luminal B型晚期乳腺癌临床病理特征及预后分析*
2017-04-19郑雅方贾勇圣郎荣刚佟仲生
郑雅方 贾勇圣 郎荣刚 佟仲生
luminal B型晚期乳腺癌临床病理特征及预后分析*
郑雅方 贾勇圣 郎荣刚 佟仲生
目的:探讨luminal B型晚期乳腺癌患者的临床病理特征及预后因素。方法:收集2008年6月至2013年6月天津医科大学肿瘤医院收治的206例luminal B型晚期乳腺癌患者的临床资料,回顾性分析其临床病理特征及影响预后的因素。结果:206例患者中HER-2阳性型54例(26.2%),HER-2阴性型152例(73.8%)。其中HER-2阳性型患者中Ki-67>30%为57.4%(31/54),较HER-2阴性型的55.9%(85/152)高,差异具有统计学意义(P<0.01);HER-2阳性型患者中无病生存期(disease free survival,DFS)<36个月为79.6%(43/54),较HER-2阴性型的65.1%(99/152)高,差异具有统计学意义(P<0.05)。206例患者的中位生存期为25(2.1~85.0)个月,是否合并内脏转移、一线解救化疗疗效、是否行解救内分泌治疗是luminal B型晚期乳腺癌患者的独立预后因素(P<0.05)。结论:luminal B型晚期乳腺癌患者中,HER-2阳性型中的Ki-67指数比HER-2阴性型更高,且更易在3年内发生复发、转移。合并内脏转移、一线解救化疗时病情进展、未行解救内分泌治疗是影响luminal B型晚期乳腺癌患者不良预后的独立因素。
乳腺癌 分子分型 复发 转移 治疗 预后
2011年St.Gallen共识提出,根据雌激素受体(ER)、孕激素受体(PR)、人表皮生长因子受体-2(HER-2)和细胞增殖标志Ki-67的表达情况,将乳腺癌分为luminal A型、luminal B型、HER-2过表达型和三阴性乳腺癌[1],luminal A和luminal B型统称为lu⁃minal型。不同分子亚型的乳腺癌预后具有显著性差异,luminal型乳腺癌中luminal B较luminal A型预后差[2]。未治疗的luminal B型乳腺癌的总生存期与HER-2过表达型及三阴性乳腺癌相似[3],luminal B型乳腺癌ER相关基因低表达,但增殖基因高表达,导致该型乳腺癌的治疗效果欠佳[4-5]。luminal B型乳腺癌自身的复杂性及不良预后给临床工作带来较大挑战,该型乳腺癌的研究尚较少,本研究通过回顾性分析206例luminal B型晚期乳腺癌的临床病理特征及预后因素,为临床个体化治疗提供更多的理论依据。
1 材料与方法
1.1 病例资料
收集2008年6月至2013年6月天津医科大学肿瘤医院收治的206例luminal B型晚期乳腺癌患者的临床病理资料。入选标准:女性,原发单侧乳腺癌,出现复发和(或)转移,临床病理资料齐全,完成随访。肿瘤复发和(或)转移部位经B超、CT、核磁、放射性核素扫描或PET-CT证实。排除男性乳腺癌、原发双乳癌及合并其他恶性肿瘤病史者、临床病理资料不完善者。符合luminal B型乳腺癌的标准如下:1)ER和(或)PR阳性,HER-2阴性,Ki-67≥14%(HER-2阴性型);2)ER和(或)PR阳性,HER-2阳性(HER-2阳性型)。ER、PR采用免疫组织化学方法检测,阳性细胞≥10%定义为阳性。HER-2使用国际公认的ASCO/CAP指南推荐的评分系统,HER-2免疫组织化学方法染色0或(+)评定为阴性,(+++)评定为阳性,(++)者采用荧光原位杂交技术(FISH)进行验证。本研究所有患者的分子分型均经病理科医生证实。
1.2 方法
通过门诊、住院检查及电话相结合的方式进行随访,随访截止至患者死亡或2016年6月15日。无病生存期(disease free survival,DFS)指从确诊开始至出现任何部位复发转移的时间。复发转移后总生存期(metastases-overall survival,M-OS)指从出现任何部位复发转移至因任何原因死亡或末次随访的时间。疗效评价根据WHO标准,包括完全缓解(CR)、部分缓解(PR)、疾病稳定(SD)、疾病进展(PD),其中完全缓解和部分缓解统称为有效缓解(CR+PR)。
1.3 统计学分析
采用SPSS 18.0软件进行统计学分析。各组数据间的比较采用χ2检验,应用Kaplan-Meier法进行生存分析,单因素分析采用Log-rank检验,多因素分析采用Cox比例风险回归模型。以P<0.05为差异具有统计学意义。
2 结果
2.1 患者的临床病理特征
206例患者中,除首次诊断为Ⅳ期的18例患者外,其余188例均接受乳腺癌根治术或改良根治术(91.3%),患者的中位年龄为46(23~73)岁。病理类型以浸润性导管癌为主、占90.3%(186/206),原发肿瘤大小主要集中在T2期、占53.9%(111/206),组织学分级以Ⅱ级为主、占85.0%(175/206),Ki-67指数>30%者居多、占56.3%(116/206),大部分患者DFS<36个月、占68.9%(142/206),见表1。

表1 206例Luminal B型晚期乳腺癌患者的临床病理特征 n(%)Table 1 Clinicopathological characteristics of 206 patients with advanced luminal B-like breast cancer n(%)
2.2 不同亚型的临床病理特征比较
206例患者中HER-2阳性型为54例(26.2%),HER-2阴性型为152例(73.8%)。对不同亚型患者的年龄、病理类型、肿瘤大小、淋巴结转移情况、临床分期、组织学分级、激素受体状态进行比较,差异均无统计学意义。HER-2阳性型与HER-2阴性型相比,Ki-67指数及DFS差异具有统计学意义(P<0.05,表1)。

表1 206例Luminal B型晚期乳腺癌患者的临床病理特征 n(%)(续表1)Table 1 Clinicopathological characteristics of 206 patients with advanced luminal B-like breast cancer n(%)
2.3 复发转移特征
206例患者的中位复发年龄为49(26~77)岁,中位DFS为23(0~90)个月。首次确诊复发转移时,部位单发者占42.7%(88/206),多发者占57.3%(118/206)。出现复发转移后,98.5%(203/206)接受了化疗,57.8%(119/ 206)接受了内分泌治疗,14.6%(30/206)接受了放疗。接受解救化疗患者中,(CR+PR)占31.0%(63/203),SD占53.7%(109/203),PD占15.3%(31/203)。
2.4 预后
全组患者的中位M-OS为25(2.1~85.0)个月。无内脏转移及合并内脏转移患者的中位M-OS分别为37.4和33.4个月,差异具有统计学意义(P<0.05,图1A);一线解救化疗疗效评价为(CR+PR)、SD和PD患者的中位M-OS分别为42.6、34.4和21.3个月,疗效为(CR+PR)及SD患者的中位M-OS明显优于PD者(P<0.05,图1B);行解救内分泌治疗和未行解救内分泌治疗患者的中位M-OS分别为38.6和21.7个月,差异具有统计学意义(P<0.05,图1C)。单因素分析显示,肿瘤大小、是否合并内脏转移、首发转移部位数目、一线解救化疗疗效、是否行解救内分泌治疗均与luminal B型晚期乳腺癌患者的预后相关(P<0.05,表2)。Cox多因素分析显示,是否合并内脏转移、一线解救化疗疗效、是否行解救内分泌治疗是luminal B型晚期乳腺癌的独立预后因素(P<0.05,表3)。
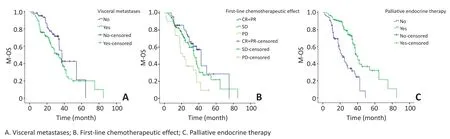
图1 luminal B型晚期乳腺癌患者内脏转移、一线解救化疗疗效及解救内分泌治疗的生存比较Figure 1 Comparison of M-OS in visceral metastases,first-line chemotherapeutic effect,and palliative endocrine therapy among patients with advanced luminal B-like breast cancer
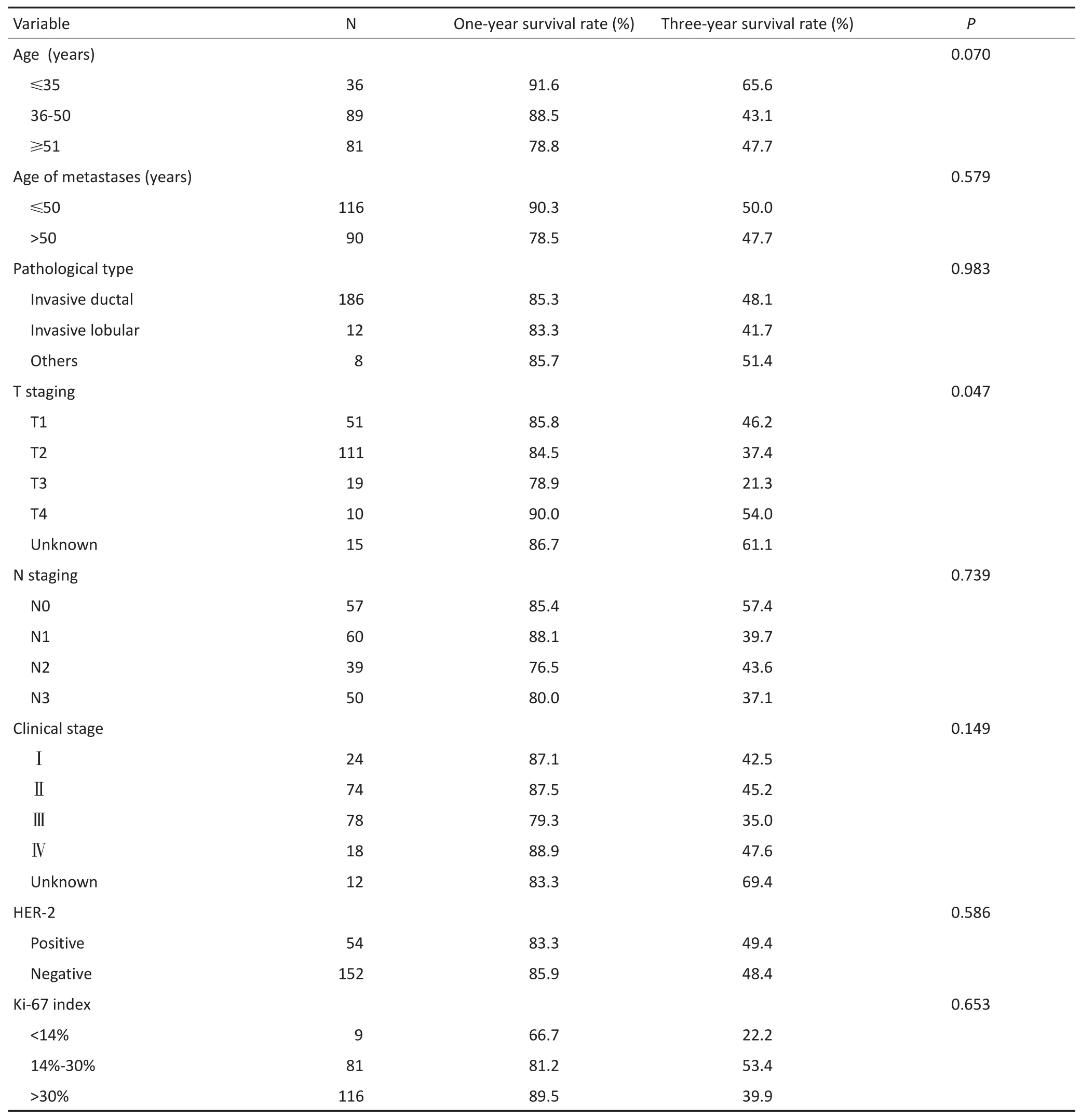
表2 206例luminal B型晚期乳腺癌患者预后的单因素分析Table 2 Univariate analyses of prognosis in 206 patients with advanced luminal B-like breast cancer
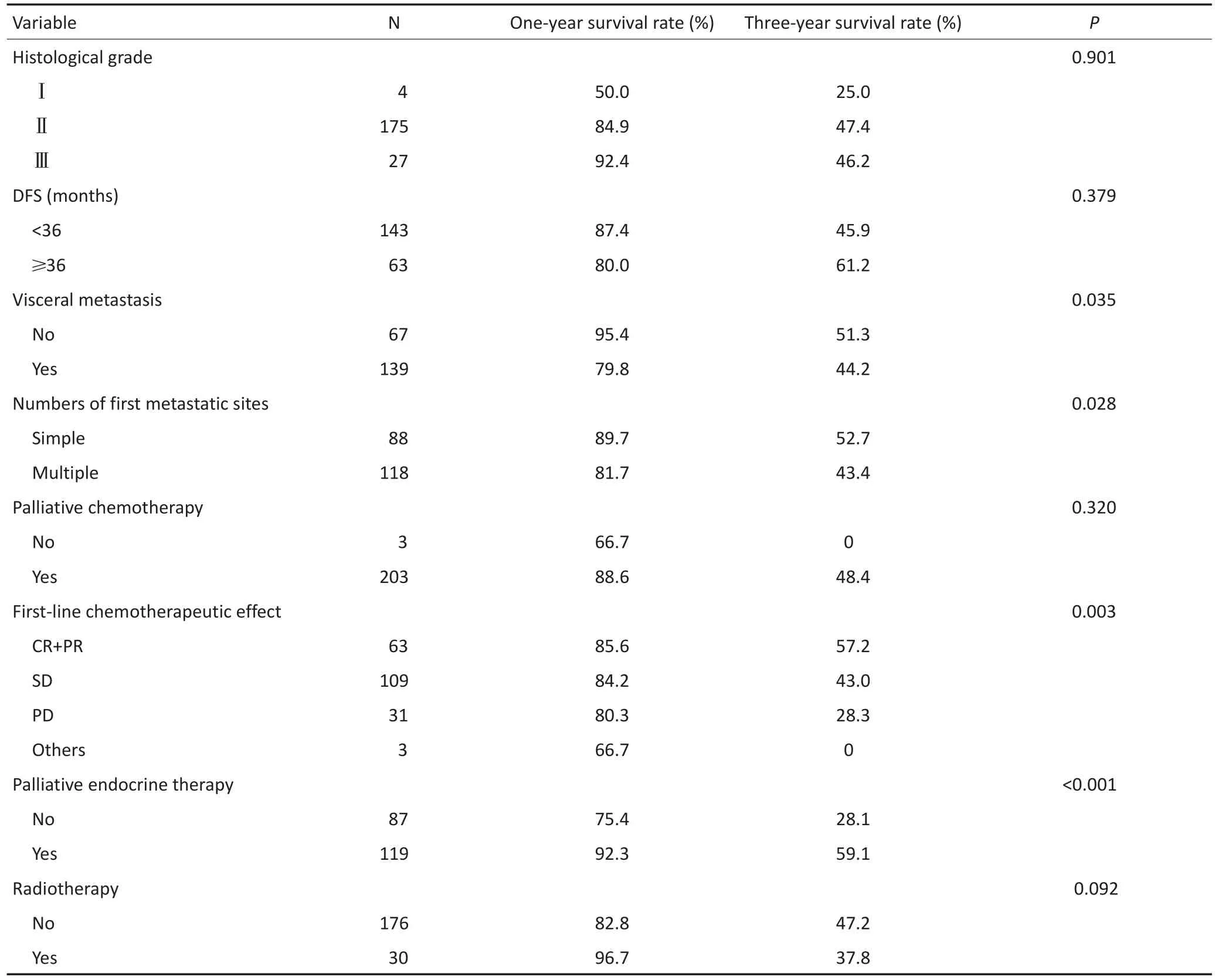
表2 206例luminal B型晚期乳腺癌患者预后的单因素分析(续表2)Table 2 Univariate analyses of prognosis in 206 patients with advanced luminal B-like breast cancer

表3 luminal B型晚期乳腺癌患者预后的Cox多因素分析Table 3 Multivariate analyses of prognosis in 206 patients with advanced luminal B-like breast cancer
3 讨论
luminal B型乳腺癌是一类异质性疾病,分为HER-2阳性和HER-2阴性两个亚型,由于研究方法、地域以及人群种属的不同,各分子亚型构成比例不尽相同。国外文献报道,约20%luminal B型乳腺癌为HER-2阳性[6],本研究中HER-2阳性型占26.2%(54/ 206)。
luminal B型乳腺癌淋巴结转移情况较分散[7],其中HER-2阳性型腋窝淋巴结转移率高于HER-2阴性型[8],且该型乳腺癌的组织学分级和Ki-67指数较高[9]。本研究中,HER-2阳性型患者的腋窝淋巴结转移率高于HER-2阴性型,但差异无统计学意义(P>0.05)。本研究患者组织学分级主要集中在Ⅱ级,Ki-67>30%者所占比例最高,其中HER-2阳性型中高指数Ki-67所占的比例较HER-2阴性型高,差异具有统计学意义(P<0.01)。国外文献报道,luminal型乳腺癌复发和(或)转移的时间较其他分子分型晚,但luminal B型乳腺癌的DFS却较短[10]。本研究68.9%(142/206)患者中,HER-2阳性型较HER-2阴性型患者更易在3年内发生复发和(或)转移。
一般认为,转移性乳腺癌的中位M-OS为2~3年,不同分子分型的患者的预后存在差别,本研究患者的中位M-OS为2.1年。远处转移是影响乳腺癌患者预后的重要因素之一,复发转移的部位和数目与预后密切相关。有文献报道,多发性转移或内脏转移的中位生存时间较无内脏转移者短,单发性转移是预后良好的指标[11]。本研究中,多发性转移及合并内脏转移患者的中位M-OS较单发性转移及无内脏转移者短,差异均具有统计学意义,与上述研究结果一致。luminal B型乳腺癌Ki-67指数截断值的选取,目前仍存在争议。2011年St.Gallen共识提出以14%作为区分luminal A和luminal B型的截断值。2013年St.Gallen共识将该截断值改为20%。目前有文献指出,“最佳”的Ki-67截断值是不存在的,临床上应该把Ki-67作为一个反映肿瘤增殖的连续指标[12]。本研究中,Ki-67>30%与Ki-67为14%~30%的患者相比,3年生存率有降低的趋势,提示Ki-67指数较高的luminal B型乳腺癌患者预后较差。
晚期乳腺癌患者最常用化疗及内分泌治疗[13-14]。本研究多数患者首次复发转移后接受蒽环和(或)紫衫类化疗方案,疗效为(CR+PR)及SD患者的中位M-OS明显长于PD者,患者一线化疗的疗效提高可延长改善患者生存。芳香化酶抑制剂内分泌治疗药物的应用可明显提高乳腺癌患者的生存率[15],luminal B型乳腺癌属于激素受体阳性乳腺癌,对内分泌治疗较敏感,本研究发现复发转移后接受内分泌治疗患者的预后明显优于未接受内分泌治疗者。因此,内分泌治疗是luminal B型晚期乳腺癌的重要治疗方法之一。
综上所述,luminal B型乳腺癌自身分子表达复杂,HER-2阳性型中的Ki-67指数比HER-2阴性型更高,且更易在3年内发生复发、转移。是否合并内脏转移、转移后一线化疗疗效及是否行内分泌治疗是影响luminal B型晚期乳腺癌的独立预后因素,对判断luminal B型晚期乳腺癌患者的预后及制定个体化治疗方案具有重要的指导意义。
[1]Goldhirsch A,Wood WC,Goates AS,et al.Strategies for subtypes--dealing with the diversity of breast cancer:highlights of the St.Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2011[J].Ann Oncol,2011,22(8):1736-1747.
[2]He ZY,Wu SG,Yang Q,et al.Breast cancer subtype is associated with axillary lymph node metastasis:a retrospective cohort study [J].Medicine(Baltimore),2015,94(48):e2213.
[3]Hu Z,Fan C,Oh DS,et al.The molecular portraits of breast tumors are conserved across microarray platforms[J].BMC Genomics,2006,7:96.
[4]Harbeck N,Thomssen C,Gnant M.St.Gallen 2013:brief preliminary summary of the consensus discussion[J].Breast Care(Basel), 2013,8(2):102-109.
[5]Gyöorffy B,Schäfer R.Meta-analysis of gene expression profiles related to relapse-free survival in 1,079 breast cancer patients[J]. Breast Cancer Res Treat,2009,118(3):433-441.
[6]Wirapati P,Sotiriou C,Kunkel S,et al.Meta-analysis of gene expression profiles in breast cancer:toward a unified understanding of breast cancer subtyping and prognosis signatures[J].Breast Cancer Res,2008, 10(4):R65.
[7]Zhu X,Ying J,Wang F,et al.Estrogen receptor,progesterone receptor,and human epidermal growth factor receptor 2 status in invasive breast cancer:a 3,198 cases study at National Cancer Center, China[J].Breast Cancer Res Treat,2014,147(3):551-555.
[8]Van Calster B,Vanden Bempt I,Drijkoningen M,et al.Axillary lymph node status of operable breast cancers by combined steroid receptor and HER-2 status:triple positive tumours are more likely lymph node positive[J].Breast Cancer Res Treat,2009,113(1):181-187.
[9]Tran B,Bedard PL.Luminal-B breast cancer and novel therapeutic targets[J].Breast Cancer Res,2011,13(6):221.
[10]Vici P,Pizzuti L,Natoli C,et al.Triple positive breast cancer:a distinct subtype[J]?Cancer Treat Rev,2015,41(2):69-76.
[11]Li ZH,Hu PH,Tu JH,et al.Luminal B breast cancer:patterns of recurrence and clinical outcome[J].Oncotarget,2016,7(40):65024-65033.
[12]Denkert C,Budczies J,von Minckwitz G,et al.Strategies for developing Ki67 as a useful biomarker in breast cancer[J].Breast,2015,24 (Suppl 2):67-72.
[13]Ren Z,Li Y,Hameed O,et al.Prognostic factors in patients with metastatic breast cancer at the time of diagnosis[J].Pathol Res Pract, 2014,210(5):301-306.
[14]Giordano SB,Gradishar W.Breast cancer:updates and advances in 2016[J].Curr Opin Obstet Gynecol,2017,29(1):12-17.
[15]Rugo HS,Rumble RB,Macrae E,et al.Endocrine therapy for hormone receptor-positive metastatic breast cancer:American Society of Clinical Oncology Guideline[J].J Clin Oncol,2016,34(25):3069-3103.
(2016-11-10收稿)
(2017-02-09修回)
Clinicopathological features and prognostic factors of patients with advanced luminal B-like breast cancer
Yafang ZHENG,Yongsheng JIA,Ronggang LANG,Zhongsheng TONG
Zhongsheng TONG;E-mail:tonghang@medmail.com.cn
Department of Breast Oncology,Tianjin Medical University Cancer Institute and Hospital,National Clinical Research Center for Cancer, Key Laboratory of Breast Cancer Prevention and Therapy(Ministry of Education),Tianjin Key Laboratory of Cancer Prevention and Therapy,Tianjin Clinical Research Center for Cancer,Tianjin 300060,China This work was supported by the National Science and Technology Pillar Program(No.2015BAI12B00)
Objective:To analyze the clinicopathological features and prognostic factors of advanced luminal B-like breast cancer.Methods:The clinicopathological features and prognostic factors of 206 patients with advanced luminal B-like breast cancer treated in our hospital between June 2008 and June 2013 were retrospectively analyzed.Results:Among 206 cases,human epidermal growth factor receptor 2(HER2)positive subtype was found in 54 cases(26.2%),whereas the negative subtype was found in 152 cases(73.8%).The proportion of Ki-67>30%in HER-2 positive subtype was significantly higher(57.4%;31/54)than that in HER-2 negative subtype (55.9%;85/152;P<0.01).The percentage of disease-free survival<36 months in HER-2 positive subtype was dramatically higher (79.6%;43/54)than that in HER-2 negative subtype(65.1%;99/152;P<0.05).The median overall survival of metastasis was 25(2.1-85.0)months.Multivariate analysis revealed that visceral metastases,first-line salvage chemotherapeutic effect,and palliative endocrine therapy were the independent predictors of survival in advanced luminal B-like breast cancer(P<0.05).Conclusion:Among patients with advanced luminal B-like breast cancer,HER-2 positive subtype was more commonly diagnosed with higher Ki-67 index, quicker and easier recurrence,and metastasis within three years than HER-2 negative subtype.Visceral metastases,poor effect of firstline salvage chemotherapy,and not receiving palliative endocrine therapy were independent factors of poor prognosis for the survival of advanced luminal B-like breast cancer.
breast cancer,molecular classification,recurrence,metastasis,treatment,prognosis
10.3969/j.issn.1000-8179.2017.04.298

天津医科大学肿瘤医院乳腺肿瘤内科,国家肿瘤临床医学研究中心,乳腺癌防治教育部重点实验室,天津市肿瘤防治重点实验室,天津市恶性肿瘤临床医学研究中心(天津市300060)
*本文课题受国家科技支撑计划项目(编号:2015BAI12B00)资助
佟仲生 tonghang@medmail.com.cn
郑雅方 专业方向为乳腺癌的综合治疗及肿瘤信号转导通路机制等基础研究。
E-mail:229872698@qq.com
