血栓抽吸联合冠脉内给予尼可地尔对急性心肌梗死急诊PCI术后无复流的影响
2017-05-17吴君邓根群
吴君+邓根群
[摘要]目的 探讨血栓抽吸联合冠脉内给予尼可地尔对急性心肌梗死急诊PCI无复流的影响与安全性。方法 选取2014年12月~2015年12月我院收治的IRA术前TIMI≤1级的120例急性ST段抬高心肌梗死行急诊PCI患者,按病历号随机分为观察组和对照组,各60例,两组手术方法相同,出现无复流现象后分别经冠脉给予尼可地尔和硝酸甘油。比较两组注射药物后TIMI血流分级、TMPG分级、心电图ST段回落、住院期间的主要心血管事件。结果 观察组TIMI血流分级、TMPG分级优于对照组,差异有统计学意义(P<0.05)。观察组心电图ST段回落率高于对照组,差异有统计学意义(P<0.05)。观察组住院期间的主要不良心血管事件(MACE)发生率低于对照组,差异有统计学意义(P<0.05)。结论 AMI行急诊PCI血栓抽吸联合冠脉内给予尼可地尔可改善冠脉血流和梗死区的心肌再灌注,改善近期预后,安全有效。
[关键词]急性心肌梗死;经皮冠脉介入治疗;血栓抽吸;尼可地尔
[中图分类号] R541.4 [文献标识码] A [文章编号] 1674-4721(2017)03(a)-0060-04
[Abstract]Objective To investigate the effect and security of thrombus aspiration associated with Nicorandil in coronary on no-reflow of acute myocardial infarction after emergency percutaneous coronary intervention (PCI).Methods 120 patients in our hospital from December 2014 to December 2015,with emergency PCI for ST elevation myocardial infarction,preoperative infarction related artery (IRA) thrombolysis in myocardial infarction(TIMI)≤grade 1,were randomly divided into nicorandil group and control group according to the medical record number,each group had 60 patients.Two group did the same operation.When no-reflow after PCI appeared,intracoronary Nicorandil or Nitroglycerin was administered in each group separately.At the end of PCI,TIMI grade and TIMI myocardial perfusion grade (TMPG) were observed in the two groups,ST-segment down of ECG and the incidence of major adverse cardiac events (MACE) during hospitalization were compared between two groups.Results The proportion of with TIMI grade and TMPG grade of the nicorandil group was significantly better than that of the control group(P<0.05).The incidence rate of ST-segment down of the nicorandil group was significantly higher than that of the control group (P<0.05).The incidence rate of MACE in the nicorandil group was significantly lower than that in the control group before discharge (P<0.05).Conclusion The therapy of thrombus aspiration associated with Nicorandil in coronary for no-reflow of acute myocardial infarction after emergency PCI can improve coronary blood flow and myocardial reperfusion in infarct area,improve short-term prognosis and is safe and effective.
[Key words]Acute myocardial infarction;Percutaneous coronary intervention;Thrombus aspiration;Nicorandil
目前,直接經皮冠状动脉介入治疗(percutaneous coronary intervention,PCI)可尽早、充分、持续开通梗塞相关动脉,减少梗死心肌面积,改善左室功能,并降低主要不良心血管事件(MACE),已成为急性心肌梗死治疗的主要手段。尽管PCI在各级医院被广泛应用,但仍有部分患者术后心功能会继续恶化,猝死、心力衰竭等心血管事件高发。其原因认为与缺血再灌注损伤、无复流等有关,大量研究显示,术后冠状动脉无复流及慢血流提示心肌水平灌注不足,与心源性死亡、恶性心律失常、心脏机械并发症、充血性心力衰竭等有直接关联[1-4]。无复流的机制与冠脉微血管损伤有关,始于缺血时,而在再灌注时,中性粒细胞和血小板进入微循环释放自由基造成组织和内皮损伤,释放的各种缩血管物质导致的远端微血管痉挛是其重要原因。新型ATP敏感型K+通道开放剂尼可地尔,能扩张冠状动脉,减少梗死面积,减少冠脉结扎后再灌注心律失常的发生。动物实验证实其可抑制氧自由基和调控中性粒细胞活性,具有缺血预适应、降低无复流发生率等作用,可有效减轻PCI后再灌注损伤[5-8]。但关于尼可地尔在直接PCI术后的临床应用效果,尚缺乏大规模的临床研究证实。本研究旨在探讨急性心肌梗死行PCI治疗患者在常规血栓抽吸基础上,应用尼可地尔可否进一步改善术后无复流及近期临床效果,现报道如下。
1对象与方法
1.1研究对象
选择2014年12月~2015年12月我院收治的120例急性ST段抬高心肌梗死患者,发病24 h内仍有心肌缺血表现。行急诊冠脉造影,梗死相关动脉(IRA)术前心肌梗死溶栓(TIMI)≤1级。其中男70例,女50例,按病历号随机分为观察组和对照组,各60例。入选标准:胸痛≥30 min持续缓解;心电图成组导联ST段抬高,在肢导≥0.1 mV,胸导≥0.2 mV。排除标准:近期内脏活动性出血、颅内出血、严重肝肾功能不全、心源性休克及凝血功能障碍患者。两组入选基线资料具有可比性。观察组中,男性34例,女性26例,年龄(54.0±11.3)岁,对照组中,男性36例,女性24例,年龄(59.0±10.3)岁,两组性別及年龄比较,差异无统计学意义(P1=0.92,P2=0.48,P>0.05)。观察组中,吸烟20例,高血压病23例,糖尿病17例,对照组中,吸烟22例,高血压病21例,糖尿病16例,三项危险因素差异无统计学意义(P1=0.67,P2=0.89,P3=0.97,P>0.05)。观察组PCI术部位左前降支31例,左回旋支13例,右冠状动脉16例,对照组PCI术部位左前降支33例,左回旋支12例,右冠状动脉15例,支架部位差异无统计学意义(P1=0.68,P2=0.97,P3=0.56,P>0.05)。观察组植入支架(1.2±0.1)个,平均住院日(8.1±2.2)d,对照组植入支架(1.2±0.2)个,平均住院日(7.4±2.4)d,支架个数及平均住院日差异无统计学意义(P1=0.56,P2=0.18,P>0.05)。
1.2方法
两组患者入选后立即口服阿司匹林(嚼服)及氯吡格雷300 mg,常规肝素100 U/kg经动脉鞘内注射,常规按公斤体重使用替罗非班。
1.2.1观察组 先行血栓抽吸至少2次后依据IRA残余狭窄程度行球囊扩张后置入支架或直接置入支架,出现无复流者冠脉内给予尼可地尔(北京四环科宝制药有限公司,批准文号:国药准字H20120069)0.06 mg/kg,随后给予12 mg/h至术后12 h。
1.2.2对照组 常规方法行球囊扩张后支架置入,出现无复流者冠脉内硝酸甘油200 μg/次,最大剂量依据术中血压情况而定。
两组的术后低分子肝素5~7 d皮下注射5~7 d。
1.3无复流评价
①分级。TIMI 0级:闭塞动脉远端完全无血流;TIMI 1级:仅有少量对比剂通过闭塞血管,血管床充盈不完全;TIMI 2级:对比剂能完全充盈冠状动脉远端,但需>3个心动周期;TIMI 3级:3个心动周期内可以完全再灌注。②TIMI心肌灌注(TMPG)分级:0级为心肌完全无充盈及滞留;1级为有少量缓慢灌注,但不能自微血管排空,下一体位造影仍存在;2级为造影剂造影剂充盈延迟;滞留2~3个心动周期仍存在;3级为正常充盈微血管,2~3个心动周期完全排空。③无复流诊断标准:术后TIMI血流<3级,或尽管3级,心肌呈色为0或1级,或术后4 h ST段回落率仍<70%[3]。④心电图分析:术前和术后1 h心电图ST段测量以PR段为等电位线,测量QRS波后80 ms处ST段距基线。ST段抬高总和回落百分比≥70%为完全回落,31%~69%为部分回落,≤30%为无回落。⑤住院期间主要心血管不良事件。
1.4统计学方法
采用SPSS 13.0统计软件包对数据进行处理,计量资料用均数±标准差(x±s)表示,采用t检验,计数资料用百分率(%)表示,采用χ2检验,以P<0.05为差异有统计学意义。
2结果
2.1术后即刻冠脉血流
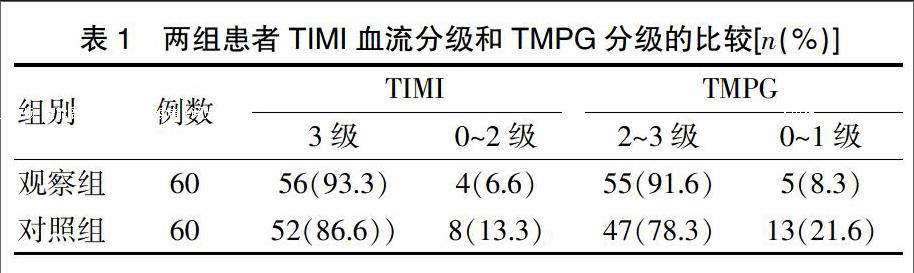
两组患者手术成功率均为100%,观察组TIMI血流分级和TMPG 分级均优于对照组(P<0.05)(表1)。
2.2心电图ST段回落率
观察组术后1 h心电图ST段完全回落54例,部分回落4例,无回落2例,对照组分别为47、3、10例观察组PCI术后ST段回落率高于对照组,差异有统计学意义(P<0.05)。
2.3 PCI后MACE及安全性
观察组发生1例再梗死,2例心衰,1例梗塞后心绞痛,1例死亡,对照组发生3例再梗死,8例心衰,4例梗塞后心绞痛,3例死亡,两组MACE发生率比较,差异有统计学意义(P<0.05)。两组患者出血事件多为齿龈出血、鼻出血、肉眼血尿、皮肤及黏膜淤斑、穿刺部位出血等。
3讨论
尼可地尔是首个临床应用作用于平滑肌的ATP敏感型K+通道开放剂,可同时激活鸟苷酸环化酶,升高细胞内环磷酸鸟苷,降低细胞内钙浓度,也具有硝酸酯类血管平滑肌松弛作用。可有效扩张正常冠脉和狭窄冠脉,增加冠脉血流,解除冠脉痉挛而被用于治疗冠心病心绞痛[9-14]。研究显示,心肌缺血预适应对于缩小心肌梗死面积和减轻恶性心律失常具有重要意义[15]。在局部心肌缺血预处理和心脏保护作用中起主导作用的是线粒体ATP敏感性钾通道,因而尼可地尔用于心肌梗死治疗时兼具有减少冠状动脉无复流的产生和缺血预适应的作用[16-19],从而改善心功能。在急性心肌梗死PCI的研究中日益受到关注。心肌组织无复流可导致心肌坏死、梗塞延展、心室重构以及恶性心律失常发生。在当今PCI时代,单纯冠脉再通在多数介入中心已可以顺利完成,进一步改善预后。微血管灌注日益受到重视。围手术期应用尼可地尔能改善无复流,减少再恶性心律失常的发生,降低再灌注损伤,从而有效改善左心室功能,降低心源性死亡和因心力衰竭的住院天数。无复流/慢复流主要与急性心肌梗死PCI术中动脉粥样硬化性微血栓致使远端微血管缺血以及血管内皮功能紊乱,再灌注时大量中性粒细胞及血小板进入微循环堵塞微血管,释放的各种缩血管物质导致的远端微血管痉挛等有关[20-26]。
本研究采用术中冠状动脉内和围术期静脉短期给药,观察尼可地尔对心肌缺血再灌注的保护效应,选取无复流现象作为观察指标,PCI术后心电图ST段回落及住院期间MACE为近期预后观察目标。结果尼可地尔组TIMI血流分级、TMPG分级、心电图ST段回落、住院期间的MACE发生率优于对照组(P<0.05),显示尼可地尔能减轻心脏缺血再灌注损伤,改善急性心梗PCI术后冠状动脉血流再灌注。这些作用可能与尼可地尔通过开放线粒体膜上的ATP敏感性钾通道,保护心肌细胞减少钙内流,促进线粒体呼吸和能量生成,模拟缺血预适应以及抑制过氧化产物形成有关[27-28]。同时尼可地尔本身具有硝酸酯类的扩张冠状动脉及扩张静脉作用,增加冠状动脉血流以减轻心脏负荷。
本研究显示,AMI急诊PCI患者尤其是血栓负荷重的患者常規采用血栓抽吸,在应用替罗非班基础上应用尼可地尔可改善冠脉血流,增加心肌灌注,还可改善近期预后,减少并预防无复流的发生。但是由于本研究样本量偏少,结果可能存在一定的偏倚。在当今PCI时代,仍需要更多大规模临床试验来进一步验证尼可地尔作为辅助药物对行急诊PCI 的急性ST 段抬高型心肌梗死患者预后的影响。
[参考文献]
[1]Svilaas T,Vlaar PJ,van der Horst IC,et al.Thrombus aspiration during primary percutaneous coronary intervention[J].N Engl J Med,2008,358(6):557-567.
[2]王国涛,马丽华,张文琪,等.急性ST段抬高心肌梗死直接经皮冠状动脉介入术冠状动脉无复流现象对预后的影响[J].中国心血管病研究杂志,2006,4(1):31-33.
[3]Van de Werf F,Ross A,Armstrong P,et al.Primary versus tenecteplase-facilitated percutaneous coronary intervention in patients with ST-segment elevation acute myocardial infarction(ASSENT-4 PCI):randomised trial[J].Lancet,2006, 367(9510):569-578.
[4]Brosh D,Assali AR,Mager A,et al.Effect of no-reflow during primary percutaneous coronary intervention for acute myocardial infarction on six-month mortality[J].Am J Cardiol,2007,99(4):442-445.
[5]陈艳丽,邹德玲,庞文跃,等.尼可地尔对稳定性心绞痛患者的疗效评价[J].实用药物与临床,2012,15(3):149-150.
[6]Auchampach JA,Cavero I,Gross G J.Nicorandil attenuates myocardial dysfunction associated with transient ischemia by opening ATP-dependent potassium channels[J].J Cardiovasc Pharmacol,1992,20(5):765-771.
[7]Sugimoto K,Ito H,Iwakura K,et al.Intravenous nicorandil in conjunction with coronary reperfusion therapy is associated with better clinical and functional outcomes in patients with acute myocardial infarction[J].Circ J,2003,67(4):295-300.
[8]Pieper GM,Gross GJ.Anti-free-radical and neutrophil-modulating properties of the nitrovasodilator,nicorandil[J].Cardiovasc Drugs Ther,1992,6(3):225-232.
[9]Simoons M,Ellis S.A clinical trial comparing primary coronary angioplasty with tissue plasminogen activator for acute myocardial infarction[J].N Engl J Med,1997,336(23):1621-1628.
[10]Taniyama Y,Ito H,Iwakura K,et al.Beneficial effect of intracoronary verapamil on microvascular and myocardial salvage in patients with acute myocardial infarction[J].J Am Coll Cardiol,1997,30(5):1193-1199.
[11]Sakata Y,Kodama K,Komamura K,et al.Salutary effect of adjunctive intracoronary nicorandil administration on restoration of myocardial blood flow and functional improvement in patients with acute myocardial infarction[J].Am Heart J,1997,133(6):616-621.
[12]Taira N.Nicorandil as a hybrid between nitrates and potassium channel activators[J].Am J Cardiol,1989,63(21):J18-J24.
[13]Auchampach JA,Cavero I,Gross GJ.Nicorandil attenuates myocardial dysfunction associated with transient ischemia by opening ATP-dependent potassium channels[J].J Cardiovasc Pharmacol,1992,20(5):765-771.
[14]Kempsford RD,Hawgood BJ.Assessment of the antiarrhythmic activity of nicorandil during myocardial ischemia and reperfusion[J].Eur J Pharmacol,1989,163(1):61-68.
[15]IONA Study Group.Effect of nicorandil on coronary events in patients with stable angina:the Impact of Nicorandil in Angina (IONA) randomised trial[J].Lancet,2002,359(9314): 1269-1275.
[16]Ito H,Taniyama Y,Iwakura K,et al.Intravenous nicorandil can preserve microvascular integrity and myocardial viability in patients with reperfused anterior wall myocardial infarction[J].J Am Coll Cardiol,1999,33(3):654-660.
[17]Ota S,Nishikawa H,Takeuchi M,et al.Impact of nicorandil to prevent reperfusion injury in patients with acute myocardial infarction sigmart multicenter angioplasty revascularization trial (SMART)[J].Circ J,2006,70(9):1099-1104.
[18]Ikeda N,Yasu T,Kubo N,et al.Nicorandil versus isosorbide dinitrate as adjunctive treatment to direct balloon angioplasty in acute myocardial infarction[J].Heart,2004,90(2):181-185.
[19]Kitakaze M,Minamino T,Node K,et al.Role of activation of ectosolic 5′-nucleotidase in the cardioprotection mediated by opening of K+ channels[J].Am J Physiol,1996, 270(5):H1744-H1756.
[20]Cura FA,Bhatt DL,Lincoff AM,et al.Pronounced benefit of coronary stenting and adjunctive platelet glycoprotein Ⅱb/Ⅲa inhibition in complex atherosclerotic lesions[J].Circulation,2000,102(1):28-34.
[21]Webb JG,Carere RG,Virmani R,et al.Retrieval and analysis of particulate debris after saphenous vein graft intervention[J].J Am Coll Cardiol,1999,34(2):468-475.
[22]Reffelmann T,Kloner RA.The "no-reflow" phenomenon:basic science and clinical correlates[J].Heart,2002,87(2):162-168.
[23]Ito H,Tomooka T,Sakai N,et al.Lack of myocardial perfusion immediately after successful thrombolysis.A predictor of poor recovery of left ventricular function in anterior myocardial infarction[J].Circulation,1992,85(5):1699-1705.
[24]Kaul S,Ito H.Microvasculature in acute myocardial ischemia:part Ⅱ evolving concepts in pathophysiology,diagnosis,and treatment[J].Circulation,2004,109(3):310-315.
[25]Ito H.No-reflow phenomenon and prognosis in patients with acute myocardial infarction[J].Nat Clin Prac Cardiovasc Med,2006,3(9):499-506.
[26]Choo EH,Kim PJ,Chang K,et al.The impact of no-reflow phenomena after primary percutaneous coronary intervention:a time-dependent analysis of mortality[J].Coronary Artery Dis,2014,25(5):392-398.
[27]Liu Y,Sato T,O′Rourke B,et al.Mitochondrial ATP-dependent potassium channels novel effectors of cardioprotection?[J].Circulation,1998,97(24):2463-2469.
[28]Dzeja PP,Holmuhamedov EL,Ozcan C,et al.Mitochondria gateway for cytoprotection[J].Circ Res,2001,89(9):744-746.
(收稿日期:2017-01-11 本文編辑:方菊花)
