The application of the necessity-concerns framework in investigating adherence and beliefs about immunosuppressive medication among Chinese liver transplant recipients*
2017-07-05HongXiLiuShTengXioHongLinBinShngLuWngJingZhngYunJinZng
Hong-Xi Liu,Sh Teng,Xio-Hong Lin,Y-Bin Shng,Lu Wng,Jing Zhng, Yun-Jin Zng
aSchool of Nursing,Beijing University of Chinese Medicine,Beijing 100102,China
bGeneral Surgery Center,Beijing You'an Hospital,Capital Medical University,Beijing 100069,China
Original article
The application of the necessity-concerns framework in investigating adherence and beliefs about immunosuppressive medication among Chinese liver transplant recipients*
Hong-Xia Liua,*,Sha Tenga,Xiao-Hong Lina,Ya-Bin Shanga,Lu Wangb,Jing Zhangb, Yun-Jin Zangb
aSchool of Nursing,Beijing University of Chinese Medicine,Beijing 100102,China
bGeneral Surgery Center,Beijing You'an Hospital,Capital Medical University,Beijing 100069,China
a r t i c l e i n f o
Article history:
Liver transplant recipients
Immunosuppressive medication
Medication adherence
Belief in medication
Necessity-concerns framework
Objective:This study aimed to explore adherence to and beliefs about immunosuppressive medication using the Necessity-Concerns Framework(NCF)in liver transplant recipients.
Methods:A cross-sectional study performed in recipients who were at least 3 months post liver transplantation.A convenience sample of 243 recipients was recruited.Self-reported medication adherence was measured by the Basel Assessment of Adherence with Immunosuppressive Medication Scale(BAASIS).The NCF was operationalized using the Beliefs about Medication Questionnaire(BMQ)to assess the beliefs about necessity and concerns with taking immunosuppressive medication.
Results:One-hundred-forty-fi ve liver transplant recipients were non-adherent(59.67%).Compared to adherers,non-adherers had lower beliefs regarding the necessity of taking immunosuppressive medication and lower scores on the necessity-concerns different from adherers.
Conclusions:Non-adherence is common in liver transplant recipients.Non-adherers hold beliefs that are different from adherers.Efforts to increase adherence should be made by targeting medication beliefs.
©2017 Shanxi Medical Periodical Press.Publishing services by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
1.Introduction
With advanced transplantation procedures and immunosuppressive therapy,the survival rates of liver transplant recipients (LTRs)have improved worldwide.LTRs face a lifelong intake of immunosuppressive medication(ISM)to prevent rejection of the graft.One study reported that 25e50%of LTRs experienced rejection episodes,which were not only related to whether a therapy regimen was effective but also depended on whether the LTRs were adherent to the medical advice of taking ISM and undergoing regular medical follow up.1ISM nonadherence is related to an increased risk for late acute graft rejections,late graft failure,and increased healthcare costs.2e4Although strict adherence to ISM therapy is important for maintaining the graftfunction,LTRs do not always completely adhere to their regimen.Studies have shown that the self-reported ISM nonadherence prevalence ranges from 14%to 73%in LTRs.5e8However,the prevalence of ISM nonadherence in Chinese LTRs has not been well studied.
Enhancing adherence to immunosuppressive medications for at-risk recipients may prevent adverse outcomes(graft rejection and loss etc.)and improve long-term outcomes in liver transplantation.Recipients'beliefs about their medications appear to be critical to understanding patient adherence practices.Recipients can have concerns about,for example,the side effects of the medication or they may believe that the medication is not necessary for their health.Studies on patients'beliefs have identi fi ed the NCF as a useful method for operationalizing key beliefs that in fluence adherence.9,10The Framework argues that beliefs that medication is less necessary(necessity beliefs)or feelings of greater concerns about taking it(concerns)are related to lower adherence to medication,which have been found in many disease populations(e.g.,thalassemia patients,asthma,diabetes,arthritis,and depression).11e15The necessity-concerns difference score has also been found to be associated with adherence.15Given the importance of adherence to IMS in LTRs,this‘NCF’potentially helps clinicians to understand patients'attitudes and decisions about the ISM regimen and then to better assist their patients.Beliefs about medicines are different among different cultures;therefore,the purpose of this study was to evaluate the adherence to ISM and beliefs about ISM among Chinese liver transplant recipients and compare the beliefs about ISM between adherent and nonadherent recipients.
2.Methods
2.1.Study design and participants
A cross-sectionaldesign was administered in this study and was performed at the outpatient transplant clinic of a general hospital in Beijing.The inclusion criteria for the recipients were as follows: (1)18 years or older;(2)able to read and understand Chinese;(3) have a functioning liver-only transplant;(4)at least3 months posttransplant;and(5)voluntary participation.Recipients who had received more than one liver transplant or a simultaneous solid organ transplant were not included.
2.2.Ethics statement
This study was approved by the ethics committee of the Beijing University of Chinese Medicine in Beijing,China.The purpose,risks and bene fi ts ofthis study were explained to the participants before they were asked to participate.The participants were assured that participation was voluntary,and that choosing not to participate would not in fluence their clinicalcare.All the data from the study were assured for con fi dentiality.Written informed consent was obtained when collecting the data.
2.3.Data collection and measurements
Recipients who had an appointment at the clinic between April 2015 and November 2015 and who met the eligibility criteria were invited to participate in the study.Interested recipients were given the questionnaires and completed them in-person at the time of the clinic visit.A knowledgeable researcher answered any questions that recipients might have about the questionnaires or research program.It took approximately 20e30 min to fi nish the questionnaires.
ISM adherence was measured by the Basel Assessment of adherence to immunosuppressive medications scale(BAASIS), which(developed by the Leuven-Basel Adherence Research Group) is a self-reported instrument developed to assess the relevant dimensions of ISM adherence,16i.e.,taking adherence,timing adherence,drug holiday,and dose-reduction in the lastfour weeks. The BAASIS is a 4-item,6-Likert scale that has been validated in liver transplant recipients17with a Cronbach's alpha of 0.71;when used in other organ transplant recipients,18Cronbach's alpha was 0.70.A higher score corresponds to worse adherence.Nonadherence was de fi ned as a BAASIS score of more than 4.The Cronbach's alpha of this scale was 0.69 in the present study.
The beliefs about ISM were assessed using the 10-item Beliefs about Medicines Questionnaire(BMQ),which is a reliable and validated scale.19The BMQ includes two subscales thatmeasure the perceived necessity of taking a speci fi c medication for controlling disease(Necessity)and concerns about the potentialadverse consequences of taking it(Concern).Reported reliability coef fi cients for the Necessity and Concern scales ranged from 0.55 to 0.86.19All items are scored on a 5-point Likert scale;the item responses ranged from 1(strongly disagree)to 5(strongly agree).The total scores for both the Necessity and Concern scales ranged from 5 to 25.Higher scores indicate a stronger necessity and concern belief. The Cronbach's alpha scores of the two dimensions were 0.87 and 0.85 in the study.Some studies have calculated a“necessityconcern differential”by subtracting the Concern scale score from the Necessity scale score.15,20The score was on a differential range from20 toþ20.A positive score indicates that the patients rated their beliefs in the necessity of taking medications higher than concerns about the medication and vice versa.The necessityconcern framework was split at the scale midpoint to create the following 4 attitude groups:ambivalent(high necessity,high concerns);accepting(high necessity,low concerns);indifferent(low necessity,low concerns);and skeptical(low necessity,high concerns).
Demographic and clinical characteristic questionnaires were designed to collect information on the age,gender,marital status, education level,economic burden,health insurance,household registration,employment status,donor type,time post-transplant, and immunosuppressive medications prescribed.
2.4.Data analysis
Statistical analyses were performed using the SPSS 21.0 statistical package(SPSS Inc.,Chicago,IL,USA).Prior to data analysis,a test of normality was performed.Categorical variables were described as proportions,and continuous variables that were normally distributed were described as the mean±SD and median (inter-quartile range:Q1e Q3)for non-normally distributed continuous variables.Student's t test was used to compare the beliefs between the adherence and nonadherence groups(nonadherence was de fi ned as a BAASIS score of more than 4).Twosided P-values were set at 0.05.
3.Results
3.1.Participant characteristics
A total of 300 questionnaires were distributed,and all were returned;57 ofthemwere incomplete and considered to be invalid.Data from the remaining 243 questionnaires were included in the analysis.The recipients(n¼243)had a median age of 55 years (range:28e75),with 184 males(75.72%)and 59 females(24.28%). The majority were urban residents(n¼220,90.53%)and were married(n¼234,96.30%).Approximately half of the recipients (53.91%)were currently retired,36.63%were employed,and 9.46% were unemployed.The length oftime since transplantation ranged from 0.23 to 26.18 years,with a median time of 4.41 years.The demographic and clinicalcharacteristics ofthe study recipients are shown in Table 1.
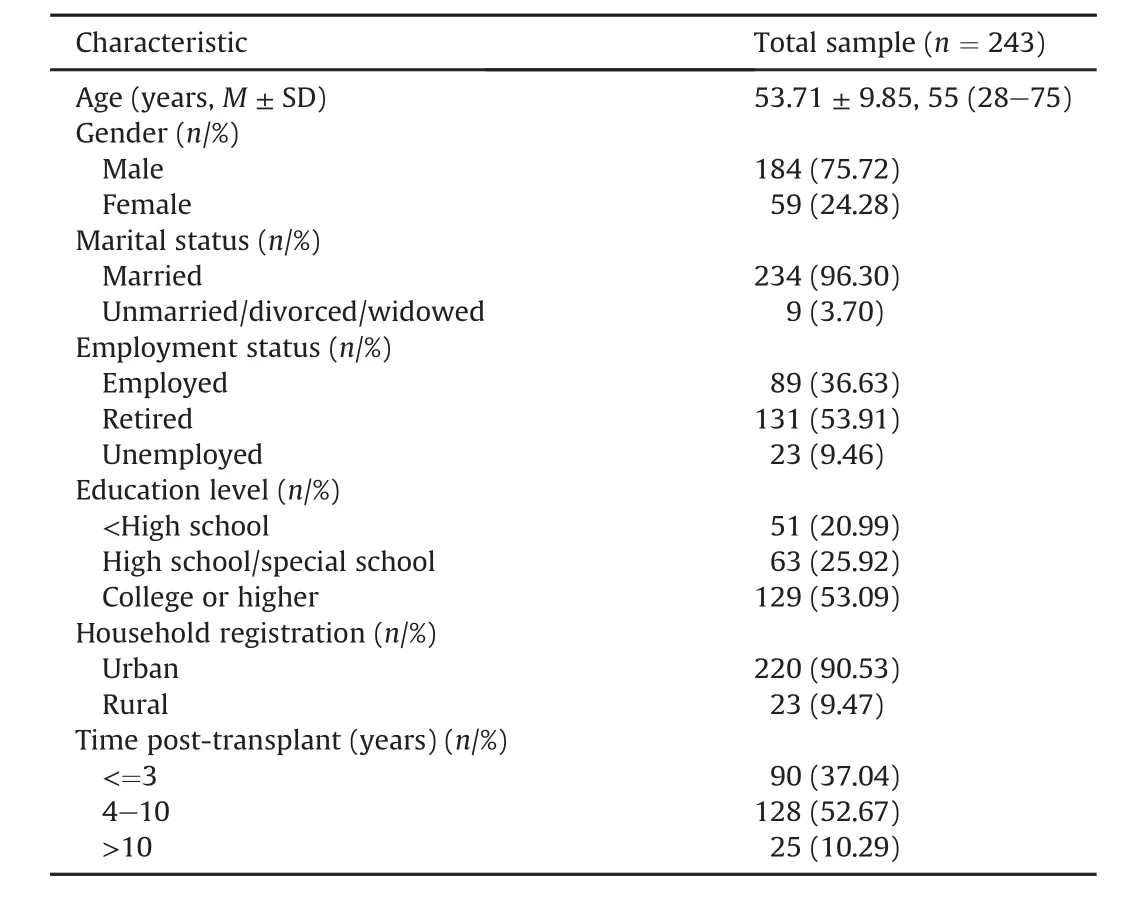
Table 1 Socio-demographic and clinical characteristics of participants.
3.2.Self-reported nonadherence
More than half(n¼145,59.67%)of the recipients reported nonadherence,with a score of more than 4.The median score on the BAASIS was 5(IQR 4e7).More than one-third(33.33%)of LTRs reported that sometimes they missed a dose of any of their immunosuppressive medications in the last four weeks;9.47%of LTRs reported that they skipped two or more doses of their medications on at least one occasion;47.74%of LTRs reported that sometimes they took their medications more than 2 h before or after the prescribed dosing time;and 11.93%reported that they altered the prescribed amount oftheir medications without telling their doctor.
3.3.Medication beliefs
The mean necessity score of the entire participants was 19.91±3.14,and the mean concern score was 15.26±4.17. Approximately 90.95%ofrecipients reported high necessity(higher than the midpoint of 15),with 50.21%reporting high concerns. Table 2 shows that 85.19%of the recipients agreed or strongly agreed that“My life would be impossible without my immunosuppressive medicines”and 81.07%of the recipients agreed or strongly agreed,“My health,at present,depends on my immunosuppressive medicines”.On the concern scale,61.73%agreed or strongly agreed that“I sometimes worry about the long-term effects of my immunosuppressive medicines”and more than onethird of LTRs reported worries in the other four items of concern scale.
A positive mean necessity-concerns differential of 4.65 was calculated.Few recipients(13.99%)had higher concerns than necessity.Mostparticipants(n¼209,86.01%)rated their beliefs in the necessity of taking medications higher than their concerns about the medication.Views about immunosuppressive medications were 45.68%accepting(high necessity,low concerns),45.28% ambivalent(high necessity,high concerns),4.12%indifferent(low necessity,low concerns),and 4.94%skeptical(low necessity,high concerns).
Student's t test indicated that medication beliefs varied signi ficantly in the adherence and nonadherence groups.Speci fi cally, compared to adherers,non-adherers had lower beliefs in the necessity of taking immunosuppressive medication(t¼ 8.337, p<0.001)and lower scores on the necessity-concerns differential than adherers(t¼4.606,p<0.001).
4.Discussion
In the currentstudy,immunosuppressive medication adherence and the difference in beliefs between the medication adherence and nonadherence groups was assessed in Chinese liver transplant recipients.Nonadherence was found in 59.67%of liver transplant recipients in our study,which was within the medication nonadherence range of 14e73%found in previous studies.5e8The fi nding in this study con fi rmed that ISM nonadherence was prevalent among liver transplant recipients.We should pay more attention to the dif fi culty in taking immunosuppressive medication reported by our recipients.Timing adherence performed the worst among taking adherence,timing adherence,drug holiday and dosing adherence in our study,and this is in agreement with Gordon's study results.21The ISMtiming is important considering that taking doses early may increase the chances of perceiving the side effects of ISMand taking doses later may increase the chance of the ISMlevelfalling below therapeutic levels,with an increased chance of graft rejection.22A previous study indicated that even small deviations from the prescribed ISM may harm the transplant graft.23Interventions designed to increase adherence are recommended.
The results of our study showed that most recipients strongly believe that immunosuppressive medications are necessary for their current and future health.However,some recipients expressed concerns about the adverse consequences of taking immunosuppressive medications.As immunosuppressive medications are life sustaining for liver transplant recipients,it is not surprising that most of recipients rated their beliefs on the necessity of taking medications higher than concerns about the medication(a positive necessity-concerns differential).Recipients need to understand that the medications have an acceptable safety pro fi le for long-term use.
Although our study cannot support a causal conclusion,we found thatnon-adherers had lower beliefs in the necessity oftaking immunosuppressive medication.Several theoretical models(e.g., Social-Cognitive Theory,Health Beliefs Model,and Commonsense/ Self S Regulation Model)address that beliefs determine behavior. Horne et al.24postulated that medication adherence is determined by patients'perception of whether they need medication and whether it will cause adverse consequences.Our fi ndings specifically support that non-adherers were signi fi cantly more likely to have stronger concerns about taking immunosuppressive medication and to doubt their personalneed for taking it,which is similar to previous studies using the BMQ.24,25A possible reason may be that recipients who have a low perception of the necessity of theirmedications and a high level of concern may be prone to forget to take it because of the low importance they ascribe to the medication.26

Table 2 Beliefs about ISM among Chinese liver transplant recipients(n/%).
Furthermore,non-adherers were signi fi cantly more likely to score lower on the necessity-concerns differential than adherers. The fact that recipients score a negative necessity-concerns differential would indicate a negative attitude towards these medications.This may indicate that even recipients were concerned about the troublesome side effects of their medications,but their fear of graft rejection and a strong perception regarding the need for ISM made them adherent to their ISM.The fi ndings revealed that recipients could be more motivated to adhere to their ISM if their belief in its necessity outweighs their concerns about taking it.15,20
One study showed that the beliefs about medicines were associated with patients'needs for information and counseling.27In clinicalpractice,the BMQ could be used as a simple toolto evaluate patient beliefs and identify who would bene fi t most from extra education.Education could address any questions patients might have and improve their attitudes towards the medication,which could in turn improve medication adherence.The data on the categoricalperspective ofthe necessity-concerns differentialcould lead to the development of belief promotion strategies for clinicians.For example,recipients who are indifferent about immunosuppressive medications might be in fluenced by socialfactors(e.g., patient e clinician relationship and social support).Recipients who are ambivalent about immunosuppressive medications might bene fi t from clinicians correcting their misunderstanding about taking medication and telling them that most side effects are transient or reversible.Recipients who are skeptical about immunosuppressive medications may not have good adherence until their perceived concerns diminish,needs increase or symptoms worsen.Clinicians may need to explore whether patients have a history of side effects or cultural beliefs about the medication.
The present study has some limitations.A convenience sample at a single transplant center may limit the generalization of the results because different transplant centers may differ in their instructions about medications and the frequency their transplant recipient follow up.Second,the use of a cross-sectional design cannot demonstrate that beliefs play a causal role.
5.Conclusions
In conclusion,more than half of liver transplant recipients acknowledged non-adherence in taking immunosuppressive medications in our study.Recipients who were adherent scored higher on the necessity scale and necessity-concern differential than recipients who were non-adherent.Given the fi ndings of this study,we suggest that the NCF could be used to measure patient beliefs and identify patients with a negative attitude towards immunosuppressive medications.
Conflict of interest
All contributing authors declare no con flicts of interest.
1.Corrao G,Parodi A,Nicotra F,et al.Better compliance to antihypertensive medications reduces cardiovascular risk.J Hypertens.2011;29:610e618.
2.O'Carroll RE,McGregor LM,Swanson V,Masterton G,Hayes PC.Adherence to medication after liver transplantation in Scotland:a pilot study.Liver Transpl. 2006;12:1862e1868.
3.Berlakovich GA,Langer F,Freundorfer E,et al.General compliance after liver transplantation for alcoholic cirrhosis.Transpl Int.2000;13:129e135.
4.Gaynor JJ,Ciancio G,Guerra G,et al.Graft failure due to noncompliance among 628 kidney transplant recipients with long-term follow-up:a single-center observational study.Transplantation.2014;97:925e933.
5.Rodrigue JR,Nelson DR,Hanto DW,Reed AI,Curry MP.Patient-reported immunosuppression nonadherence 6 to 24 months after liver transplant:association with pretransplant psychosocial factors and perceptions of health status change.Prog Transpl.2013;23:319e328.
6.Drent G,Haagsma EB,Geest SD,et al.Prevalence of prednisolone(non) compliance in adult liver transplant recipients.Transpl Int.2005;18:960e966.
7.Germani G,Gnoato F,Borella V,et al.473 non adherence to medical prescriptions in liver transplantation:a prospective longitudinal study.J Hepatol. 2010;52:183e317.
8.De Bleser L,Dobbels F,Berben L,et al.The spectrum of nonadherence with medication in heart,liver,and lung transplant patients assessed in various ways.Transpl Int.2011;24:882e891.
9.So fi anou A,Martynenko M,Wolf MS,et al.Asthma beliefs are associated with medication adherence in older asthmatics.J Gen Intern Med.2013;28:67e73.
10.Horne R,Chapman SC,Parham R,Freemantle N,Forbes A,Cooper V.Understanding patients'adherence-related beliefs about medicines prescribed for long-term conditions:a meta-analytic review of the Necessity-Concerns Framework.PLoS ONE.2013;8:e80633.
11.Mahler C,Hermann K,Horne R,Jank S,Haefeli WE,Szecsenyi J.Patients'beliefs about medicines in a primary care setting in Germany.J Eval Clin Pract. 2012;18:409e413.
12.Hedenrud T,Jonsson P,Linde M.Beliefs about medicines and adherence among Swedish migraineurs.Ann Pharmacother.2008;42:39e45.
13.Tibaldi G,Clatworthy J,Torchio E,Argentero P,Munizza C,Horne R.The utility of the Necessity-Concerns Framework in explaining treatment non-adherence in four chronic illness groups in Italy.Chronic Illn.2009;5:129e133.
14.Conn KM,Halterman JS,Fisher SG,Yoos HL,Chin NP,Szilagyi PG.Parental beliefs about medications and medication adherence among urban children with asthma.Ambul Pediatr.2005;5:306e310.
15.Clifford S,Barber N,Horne R.Understanding different beliefs held by adherers, unintentional nonadherers,and intentional nonadherers:application of the Necessity-Concerns Framework.J Psychosom Res.2008;64:41e46.
16.Dobbels F,Berben L,De Geest S,et al.The psychometric properties and practicability of self-report instruments to identify medication nonadherence in adult transplant patients:a systematic review.Transplantation.2010;90: 205e219.
17.Weng FL,Chandwani S,Kurtyka KM,Zacker C,Chisholm-Burns MA,Demissie K. Prevalence and correlates of medication non-adherence among kidney transplant recipients more than 6 months post-transplant:a cross-sectional study. BMC Nephrol.2013;14:261.
18.Marsicano Ede O,Fernandes Nda S,Colugnati F,et al.Transcultural adaptation and initialvalidation of Brazilian-Portuguese version ofthe Baselassessment of adherence to immunosuppressive medications scale(BAASIS)in kidney transplants.BMC Nephrol.2013;14:108.
19.Horne R,Weinman J,Hankins M.The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication.Psychol Health.1999;14:1e24.
20.Griva K,Davenport A,Harrison M,Newman SP.Non-adherence to immunosuppressive medications in kidney transplantation:intent vs.forgetfulness and clinical markers of medication intake.Ann Behav Med.2012;44:85e93.
21.Gordon EJ,Prohaska TR,Gallant MP,Siminoff LA.Adherence to immunosuppression:a prospective diary study.Transplant Proc.2007;39:3081e3085.
22.Russell CL,Cetingok M,Hamburger KQ,et al.Medication adherence in older renal transplant recipients.Clin Nurs Res.2010;19:95e112.
23.Nevins TE,Thomas W.Quantitative patterns of azathioprine adherence after renal transplantation.Transplantation.2009;87:711e718.
24.Butler JA,Peveler RC,Roderick P,Smith PW,Horne R,Mason JC.Modi fi able risk factors for non-adherence to immunosuppressants in renal transplant recipients:a cross-sectional study.Nephrol Dial Transpl.2004;19:3144e3149.
25.Denhaerynck K,Schmid-Mohler G,Kiss A,et al.Differences in medication adherence between living and deceased donor kidney transplant patients.Int J Organ Transpl Med.2014;5:7e14.
26.Horne R.Compliance,adherence,and concordance:implications for asthma treatment.Chest.2006;130:65S e72S.
27.van Geffen EC,Philbert D,van Boheemen C,van Dijk L,Bos MB,Bouvy ML. Patients'satisfaction with information and experiences with counseling on cardiovascular medication received at the pharmacy.Patient Educ Couns. 2011;83:303e309.
How to cite this article:Liu H-X,Teng S,Lin X-H,et al.The application ofthe necessity-concerns framework in investigating adherence and beliefs about immunosuppressive medication among Chinese liver transplant recipients.Chin Nurs Res. 2017;4:14e17.http://dx.doi.org/10.1016/j.cnre.2017.03.005
12 July 2016
*This project was supported by State Scholarship Fund(No.201506555004), China Scholarship Council,and Beijing Natural Science Foundation of China(No. 7144223).
*Corresponding author.
E-mail address:hongxia_t@163.com(H.-X.Liu).
Peer review under responsibility of Shanxi Medical Periodical Press.
http://dx.doi.org/10.1016/j.cnre.2017.03.005
2095-7718/©2017 ShanxiMedical PeriodicalPress.Publishing services by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons. org/licenses/by-nc-nd/4.0/).
Received in revised form 10 October 2016
Accepted 2 January 2017
Available online 31 March 2017
杂志排行

Frontiers of Nursing的其它文章
- Combined debridement in chronic wounds:A literature review
- Resilience as a strategy for struggling against challenges related to the nursing profession
- Changing trends and in fluencing factors of the quality of life of chemotherapy patients with breast cancer*
- Training indicators and quantitative criteria for emergency nurse specialists*
- Comparative research on the prognostic ability of improved early warning and APACHE II evaluation for hospitalized patients in the emergency department*
- Conversation with presence:A narrative inquiry into the learning experience of Chinese students studying nursing at Australian universities