静注复合氨基酸与充气式升温机对肿瘤术后低体温无寒战患者的治疗效果比较
2016-11-17羊晰君缪长虹徐亚军张燕影苏子敏侯文婷葛圣金
羊晰君,缪长虹,徐亚军,张燕影,苏子敏,侯文婷,葛圣金
1.复旦大学附属肿瘤医院麻醉科,复旦大学上海医学院肿瘤学系,上海 200032;
2.复旦大学附属中山医院麻醉科,上海 200032
静注复合氨基酸与充气式升温机对肿瘤术后低体温无寒战患者的治疗效果比较
羊晰君1,缪长虹1,徐亚军1,张燕影2,苏子敏2,侯文婷1,葛圣金2
1.复旦大学附属肿瘤医院麻醉科,复旦大学上海医学院肿瘤学系,上海 200032;
2.复旦大学附属中山医院麻醉科,上海 200032
背景与目的:围术期低体温会影响肿瘤患者的预后,静脉输注氨基酸可以通过内源性产热升高体温,充气式升温机是普遍使用的治疗低体温的一种物理方式。本研究探讨静脉输注氨基酸对肿瘤患者术后低体温是否有治疗效果及与升温机相比的疗效。方法:选取57例胃癌患者,ASA Ⅰ~Ⅱ级,年龄18~60岁,在硬膜外复合全身麻醉下行胃癌根治术,术后中心温度低于36 ℃。进入苏醒室后随机分为3组(n=19):A组静脉输注氨基酸,速度2 mL·kg-1·h-1;B组给予充气式升温机;C组未给予干预措施。1 h内每5 min记录1次直肠体温及热舒适度,之后在2、6和24 h时分别记录口腔温度及热舒适度。患者进入苏醒室时及1 h后分别进行1次血气分析。结果:1 h时,A组和B组之间体温和热舒适度差异无统计学意义(P>0.05),但均显著高于C组(P<0.05);2和6 h时,A组体温和热舒适度明显高于B组和C组(P<0.05),B组和C组之间体温和热舒适度差异无统计学意义(P>0.05);24 h时,3组之间体温和热舒适度差异无统计学意义(P>0.05)。结论:静脉输注氨基酸升温效果优于充气式升温机,是治疗术后低体温更为有效便捷的方法。
复合氨基酸;充气式升温机;术后低体温;肿瘤转移
低体温一般指中心温度低于36 ℃,是围术期常见的并发症,发生率高达20%[1]。围术期低体温会引起患者凝血异常、失血量增大,术后感染机会增加,延长住院时间[2-3],使高危患者心脏不良事件如室速发生率增加3倍[4]。对于术后低体温患者,充气式升温机是普遍使用的一种物理治疗方式,其效果确切,操作安全方便,是较理想的治疗方法[5]。但在很多不发达地区,苏醒室内配置的充气式升温机数量有限,其使用范围明显受到限制。静脉输注氨基酸可以通过内源性产热升高体温[6],既往研究认为术前和术中输注氨基酸可以预防术后低体温的发生[7-8]。但静脉输注氨基酸对术后已发生低体温患者治疗效果的研究仍较少。对于围术期肿瘤患者,低体温可能会增加肿瘤细胞远处转移的发生率,显著影响肿瘤患者的预后[9]。因此,围术期肿瘤患者一旦发生低体温,必须及时接受治疗。本研究以围术期肿瘤患者为研究对象,将静脉输注氨基酸与使用充气式升温机比较,观察输注氨基酸对术后低体温肿瘤患者的治疗效果,以寻求治疗术后低体温更经济方便的方法。
1 资料和方法
1.1 一般资料
选取57例患者,ASA Ⅰ~Ⅱ级,年龄18~60岁,男女不限,在硬膜外复合全身麻醉下行胃癌根治术,术后进入苏醒室时中心温度低于36 ℃。排除标准:孕期及哺乳期女性;内分泌系统疾病;手术时间低于2 h或超过4 h(从划皮开始),选择此手术时间范围是因为如果手术时间过长会严重影响患者的体温调节功能;术前及术中输血的患者;在苏醒室内发生寒战;发生需要心血管活性药物治疗的低血压或高血压。本研究通过复旦大学附属中山医院伦理委员会审核,并在术前与患者签署知情同意书。
将57例患者随机分为3组,每组19例患者。A组给予输注复合氨基酸(乐凡命,复方氨基酸注射液,购自华瑞制药有限公司,以2 mL·kg-1·h-1(相当于0.92 kcal·kg-1·h-1)的输注速度持续输注1 h。B组使用充气式升温机复温1 h,充气式升温机包括主机Thermacare TC3146和Thermacare TC1050充气式保温毯(购自美国Gaymar公司)。温度设定在“high(43 ℃)”。C组未接受任何治疗。3组患者年龄、性别、身高、体质量和手术时间差异无统计学意义(P>0.05,表1)。
表 1 患者一般资料Tab. 1 The characteristics of patients

表 1 患者一般资料Tab. 1 The characteristics of patients
Characteristics Group A Group B Group C Gender(Male/Female) 15/4 13/6 16/3 Age/year 57.6±7.2 56.2±7.2 57.5±6.9 Weight m/kg 64.2±9.0 63.1±10.0 65.6±12.9 Height l/cm 168.0±5.6 168.5±7.4 166.7±6.3 Time t/min 178.4±7.8 188.0±4.5 181.6±5.5
1.2 方法
苏醒室温度保持22~24 ℃,相对湿度为40%~50%。患者入苏醒室后置入直肠体温探头(Drager体温探头,食道-直肠型,成人3M),温度探头连接于监护仪(购自美国Drager公司)。患者入苏醒室时记录基础温度并询问患者热舒适度(热舒适度评估采用VAS视觉分析法,0为极冷,50为温度适宜,100为极热)。之后1 h每隔5 min记录1次。随后在2、6和24 h时,因为患者已经由苏醒室转至病房,测量直肠温度存在困难,因此分别记录患者口腔温度和热舒适度。患者进入苏醒室时及1 h后分别进行1次血气分析。
1.3 统计学处理
2 结 果
2.1 直肠温度的变化
3组患者入苏醒室时基础体温差异无统计学意义(P>0.05,表2)。入苏醒室1 h后,A组体温[(36.50±0.33) ℃]与B组体温[(36.45±0.39) ℃]均显著升高,但差异无统计学意义(P>0.05)。而A组、B组体温均显著高于C组[(36.01±0.40) ℃,P<0.05]。
2.2 口腔温度的变化
2 h时,C组体温[(36.30±0.33) ℃]显著低于A组[(36.82±0.37) ℃]和B组[(36.52±0.42) ℃],差异有统计学意义(P<0.05),且A组显著高于B组(P<0.05)。6 h时,A组体温[(37.66±0.46) ℃]显著高于B组[(37.26±0.32) ℃]和C组[37.30±0.37) ℃,P<0.05]。B组和C组之间差异无统计学意义(P>0.05)。24 h时,3组之间体温差异无统计学意义(P>0.05,表2)。
2.3 热舒适度
1 h时,A组(50.00±1.41)与B组舒适度(51.11±1.44)之间差异无统计学意义(P>0.05),均优于C组(41.55±2.10,P<0.05)。2 h时,A组(50.00±2.61)优于B组(41.51±1.81)和C组(41.36±2.36,P<0.05),B、C组间差异无统计学意义(P>0.05)。6 h时,A组(50.00±3.12)优于B组(42.00±1.13)和C组(41.91±1.98,P<0.05),B、C组间差异无统计学意义(P>0.05)。24 h时,3组之间热舒适度差异无统计学意义(P>0.05,表3)。
2.4 血气分析
3组之间血气分析结果显示,除A组1 h血糖水平[(8.9±2.2) mmol/L]显著高于入苏醒室时[(7.2±2.1) mmol/L,P<0.05],其他指标前后差异无统计学意义(P>0.05,表4)。
表 2 患者平均体温Tab. 2 The mean temperature data from patients
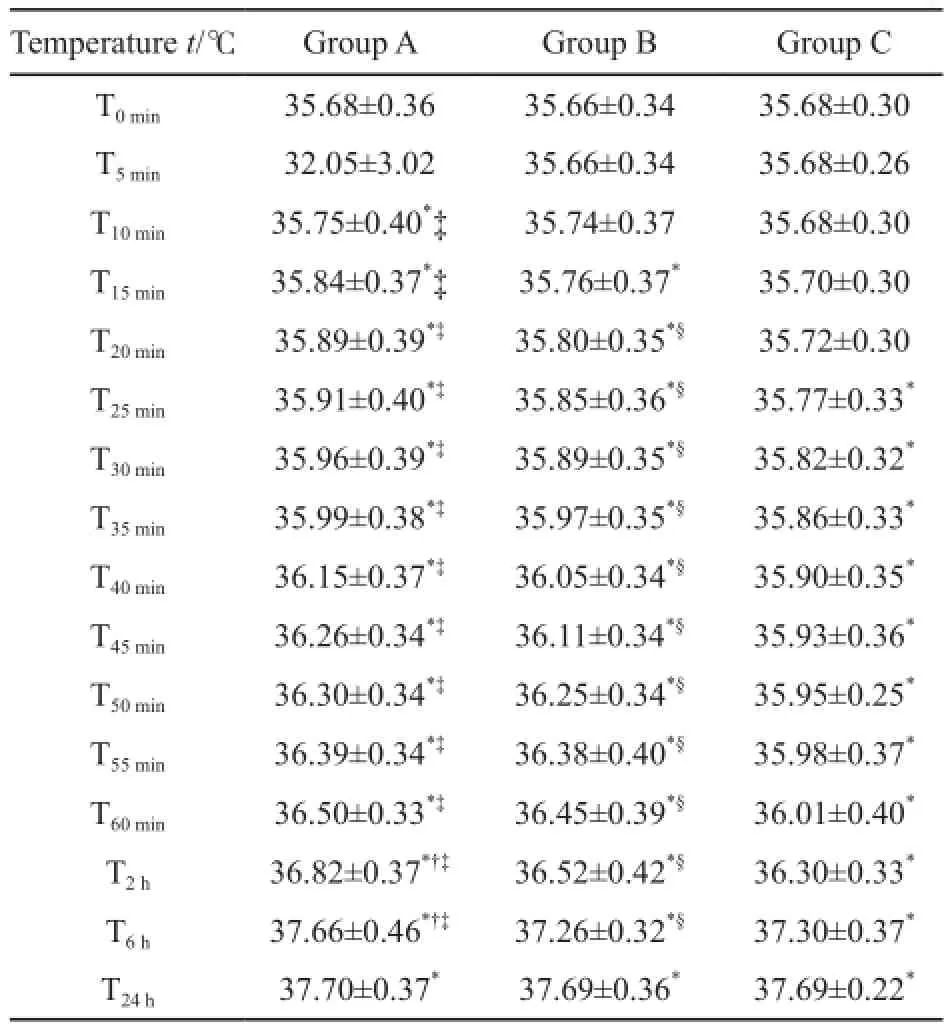
表 2 患者平均体温Tab. 2 The mean temperature data from patients
*: P<0.05, intragroup comparison with 0 min;†: P<0.05, group A vs group B;‡: P<0.05, group A vs group C;§: P<0.05, group B vs group C
Temperature t/℃ Group A Group B Group C T0min 35.68±0.36 35.66±0.34 35.68±0.30 T5min 32.05±3.02 35.66±0.34 35.68±0.26 T10min 35.75±0.40*‡ 35.74±0.37 35.68±0.30 T15min 35.84±0.37*‡ 35.76±0.37* 35.70±0.30 T20min 35.89±0.39*‡ 35.80±0.35*§ 35.72±0.30 T25min 35.91±0.40*‡ 35.85±0.36*§ 35.77±0.33*T30min 35.96±0.39*‡ 35.89±0.35*§ 35.82±0.32*T35min 35.99±0.38*‡ 35.97±0.35*§ 35.86±0.33*T40min 36.15±0.37*‡ 36.05±0.34*§ 35.90±0.35*T45min 36.26±0.34*‡ 36.11±0.34*§ 35.93±0.36*T50min 36.30±0.34*‡ 36.25±0.34*§ 35.95±0.25*T55min 36.39±0.34*‡ 36.38±0.40*§ 35.98±0.37*T60min 36.50±0.33*‡ 36.45±0.39*§ 36.01±0.40*T2h 36.82±0.37*†‡ 36.52±0.42*§ 36.30±0.33*T6h 37.66±0.46*†‡ 37.26±0.32*§ 37.30±0.37*T24h 37.70±0.37* 37.69±0.36* 37.69±0.22*
表 3 患者热舒适度Tab. 3 The thermal comfort data from patients

表 3 患者热舒适度Tab. 3 The thermal comfort data from patients
*: P<0.05, intragroup comparison with 0 min;†: P<0.05, group A vs group B;‡: P<0.05, group A vs group C;§: P<0.05, group B vs group C
Time t/min Group A Group B Group C 0 30.50±3.03 31.51±2.83 30.55±2.27 5 32.05±3.02 32.60±2.48 32.80±2.44 10 39.25±3.39* 38.67±2.18* 34.60±2.21 15 41.00±3.80*‡ 41.01±2.16* 35.75±2.27*20 44.85±3.62*‡ 43.96±1.84*§ 36.85±2.39*25 45.20±3.90*‡ 44.55±1.80*§ 37.10±2.60*30 46.35±2.68*‡ 46.20±1.81*§ 39.20±2.87*35 46.85±2.23*‡ 47.23±1.71*§ 40.20±2.70*40 47.40±1.84*‡ 48.35±1.70*§ 40.90±2.65*45 48.35±1.72*‡ 48.41±1.77*§ 40.85±2.57*50 49.70±1.48*‡ 48.96±1.67*§ 41.05±2.48*55 49.70±1.31*‡ 49.24±1.54*§ 41.75±2.38*60 50.00±1.41*‡ 51.11±1.44*§ 41.55±2.10*120 50.00±2.61*†‡ 41.51±1.81* 41.36±2.36*360 50.00±3.12*†‡ 42.00±1.13* 41.91±1.98*1440 50.00±3.44* 50.00±2.72* 50.00±2.27*
表 4 患者血气分析结果Tab. 4 The ABG data from patients
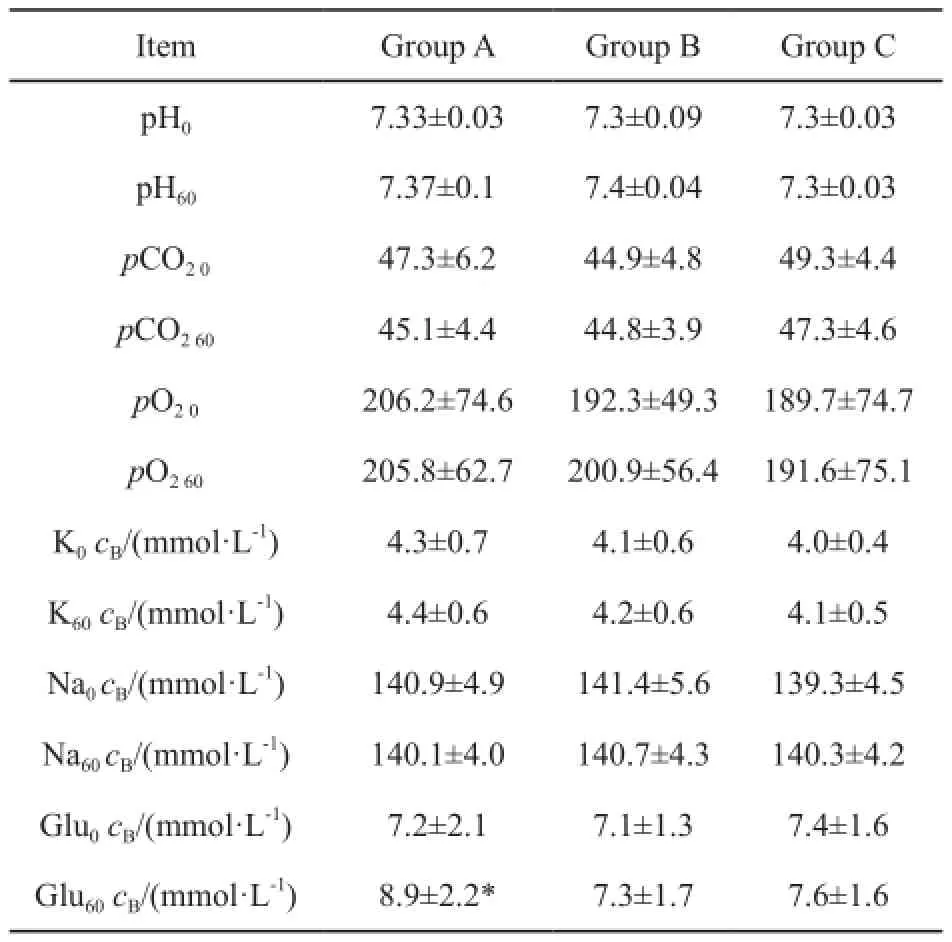
表 4 患者血气分析结果Tab. 4 The ABG data from patients
Item Group A Group B Group C pH0 7.33±0.03 7.3±0.09 7.3±0.03 pH60 7.37±0.1 7.4±0.04 7.3±0.03 pCO20 47.3±6.2 44.9±4.8 49.3±4.4 pCO260 45.1±4.4 44.8±3.9 47.3±4.6 pO20 206.2±74.6 192.3±49.3 189.7±74.7 pO260 205.8±62.7 200.9±56.4 191.6±75.1 K0cB/(mmol·L-1) 4.3±0.7 4.1±0.6 4.0±0.4 K60cB/(mmol·L-1) 4.4±0.6 4.2±0.6 4.1±0.5 Na0cB/(mmol·L-1) 140.9±4.9 141.4±5.6 139.3±4.5 Na60cB/(mmol·L-1) 140.1±4.0 140.7±4.3 140.3±4.2 Glu0cB/(mmol·L-1) 7.2±2.1 7.1±1.3 7.4±1.6 Glu60cB/(mmol·L-1) 8.9±2.2* 7.3±1.7 7.6±1.6
3 讨 论
因为术后低体温发生率较高,且会引起一系列不良后果。现在研究一般侧重于术前和术中预防。在术前及麻醉中输注氨基酸可以降低术后低体温的发生率。术中使用强制空气升温系统等物理方法也能减少热量丢失从而降低术后低体温的发生[10-11]。但有实验认为术前预热至少要30 min,才可以预防热量的重新分布和最后的低体温[11]。没有术前保温,即使术中使用升温措施也不能消除最初的体温下降。而即使使用预防性保温措施,术后低体温仍会发生。因此术后对低体温的治疗也同样重要。
本小组既往有研究针对术后低体温发生寒战的患者,明确输注氨基酸对术后寒战患者有显著疗效[12]。至于静脉输注氨基酸对于术后轻至中度低体温未发生寒战患者是否有治疗作用,既往无相关研究。因此本研究仅选取术后低体温无寒战的患者,剔除发生寒战的患者。本研究对胃癌术后发生低体温无寒战患者静脉输注复合氨基酸,患者体温和热舒适度升高明显。并且与充气式升温机相比较,氨基酸即使在停止输注后,升温作用可以持续至6 h。而充气式升温机在停止使用后,其升温作用消失,患者热舒适度也没有显著改善。因此,提示静脉输注氨基酸对术后发生的低体温有显著治疗作用,并且其长期升温效果明显优于充气式升温机。
清醒患者和麻醉状态下患者氨基酸升高体温的机制并不相同。对清醒患者,Selldén等[13]认为输注氨基酸可以通过营养物质生热效应激活氧化代谢,使代谢率增加大约20%,使得热蓄积明显增加,从而升高中心温度;而Nakajima等[14]认为氨基酸的产热效应可能是通过升高中枢体温调节的调定点,影响中枢温度调节控制来实现,氨基酸改变调定点的机制仍不是很清楚。但中心温度的升高和调定点的升高是一致的。无论是哪种机制,氨基酸升高体温主要是影响患者的中心温度,这是明确的。充气式升温机一方面通过吹出温暖的空气通过对流增加皮肤表面的热流,其传至皮肤表面的热量高达50 W[15];另一方面升高覆盖于皮肤表面的空气温度减少身体的热辐射,很快升高体温[16]。因此,充气式升温机主要是影响患者的体表温度。
本实验中无论输注氨基酸还是使用充气式升温机,在1 h内对术后低体温患者均有显著治疗效果,且升温作用相似。Selldén等[17]对于清醒健康志愿者持续输注氨基酸,结果显示热量积累在氨基酸输注终止后仍然存在,在停止输注后1.0~1.5 h体温达到最高。本研究中术后低体温患者在停止输注氨基酸后,同样表现出热量积累的持续,升温作用可以持续至6 h。充气式升温机在撤离后其升温作用随即消失。因此在实验2~6 h之间输注氨基酸升温效果要显著优于充气式升温机。
温度相关感觉可以分为温觉和热舒适度[18]。热舒适度主要依赖于大脑皮层整合中枢和外周温度传入信号产生[19]。体表温度和中心温度均能影响热舒适度。本实验在1 h内输注氨基酸和使用充气式升温机分别通过升高中心温度和外周温度来提高热舒适度。停用充气式升温机后,外来热量对体表感受刺激消失,而输注氨基酸仍有热量累积影响中心温度感受器,所以,2和6 h时氨基酸组的热舒适度优于升温机组。
本研究显示,氨基酸组患者在持续输注氨基酸1 h后,血糖显著升高,由(7.2±2.1) mmol/L上升至(8.9±2.2) mmol/L。输注氨基酸可以为糖异生和内源性葡萄糖生成提供底物,同时抑制葡萄糖转运和磷酸化,糖原合成减少[20]。这和本小组既往研究相一致,输注氨基酸会显著升高血糖水平,同时促进胰岛素和C肽分泌[21]。但是本实验中氨基酸组血糖水平升高未超过10 mmol/L,在围术期许可范围之内,所以无临床意义。
综上所述,对于胃癌术后低体温无寒战患者,静脉输注氨基酸升温效果在24 h内优于充气式升温机,升温作用持续时间远长于充气式升温机;复合氨基酸价格便宜,方便获取,是治疗术后低体温更为有效便捷的方法。
[1] KURZ A. Thermal care in the perioperative period [J]. Best Pract Res Clin Anaesthesiol, 2008, 22(1): 39-62.
[2] YAMAOKA I. Modification of core body temperature by amino acid administration [J]. Asia Pac J Clin Nutr, 2008, 17 Suppl 1: 309-311.
[3] RAJAGOPALAN S, MASCHA E, NA J, et al. The effects of mild perioperative hypothermia on blood loss and transfusion requirement [J]. Anesthesiology, 2008, 108(1): 71-77.
[4] FRANK S M, FLEISHER L A, BRESLOW M J, et al. Perioperative maintenance of normothermia reduces the incidence of morbid cardiac events. A randomized clinical trial[J]. JAMA, 1997, 277(14): 1127-1134.
[5] SESSLER D I, MOAYERI A. Skin-surface warming: heat flux and central temperature [J]. Anesthesiology, 1990, 73(2): 218-224.
[6] SELLDEN E, BRANSTROM R, BRUNDIN T. Augmented thermic effect of amino acids under general anaesthesia occurs predominantly in extra-splanchnic tissues [J]. Clin Sci(Lond), 1996, 91(4): 431-439.
[7] SELLDEN E, BRANSTROM R, BRUNDIN T. Preoperative infusion of amino acids prevents postoperative hypothermia[J]. Br J Anaesth, 1996, 76(2): 227-234.
[8] YAMAOKA I, DOI M, NAKAYAMA M, et al. Intravenous administration of amino acids during anesthesia stimulates muscle protein synthesis and heat accumulation in the body [J]. Am J Physiol Endocrinol Metab, 2006, 290(5): E882-E888.
[9] JIANG L, NICK A M, SOOD A K. Fundamental principles of cancer biology: Does it have relevance to the perioperative period? [J]. Curr Anesthesiol Rep, 2015, 5(3): 250-256.
[10] JANICKI P K, HIGGINS M S, JANSSEN J, et al. Comparison of two different temperature maintenance strategies during open abdominal surgery: upper body forced-air warming versus whole body water garment [J]. Anesthesiology,2001, 95(4): 868-874.
[11] PAULIKAS C A. Prevention of unplanned perioperative hypothermia [J]. Aorn J, 2008, 88(3): 358-368.
[12] ZHOU P, GE S, WANG Y, et al. Novamin infusion: a new method to cure postoperative shivering with hypothermia[J]. J Surg Res, 2014, 188(1): 69-76.
[13] SELLDÉN E, BRUNDIN T, WAHREN J. Augmented thermic effect of amino acids under general anaesthesia: a mechanism useful for prevention of anaesthesia-induced hypothermia[J]. Clin Sci (Lond), 1994, 86(5): 611-618.
[14] NAKAJIMA Y, TAKAMATA A, MATSUKAWA T, et al. Effect of amino acid infusion on central thermoregulatory control in humans [J]. Anesthesiology, 2004, 100(3): 634-639.
[15] SESSLER D I, MOAYERI A. Skin-surface warming: heat flux and central temperature [J]. Anesthesiology, 1990, 73(2): 218-224.
[16] WONG P F, KUMAR S, BOHRA A, et al. Randomized clinical trial of perioperative systemic warming in major elective abdominal surgery [J]. Br J Surg, 2007, 94(4): 421-426.
[17] SELLDEN E, BRANSTROM R, BRUNDIN T. Preoperative infusion of amino acids prevents postoperative hypothermia[J]. Br J Anaesth, 1996, 76(2): 227-234.
[18] NAKAMURA M, YODA T, CRAWSHAW L I, et al. Regional differences in temperature sensation and thermal comfort in humans [J]. J Appl Physiol, 2008, 105(6): 1897-1906.
[19] GOLJA P, KACIN A, TIPTON M J, et al. Moderate hypoxia does not affect the zone of thermal comfort in humans [J]. Eur J Appl Physiol, 2005, 93(5-6): 708-713.
[20] KREBS M, KRSSAK M, BERNROIDER E, et al. Mechanism of amino acid-induced skeletal muscle insulin resistance in humans [J]. Diabetes, 2002, 51(3): 599-605.
[21] ZHONG J, GE S J, ZHUANG X F, et al. Effect of intraoperative amino acid infusion on blood glucose under general anesthesia combined with epidural block [J]. Ann Nutr Metab, 2012, 61(1): 1-6.
Comparison of amino acid infusion with a forced-air warming system for rewarming hypothermic
postoperative cancer patients without shivering
YANG Xijun1, MIAO Changhong1, XU Yajun1, ZHANG Yanying2, SU Zimin2, Hou Wenting1, GE Shengjin2
(1.Department of Anesthesiology, Fudan University Shanghai Cancer Center, Department of Oncology, Shanghai Medical College, Fudan University, Shanghai 200032, China; 2.Department of Anesthesiology, Zhongshan Hospital, Fudan University, Shanghai 200032,China)
Correspondence to: GE Shengjin E-mail: shengjinge@163.com
Background and purpose: Perioperative hypothermia will affect the prognosis of cancer patients. Amino acid infusion can increase the core temperature by endogenous thermogenesis. And the forced-air warming system has gained high acceptance as a measure for rewarming. This study aimed to find out whether amino acid infusion was effective to treat postoperative hypothermia and how well the treatment effect was when compared with the forced-air warming system. Methods: Fifty-seven ASA Ⅰ or Ⅱ patients aged 18-60 years undergoing elective esophageal or gastric cancer operation under epidural-general anesthesia and whose core temperature were below 36 ℃. When admitted to the recovery room were randomly divided into 3 groups (n=19): Group Ⅰ-1·h-1(A); Group Ⅱ Conclusion: The rewarming effect of infusion of mixed amino acid is better than that of the forced-air warming system. It is the more effective and convenient method to rewarm the postoperative hypothermia.
a forced-air system (B); group Ⅲ
no therapy (C). Rectal temperature and thermal comfort were recorded per 5 min during the first 1 h and oral temperature and thermal comfort were recorded at the 2, 6 and 24 h. ABG was recorded when patients were admitted to the recovery room and at the first hour. Results: At the first hour, the rectal temperature and thermal comfort of groups A and B were higher when compared with group C (P<0.05), and there was no difference between groups A and B(P>0.05). At the second and sixth hour, the temperature and thermal comfort of group A were higher when compared with group B and C (P<0.05), and there was no difference between groups B and C (P>0.05). At the 24th hour, there were no statistically significant differences in the temperature and thermal comfort among the three groups (P>0.05).
intravenous infusion of mixed amino acid at a rate of 2 mL·kg
Mixed amino acid; Forced-air warming system; Postoperative hypothermia; Tumor metastasis
10.19401/j.cnki.1007-3639.2016.08.007
R730.5
A
1007-3639(2016)08-0682-05
葛圣金 E-mail:shengjinge@163.com
(2015-12-31
2016-03-23)
