the long axis of the root and 3 mm away from the incisal edge.
Group CR:reinforcement of f l ared root canal with compositeresin.Thedentin wallsof thepostspacewere etched for 15 seconds with 37%phosphoric acid gel(Total Etch,Ivoclar Vivadent;Schaan,Liechtenstein)then rinsed and dried with paper points.The two-step etch-and-rinse bonding material was applied on the entire canal surface in two coats with the aid of a microbrush,as recommended by the manufacturer.After solvent evaporation,the adhesive was light cured for 10 seconds by positioning the tip of the light-curing unit at the entrance of the root canal.A f l owable composite resin(Tetric N-Flow,Ivoclar Vivadent)was used to f i ll in the post space from the apex to thecervical portion to avoid theformation of air voids.After this,the glass-f i ber post#1 was lubricated with the water-soluble gel(KY,Johnson&Johnson)and inserted into the canal by using a centralization device.The f l owable composite resin was light cured for 20 seconds after the removal of the f i ber post,the root canals were rinsed abundantly with water to remove the lubricant gel.The f i ber posts were rinsed and cleaned.Afterwards,the post spaces were slightly re-prepared with size#0 drill corresponding to the#0.5 post.
Group CM:the canals were lubricated and the autopolymerizing resin(DuraLay II,Reliance Dental Mfg Co)was added over the plastic dowel using beadbrush technique.The pattern was removed inspected after 3 minutes according to instructions of the manufacturer.After re f i tting the post,the core portion wasformed by addition of more pattern resin.The f i nal shaping of the core was done with f i nishing burs.The patterns were invested and casted with Ni-Cr alloy(Kera NH;Eisenbacher Dentalwaren).
Group CP:the patterns of posts and cores were fabricated asdescribed in group CM.The patternswere sprayed with anti-re f l ection scan powder spray(Digiscan-Spray,Yeti).Each post-core was mounted over the scanning tray of the extraoral scanner(Ceramill map400,Amann Girrbach).The scanning process was performed automatically by moving the shifting plate with thepattern f i xed on it and gaining multiplecamera screening.The construction data to design the restorations was performed through standard transformation language(STL)data format.The job de f i nition on the CAD/CAM software(Ceramill Mind software,Amann Girrbach)was started by selection of inlay/onlay as restoration type.After the software calculated the proposed design of post and core,some modi f i cations were made manually.The STL f i le was sent to the milling unit(Ceramill Motion 2 5X,Amann Girrbach)to mill the post and core from VITA Enamic block.After f i nishing,the post surfaces were conditioned for 60 secondswithhydro f l uoric acid(IPSCeramic Etching gel,Ivoclar Vivadent)and subsequent silainization(vitigue silane primer,DMG Hamburg,Germany)was done(Fig.2).
Self-adhesive resin cement was used for posts cementation following the instructions of the manufacturer.The composite resin cores(Filtek Z250;3M ESPE)were fabricated in a standard manner for all groups except groups CM and CP using core-forming matrices(Ultra-form;Ultradent Products Inc).All specimens were prepared to receive complete cast crownspreparation with 0.5 mm width using adiamond bur at high speed with water spray.
Crown fabrication and cementation
Wax pattern of each crown was made directly on the specimen with a polyvinyl siloxane putty index(Lab Putty;Coltène/Whaledent),to simulate the anatomy of central incisor with an 11 mm length,and a lingual notch 3mmapical to theincisal edge.To standardizethe dimensions,each wax pattern wasmeasured with awax caliper.The wax patterns were invested and cast in Ni-Cr alloy following the manufacturer’s instructions.The inner surfaces cast crowns were airborne-particle abraded at 0.25 MPa pressure with 150 mm alumina particles(Al2O3;Heraeus Kulzer)and ultrasonically cleaned in 96% isopropanol.The prepared tooth surfaces were cleaned with pumice,rinsed,and dried before f i nal cementation with resin cement following the manufacturer’s recommendations.The specimens were thermocycled up to 10,000 cycles(5C/55C;30 seconds dwell time,6 seconds transition time).
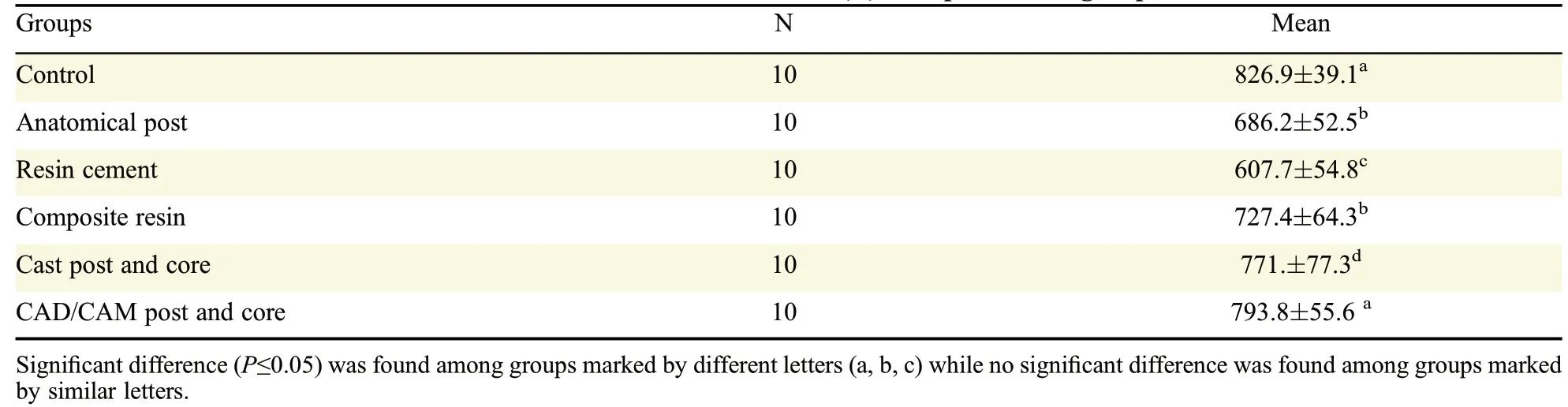
Table 1 Mean and standard deviations of fracture resistance values(N)of experimental groups
Fracture strength test
A standard testing machine(Lloyd Instrument,LTD,West Fareham,UK)was used at a crosshead speed of 1.0 mm/minute with a 5 kN load cell to apply a unidirectional static load at an angle of 135 degrees from the long axis of the root(Fig.3),applied to a groove located at the palatal concavity of the crown located 3.0 mm away from the incisal edge of the restoration.The load was applied until fracture.The force at which initial root fracture occurred was recorded in Newtons(N).Specimens were visually inspected to determine the location,type,and direction of failure.The failure mode was recorded and classi f i ed as either“repairable or favorable”(detachment of the postand coreand/or fractureof cervical third of theroot that could be repaired through fabrication of a new restoration)or“irreparable or catastrophic”(vertical or horizontal fracture and oblique fracture below the cervical third of root that would necessitate extraction of the remaining tooth structure).
Statistical analysis
The homogeneity of data were evaluated using Kolmogorov-Smirnov and Levene normality tests.Statistical analysis was performed with software(SPSS20.0,SPSSInc,Chicago,IL).Fractureresistance data(N)wereanalyzed by one-way analysisof variance(ANOVA)followed by the Tukey HSD post hoc test(α=0.05)multiple comparisons.
Results
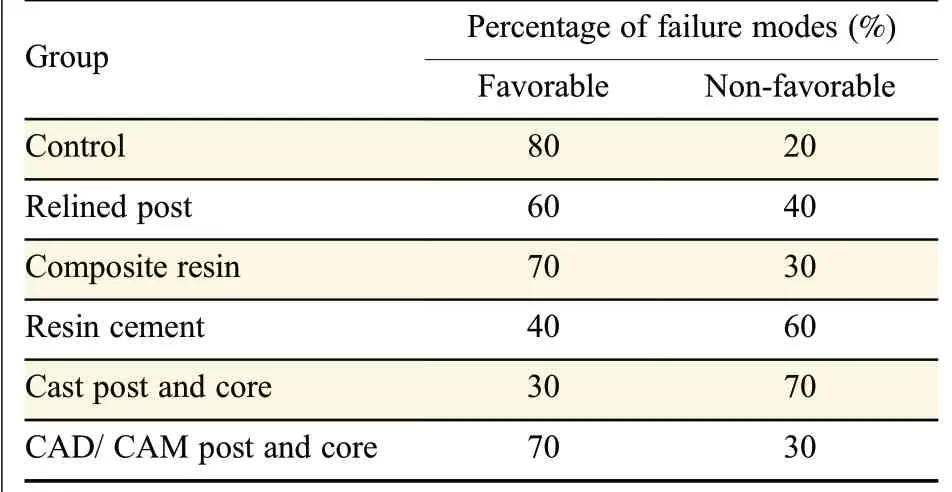
Table 2 Percentage of failure modes observed within each experimental group
Means and standard deviations of resistance to fracture values recorded for the test groups were listed in(Table1).Kolmogorov-Smirnov and Levenenormality tests revealed normal and relative(marginal)distributions of data.Therefore,a parametric ANOVA analysistestwasconducted to evaluatethedifferenceof fracture resistance values among groups(Table 2).

Fig.4 Photograph representing an exampleof a favorabletype of failurewith detachment of thepost and coresystem that could be repaired.
The highest overall fracture resistance(N)was observed in control group(827±39.1),followed by CPgroup[793.8±55.6)N]while the RCgroup showed the least fracture resistance values[(607.7±54.8)N].The CR reinforced group showed comparable fracture resistance values to the AP group where the mean values[(727.4±64.4)N]and[(686.2±52.5)N]respectively,while the CP showed comparable fracture resistance to CM group[(771±71.3)N].The results revealed a signi f i cant difference(P<0.05)in fracture resistance values of the CPgroup compared to the CR,AP and RC groups.No signi f i cant differences were found among fractureresistancevaluesof the APgroup compared to CR groups.Additional analysis with the Tukey test showed signi f i cant differences(P<0.001)among study groups as well.Predominately restorable failure observed in the Cgroup was 80%while the CP and CR groups recorded 70%as shown in Table 3.However,groups RC,AP and CM recorded a lesser percentage of favorable failure(60%,40%and 30%,respectively(Fig.4-5).

Fig.5 Photograph representing an exampleof a non-favorable typeof failurewith an obliquefracturebelow thecervical third of root that would necessitate extraction of the remaining tooth structure.
Discussion
Restoration of root-canal treated teeth with wide root canals using post and core systems still a challenging process as the mismatch between the wide diameter of the f l ared root canals and standardized rounded diameter of prefabricated post results in thick cement layer.Furthermore,the restoration of these f l ared root canals may be a compromised treatment as the remaining tooth structure is too weak to tolerate the normal masticatory forces and as a consequence the teeth areliableto fractures[21-22].The f i ndingsof this in vitro investigation support the rejection of the null hypothesis.There was a signi f i cant difference in resistance to fracture of endodontically treated teeth with non-f l ared root canals compared to teeth with f l ared root canals restored with f i ber post,cast post and core and CAM/CAM post and core.
The higher resistance to fracture values recorded for the control group can be explained by the greater amount of remaining dentin.Dentin exhibits considerable plastic deformation that enables resistance of different angles and degrees of load applied during normal occlusal function.Tooth fracture occurs when the applied loads exceeded the tensile strength or proportional limit of dentin as capability of dentin for plastic deformation is decreased.This result is supported by the f i nding of Zogheib et al.[17],who stated that the fracture resistance of endodontically treated teeth is directly proportional to the amount of remaining root canal dentin.
The CP group showed higher resistance to fracture values compared to CR,AP and RC groups.This f i nding could be related to the modulus of elasticity of VITA Enamic which is comparable to those of the hard tooth structure[31-33].Additionally,the difference in chemistry between the composite core material and the epoxy resin of the f i ber post matrix,a weak link is formed which ispartially responsiblefor thehigh failure rate happened in preformed f i ber post and core systems.In order to overcome the failure at interfaces,the post and the core should be fabricated as one piece.
The f i nding of this study showed that the root resistance to fracture of the CR group was signi f i cantly higher than the RC group.This f i nding was supported by a study conducted by Amin et al.[21]who reported that reinforcement of the f l ared post space using composite resin improved the fracture resistance of the weakened roots compared to rehabilitated using luting cement.Additionally,thick layersof resin cement incorporate more bubbles,cracks,or gaps compared to thethin one.Thesedefectsinitiateastressconcentration zone,which acts as crack raisers and reduces the bond strength of the f i ber post to root canal dentin[25].Root fracturemight beinduced dueto thewedging effect of a loose post within a root canal as a result of adhesion failurebetween rootcanal dentin and resin cements.The stress accumulated in the post is transferred by the dentin to theouter surfaceof the tooth.In caseof athin dentinal wall and/or thick resin cement layer,the load required to initiate tooth fracture is minimized,as occurred in groups RC and APin this study.
Although the use of anatomical post increases the post adaptation to root canal walls and decreases the thickness of resin cement[22-23,27].Gomes et al.[24]showed that the use of composite resin as a root reinforcement material improves fracture resistance of weekend root compared to the use of direct anatomical post.Other studies[18,25-26]reported that,to strengthen root-canal treated teeth with f l ared root canals,a f i rm bond between restorativematerialsand therootdentinis critical.However,various complicating factors could interfere with f i rm adhesion.Macedo et al.[22]reported that the use of relined post results in increased pull-out bond strengths compared with non-relined post which could be related to the higher adaptation of the post-torootcanal which increasesthesustained pressureduring cementation process and consequently reduces blister formation in thecementthatactsasastressraiser during testing.Restoration of root-canal treated teeth should be managed with one-piece post and core system with an adequate f i t of the post into theroot canal to reduce the liability of root fracture.
Failure mode analysis of the test groups revealed the prevalence of a favorable type of failure within C,CP and CR groups.This could be related to the thicker dentin layer in the control group,which increases root fractureresistance.In theother hand,thefavorabletype of failure observed in the CPgroup could be a result of itsmodulusof elasticity thatissimilar to thoseof dentin.On the contrary,AP and RC groups showed the prevalence of catastrophic failure.These f i ndings are in accordance with the results of other studies[22,24].As the use of glass f i ber posts are increasing for restoring endodontically treated teeth,further studies should be conducted to assess not only the appropriate method to restore f l ared root canal but also the appropriate post length that recommended in such situations.
The present study was an in vitro investigation that could not fully replicate the oral conditions which was considered a limitation of this study.Additionally,the specimens were tested under a static loading condition,using three types of post and core systems,and the effect of ferrule was not tested.
In conclusions,theresistance to fracture of wideroot canalscan beenhanced by using one-piece CAM/CAM post and core asan alternative to the use of either glass f i ber post relined with composite resin,increasing the thickness of luting cement or the use of cast post and coresystem.However,thiswasan in vitro investigation and further in vivo studies are necessary.
杂志排行

THE JOURNAL OF BIOMEDICAL RESEARCH的其它文章
- Angiopoietin-like protein 3(ANGPTL3)de f i ciency and fam ilial combined hypolipidemia
- Design,synthesis and biological evaluation of selective survivin inhibitors
- Computer-aided identi f i cation of protein targets of four polyphenols in Alzheimer’s disease(AD)and validation in a mouse ADmodel
- Melatonin and/or rowatinex attenuate streptozotocin-induced diabetic renal injury in rats
- Effects of lysophosphatidic acid on human periodontal ligament stem cells from teeth extracted from dental patients
- Maxillary denture f l ange and occlusal discrepancies of Vertex ThermoSens in comparison with conventional heat-cured denture base materials