更新的Diamond-Forrester法和Duke临床评分预测模型对可疑冠心病患者的诊断价值
2016-07-25吴俏玉罗爱静
贺 婷,刘 星,李 莹,吴俏玉,罗爱静,袁 洪
·论著·
更新的Diamond-Forrester法和Duke临床评分预测模型对可疑冠心病患者的诊断价值
贺 婷,刘 星,李 莹,吴俏玉,罗爱静,袁 洪
410013湖南省长沙市,中南大学湘雅三医院
【摘要】目的比较更新的Diamond-Forrester法(UDFM)和Duke临床评分(DCS)两种预测模型对我国可疑冠心病患者评估的准确性,并进一步分析两者在不同性别之间准确性的差异。方法选取2010年1月—2015年5月因胸痛在中南大学湘雅三医院心内科行冠状动脉造影(CAG)的患者1 311例。分别利用UDFM、DCS估算患者的验前概率(PTP),并分为低(<30%)、中(30%~70%)、高(>70%)PTP组,高PTP组即认为患有冠心病。以CAG为金标准,分析UDFM、DCS对我国可疑冠心病患者诊断的准确性,并进一步分析两者在不同性别之间准确性的差异。结果CAG结果显示,739例(56.37%)患者确诊为冠心病。UDFM结果显示,294(22.43%)、673(51.33%)、344(26.24%)例患者分别纳入低、中、高PTP组;DCS结果显示,165(12.59%)、403(30.74%)、743(56.67%)例患者分别纳入低、中、高PTP组。两者PTP分布比较,差异有统计学意义(χ2=379.00,P<0.001)。在确诊的739例患者中,UDFM将125(16.91%)、372(50.34%)、242(32.75%)例患者分别纳入低、中、高PTP组,DCS将64(8.66%)、189(25.58%)、486(65.76%)例患者分别纳入低、中、高PTP组,两者确诊患者PTP分布比较,差异有统计学意义(χ2=257.00,P<0.001)。以CAG为金标准,UDFM诊断冠心病的灵敏度为32.8%,特异度为82.2%,正确率为54.3%,受试者工作特征(ROC)曲线下面积为0.64〔95%CI(0.61,0.67)〕;DCS诊断冠心病的灵敏度为65.8%,特异度为55.1%,正确率为61.1%,ROC曲线下面积为0.63〔95%CI(0.60,0.66)〕。两者ROC曲线下面积比较,差异无统计学意义(Z=0.33,P>0.05)。UDFM对男性典型胸痛患者、不典型胸痛患者、非心绞痛型胸痛患者计算的PTP与实际阳性率较接近,而对女性患者,除50~59岁典型心绞痛患者存在高估现象外,余均存在低估现象;DCS对男性患者存在高估现象,对女性患者,除典型心绞痛患者存在高估现象外,余均存在低估现象。结论UDFM、DCS对于我国可疑冠心病患者的评估准确性不高,且存在性别差异。与欧美国家明显不同的是两者均对女性存在低估现象。因此,对我国可疑冠心病患者进行PTP的估算需要依据不同性别建立更为准确的模型。
【关键词】冠心病;验前概率;冠状血管造影术;诊断;灵敏度;特异度;更新的Diamond-Forrester法;Duke临床评分
贺婷,刘星,李莹,等.更新的Diamond-Forrester法和Duke临床评分预测模型对可疑冠心病患者的诊断价值[J].中国全科医学,2016,19(20):2440-2444.[www.chinagp.net]
HE T,LIU X,LI Y,et al.Diagnostic value of updated Diamond-Forrester method and Duck clinical score prediction model in patients with suspected coronary artery disease[J].Chinese General Practice,2016,19(20):2440-2444.
冠状动脉造影(coronary arteriography,CAG)作为诊断冠心病的金标准,已在临床得到广泛应用,但其在减少冠心病患者漏诊率的同时也带来过度医疗的问题。在一项包括近40万例既往无冠心病病史的患者研究中显示,CAG阳性率仅为37.6%[1],而且作为一项有创检查,其昂贵的费用以及术中、术后并发症也不容忽视。在最近发布的多个指南中强调通过验前概率(pretest probability,PTP)的估算指导行CAG患者的选择,从而提高CAG诊断阳性率[2-4],并把更新的Diamond-Forrester法(updated Diamond-Forrester method,UDFM)[5]、Duke临床评分(Duke clinical score,DCS)[6]作为估算PTP的首选模型。但由于这两个模型的建立均是以欧美人群的数据为基础,而危险因素的分布差异以及种族差异会导致模型的有效性受到不同程度的影响[5]。而且,UDFM、DCS主要依据患者的临床特征以及部分男女共有危险因素来估算PTP,并没有纳入女性特有的危险因素。而以往研究表明,与女性相关的特有危险因素可以显著增加女性患冠心病的风险[7-8],因此,这两种模型评估的准确性是否存在性别差异有待进一步证实。本研究的目的是对UDFM、DCS在欧美以外的人群中进行外部验证,评价UDFM、DCS在我国人群中对可疑冠心病患者评估的准确性,并进一步分析两者在不同性别之间准确性的差异。
1对象与方法
1.1研究对象选取2010年1月—2015年5月因胸痛在湘雅三医院心内科行CAG的患者1 311例。纳入标准:(1)既往无冠心病病史;(2)此次因胸痛查因入院,疑诊为冠心病;(3)初次行CAG检查。排除标准:(1)入院诊断为不稳定型心绞痛和心肌梗死;(2)既往有陈旧性心肌梗死;(3)有冠状动脉血运重建史(包括冠状动脉介入治疗和冠状动脉旁路移植术)。
1.2研究方法及变量定义UDFM主要纳入性别、年龄、胸痛3个变量,PTPUDFM=1/〔1+e-(-4.37+0.04×年龄+α×性别+β×胸痛)〕,α=1.34(男)或0(女),β=1.91(典型心绞痛)或0.64(不典型心绞痛)或0(非心绞痛型胸痛);DCS纳入性别、年龄、胸痛、吸烟史、糖尿病病史、高脂血症、陈旧性心肌梗死、心电图改变(包括Q波及ST-T变化)8个变量,PTPDCS=1/(1+ea)〔注:a=-(-7.376+0.112 6×年龄-α×性别-0.030 1×年龄×性别+β×胸痛+2.596×吸烟+0.694×糖尿病+1.845×高脂血症+1.093×陈旧性心肌梗死+1.213×Q波+0.637×ST-T变化+0.741×陈旧性心肌梗死×Q波-0.040 4×年龄×吸烟-0.025 1×年龄×高脂血症+0.550×性别×吸烟)〕 ,>70岁的患者按照70岁(DCS的上限年龄)计算,α、β赋值同UDFM。通过电子病历系统收集患者相关临床资料,根据UDFM、DCS计算每例患者的PTP,并分为低(<30.0%)、中(30.0%~70.0%)、高(>70.0%)PTP组,高PTP组即认为患有冠心病,不需要进一步检查。以CAG为金标准,分析UDFM、DCS对我国可疑冠心病患者诊断的准确性。
胸痛特征划分:典型心绞痛主要有以下3个特征:(1)由劳累、体力运动或情绪激动诱发;(2)位于胸骨后或心前区;(3)经休息或含服硝酸酯类药物可于数分钟内缓解。若满足以上3个特征中的2项,则定义为不典型心绞痛,若仅满足1项或均不满足则定义为非心绞痛型胸痛[4,9]。患者的胸痛特征由两名心内科医生依据上述定义从病历记录中进行人工确认,若出现不一致时则共同讨论决定。
1.3CAG方法及结果判断所有患者行CAG,由心导管室专业医生在标准的导管室中完成操作,患者取常规体位,术者可以根据患者的具体情况以及以往的经验选择股动脉或桡动脉路径,送入导管注入造影剂,行左、右冠状动脉造影,采用裸眼判定方法,由2~3名经验丰富的专科医生判断心外膜下冠状动脉病变支数及狭窄程度。取各体位中病变的最大狭窄程度作为病变的狭窄程度。冠心病的诊断标准:至少一支主要冠状动脉或其分支内径狭窄≥50%。主要冠状动脉包括左主干、左前降支、左回旋支及右冠状动脉。主要分支包括第一对角支、第二对角支、钝缘支、锐缘支、左室后支、后降支。

2结果
2.1一般资料1 311例患者中男774例,女537例;年龄30~79岁,平均年龄(61.6±9.9)岁;典型心绞痛670例,不典型心绞痛429例,非心绞痛型胸痛患者212例。男性和女性年龄、糖尿病检出率、高脂血症检出率、吸烟史、高密度脂蛋白胆固醇(HDL-C)、低密度脂蛋白胆固醇(LDL-C)、三酰甘油(TG)、总胆固醇(TC)水平比较,差异均有统计学意义(P<0.05);男性和女性Q波、ST-T变化、估算肾小球滤过率(eGFR)、胸痛特征比较,差异均无统计学意义(P>0.05,见表1)。
2.2UDFM和DCS预测模型准确性分析根据CAG结果,共有739例(56.37%)患者确诊为冠心病。UDFM结果显示,294(22.43%)、673(51.33%)、344(26.24%)例患者分别纳入低、中、高PTP组;DCS结果显示,165(12.59%)、403(30.74%)、743(56.67%)例患者分别纳入低、中、高PTP组。两者PTP分布比较,差异有统计学意义(χ2=379.00,
P<0.001)。在确诊的739例患者中,UDFM将125(16.91%)、372(50.34%)、242(32.75%)例患者分别纳入低、中、高PTP组,DCS将64(8.66%)、189(25.58)、486(65.76%)例患者分别纳入低、中、高PTP组,两者确诊患者PTP分布比较,差异有统计学意义(χ2=257.00,P<0.001)。
以CAG为金标准,UDFM诊断冠心病的灵敏度为32.8%,特异度为82.2%,正确率为54.3%,AUC为0.64〔95%CI(0.61,0.67)〕;DCS诊断冠心病的灵敏度为65.8%,特异度为55.1%,正确率为61.1%,AUC为0.63〔95%CI(0.60,0.66)〕。两者AUC比较,差异无统计学意义(Z=0.33,P>0.05,见表2、图1)。
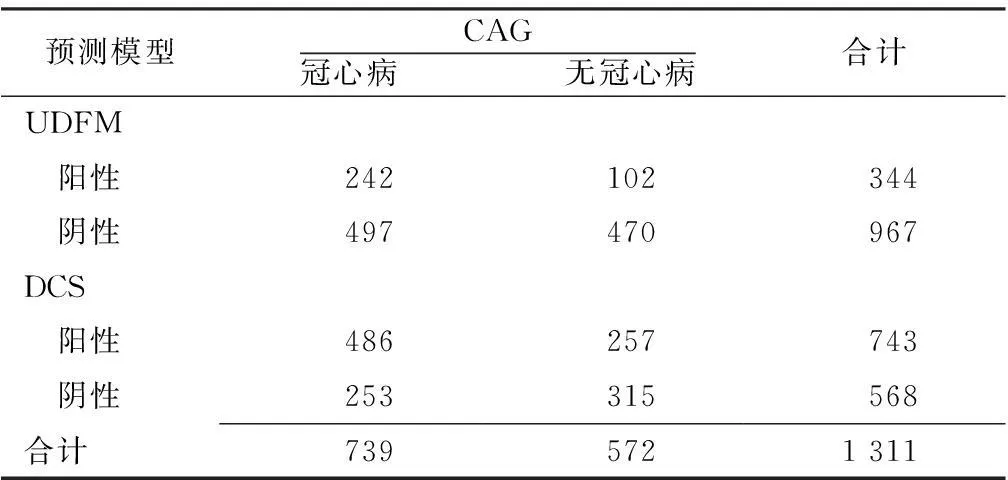
表2 UDFM、DCS对冠心病的诊断价值分析(例)
注:UDFM=更新的Diamond-Forrester法,DCS=Duke临床评分,CAG=冠状动脉造影
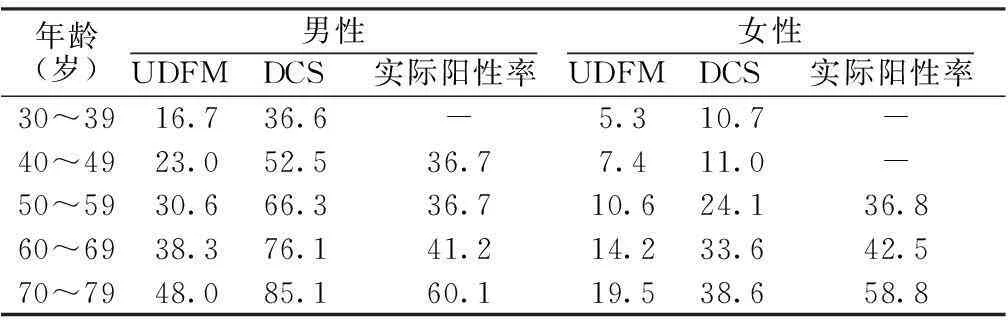
2.3UDFM和DCS在不同性别之间的准确性分析UDFM对男性典型胸痛患者、不典型胸痛患者、非心绞痛型胸痛患者计算的PTP与实际阳性率较接近,而对女性患者,除50~59岁典型心绞痛患者存在高估现象外,余均存在低估现象;DCS对男性患者存在高估现象,对女性患者,除典型心绞痛患者存在高估现象外,余均存在低估现象(见表3~5)。
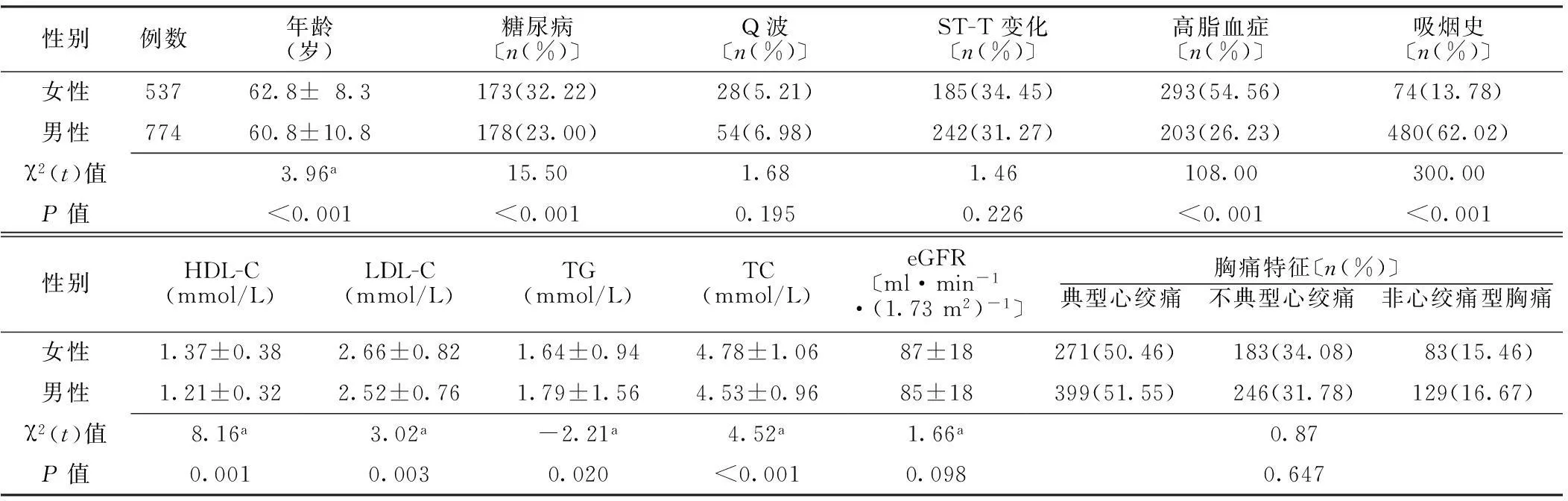
表1 不同性别患者一般资料比较
注:a为t值;HDL-C=高密度脂蛋白胆固醇,LDL-C=低密度脂蛋白胆固醇,TG=三酰甘油,TC=总胆固醇,eGFR=估算肾小球滤过率
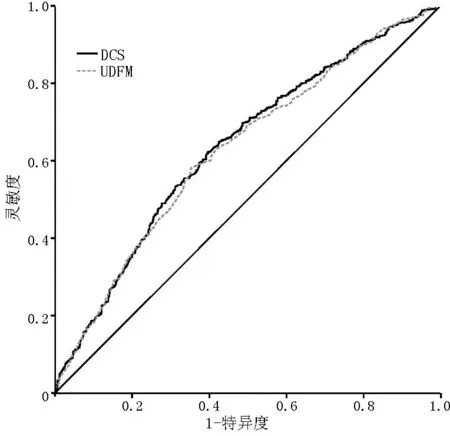
注:UDFM=更新的Diamond-Forrester法,DCS=Duke临床评分
图1UDFM和DCS诊断冠心病的ROC曲线
Figure 1ROC curve of the diagnosis of coronary artery disease by UDFM and DCS
表3不同年龄、性别的典型心绞痛患者UDFM和DCS计算的PTP与实际阳性率(%)
Table 3PTP of UDFM,DCS and actual positive rate of coronary artery disease of patients with typical angina of different ages and genders

年龄(岁)男性UDFM DCS 实际阳性率 女性UDFM DCS 实际阳性率 30~3957.266.055.625.753.3-40~4966.682.047.135.039.764.350~5975.090.071.444.156.738.860~6981.294.668.952.768.156.270~7986.096.669.161.378.169.5
注:-表示例数≤5
表4不同年龄、性别的不典型心绞痛患者UDFM和DCS计算的PTP与实际阳性率(%)
Table 4PTP of UDFM,DCS and actual positive rate of coronary artery disease of patients with atypical angina of different ages and genders

年龄(岁)男性UDFM DCS 实际阳性率 女性UDFM DCS 实际阳性率 30~3928.330.3-00-40~4936.051.143.513.213.418.250~5945.061.943.917.920.935.960~6954.176.666.224.030.867.5
注:-表示例数≤5
3讨论
CAG作为诊断冠心病的金标准,其诊断阳性率仅为20%~70%[10-11]。DOUGLAS等[10]发现影响医院CAG阳性率的主要因素在于术前患者选择以及合适的术前评估策略。近年来英国国立健康与临床优化研究所(NICE)、欧洲心脏病学会(ESC)等指南开始提出用PTP对可疑冠心病患者进行评估,为进一步决策提供参考,目前应用最为广泛的是UDFM、DCS模型。本研究结果显示,UDFM、DCS对可疑冠心病患者的筛选有一定的作用,但评估准确性的高低存在性别差异。其中UDFM、DCS对女性患者均存在低估现象,UDFM对于男性患者PTP的估算有相对较高的准确性,而DCS对男性存在高估现象。
表5不同年龄、性别的非心绞痛型胸痛患者UDFM和DCS计算的PTP与实际阳性率(%)
Table 5PTP of UDFM,DCS and actual positive rate of coronary artery disease of patients with non-angina chest pain of different ages and genders
年龄(岁)男性UDFM DCS 实际阳性率 女性UDFM DCS 实际阳性率 30~3916.736.6-5.310.7-40~4923.052.536.77.411.0-50~5930.666.336.710.624.136.860~6938.376.141.214.233.642.570~7948.085.160.119.538.658.8
注:-表示例数≤5
GENDERS等[5,12]通过纳入多个欧美研究中心胸痛患者的数据进行分析发现,UDFM、DCS预测模型的AUC分别达0.82和0.78。且在临床实践中有研究表明,如果严格应用UDFM和DCS进行PTP评估以选择进行CAG的患者,至少可以避免2/3的患者进行不必要的心脏检查[13]。而在亚洲人群中的研究却发现,这两种模型的预测效果并不佳,如FUJIMOTO等[14]、ISMA′EEL等[15]研究表明,在日本和中东地区的可疑冠心病人群中UDFM、DCS的AUC均<0.7。本研究结果亦表明,UDFM、DCS的预测效果在我国人群中不佳,其AUC分别仅为0.64、0.63,其原因可能是由于危险因素的分布差异以及研究人群之间的异质性所致。我国学者周伽等[16]在评价DCS、UDFM与CT冠状动脉造影(CTCA)联合应用对稳定型心绞痛患者的诊断准确性时,发现DCS比UDFM更适用于可疑冠心病患者PTP的估算,按照DCS估算的PTP与CTCA联合应用能够有效提高CTCA诊断准确性,并避免过度检查。本研究发现UDFM与DCS预测模型在对PTP进行估算时,DCS可以将更多的阳性患者分入高PTP组,但DEMIR等[17]直接对DCS与UDFM比较发现,DCS较UDFM对可疑冠心病患者存在明显过高估计,其适用性不及UDFM。这种差异存在的原因可能与研究人群和样本量限制有一定关系,需要进一步的研究进行验证。但若单从临床应用的便利性角度来讲,可能纳入研究变量更少的UDFM更易被临床医生所接受。
本研究发现,以CAG为金标准,UDFM对男性患者PTP的估算具有较高的准确性,对女性患者存在明显低估现象。而在另一些研究中,UDFM却被认为会过高估计PTP,在女性患者中尤甚[5]。其原因可能是由于研究人群之间存在差异以及模型本身存在的局限性。UDFM主要采用患者的性别、年龄、胸痛3个变量来预测冠心病发生的概率[17],而有部分患者,虽然存在明显冠状动脉狭窄,但并没有任何胸痛的临床症状[18]。此外,根据以往研究表明,不同性别之间发生冠心病的危险因素存在一定的差异,女性因胸痛而行CAG的诊断阳性率要比男性低[19],而UDFM却并没有考虑这些因素。RADEMAKER等[20]将女性特有的危险因素如雌激素水平、妊娠期糖尿病纳入UDFM时,其AUC可以从原来的0.61提高到0.71(P<0.001),这意味着应该对女性患者纳入更多的特有危险因素来构建模型,仅纳入3个变量对所有患者进行PTP的估算可能并不准确。
本研究的局限性:(1)本研究是单中心回顾性研究,可能存在选择偏倚。因此,下一步应当进行多中心、前瞻性和大样本量的研究以获得更有说服力的结论。(2)冠状动脉狭窄程度仅通过肉眼观察来判定,诊断结果存在观察者间的差异。(3)患者胸痛特征由医师根据病历记录人工确定,可能存在判断偏倚。
总而言之,UDFM、DCS对于我国可疑冠心病患者的评估准确性不佳,而且存在性别差异,对女性存在明显低估现象。因此,对于PTP评估模型的使用,应当注意根据研究人群的临床特点进行谨慎选择。
作者贡献:贺婷进行试验设计与实施、资料收集整理、撰写论文、成文并对文章负责;刘星、李莹、吴俏玉、罗爱静进行试验实施、评估、资料收集;袁洪进行质量控制及审校。
本文无利益冲突。
参考文献
[1]PATEL M R,PETERSON E D,DAI D,et al.Low diagnostic yield of elective coronary angiography[J].N Engl J Med,2010,362(10):886-895.
[2]SKINNER J S,SMEETH L,KENDALL J M,et al.NICE guidance.Chest pain of recent onset:assessment and diagnosis of recent onset chest pain or discomfort of suspected cardiac origin[J].Heart,2010,96(12):974-978.
[3]Task Force Members,MONTALESCOT G,SECHTEM U,et al.2013 ESC guidelines on the management of stable coronary artery disease:the Task Force on the management of stable coronary artery disease of the European Society of Cardiology[J].Eur Heart J,2013,34(38):2949-3003.
[4]FIHN S D,GARDIN J M,ABRAMS J,et al.2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the diagnosis and management of patients with stable ischemic heart disease:a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines,and the American College of Physicians,American Association for Thoracic Surgery,Preventive Cardiovascular Nurses Association,Society for Cardiovascular Angiography and Interventions,and Society of Thoracic Surgeons[J].J Am Coll Cardiol,2012,60(24):e44-164.
[5]GENDERS T S,STEYERBERG E W,ALKADHI H,et al.A clinical prediction rule for the diagnosis of coronary artery disease:validation,updating,and extension[J].Eur Heart J,2011,32(11):1316-1330.
[6]PRYOR D B,SHAW L,MCCANTS C B,et al.Value of the history and physical in identifying patients at increased risk for coronary artery disease[J].Ann Intern Med,1993,118(2):81-90.
[7]TAN Y Y,GAST G C,VAN DER SCHOUW Y T.Gender differences in risk factors for coronary heart disease[J].Maturitas,2010,65(2):149-160.
[8]MAAS A H,APPELMAN Y E.Gender differences in coronary heart disease[J].Neth Heart J,2010,18(12):598-602.
[9]WEINTRAUB W S,KARLSBERG R P,TCHENG J E,et al.ACCF/AHA 2011 key data elements and definitions of a base cardiovascular vocabulary for electronic health records:a report of the American College of Cardiology Foundation/American Heart Association Task Force on Clinical Data Standards[J].J Am Coll Cardiol,2011,58(2):202-222.
[10]DOUGLAS P S,PATEL M R,BAILEY S R,et al.Hospital variability in the rate of finding obstructive coronary artery disease at elective,diagnostic coronary angiography[J].J Am Coll Cardiol,2011,58(8):801-809.
[11]COSTA FILHO F F,CHAVESJ,LIGABL T,et al.Efficacy of patient selection for diagnostic coronary angiography in suspected coronary artery disease[J].Arq Bras Cardiol,2015,105(5):466-471.
[12]GENDERS T S,STEYERBERG E W,HUNINK M G,et al.Prediction model to estimate presence of coronary artery disease:retrospective pooled analysis of existing cohorts[J].BMJ,2012,344:e3485.
[13]PATTERSON C M,NAIR A,AHMED N,et al.Clinical outcomes when applying NICE guidance for the investigation of recent-onset chest pain to a rapid-access chest pain clinic population[J].Heart,2015,101(2):113-118.
[14]FUJIMOTO S,KONDO T,YAMAMOTO H,et al.Development of new risk score for pre-test probability of obstructive coronary artery disease based on coronary CT angiography[J].Heart Vessels,2015,30(5):563-571.
[15]ISMA′EEL H A,SERHAN M,SAKR G E,et al.Diamond-Forrester and Morise risk models perform poorly in predicting obstructive coronary disease in Middle Eastern Cohort[J].Int J Cardiol,2016,203:803-805.
[16]周伽,杨俊杰,周迎,等.验前概率联合冠脉CT造影对于稳定型冠心病的诊断价值[J].解放军医学院学报,2015,36(4):313-317.
ZHOU J,YANG J J,ZHOU Y,et al.Diagnostic accuracy of pre-test probability combined with computed tomographic coronary angiography in patients suspected for stable coronary artery disease[J].Academic Journal of Chinese Pla Medical School,2015,36(4):313-317.
[17]DEMIR O M,DOBSON P,PAPAMICHAEL N D,et al.Comparison of ESC and NICE guidelines for patients with suspected coronary artery disease:evaluation of the pre-test probability risk scores in clinical practice[J].Clin Med(Lond),2015,15(3):234-238.
[18]ROVAI D,NEGLIA D,LORENZONI V,et al.Limitations of chest pain categorization models to predict coronary artery disease[J].Am J Cardiol,2015,116(4):504-507.
[19]SUESSENBACHER A,WANITSCHEK M,DÖRLER J,et al.Sex differences in independent factors associated with coronary artery disease[J].Wien Klin Wochenschr,2014,126(21/22):718-726.
[20]RADEMAKER A A,DANAD I,GROOTHUIS J G,et al.Comparison of different cardiac risk scores for coronary artery disease in symptomatic women:do female-specific risk factors matter?[J].Eur J Prev Cardiol,2014,21(11):1443-1450.
(本文编辑:贾萌萌)
Diagnostic Value of Updated Diamond-Forrester Method and Duck Clinical Score Prediction Model in Patients With Suspected Coronary Artery Disease
HETing,LIUXing,LIYing,etal.
TheThirdXiangyaHospitalofCentralSouthUniversity,Changsha410013,China
【Abstract】ObjectiveTo compare the evaluation accuracy of the two prediction models——updated Diamond-Forrester method(UDFM)and Duke clinical score(DCS)for patients with suspected coronary artery disease in China,and further analyze their accuracy differences between different genders.Methods1 311 patients who had underwent CAG surgery because of chest pain in the Department of Cardiology of the Third Xiangya Hospital of Central South University from January 2010 to May 2015 were enrolled in this study.UDFM and DCS were employed to estimate the pretest probability(PTP)of the patients respectively,and PTP was divided into three groups,which were low PTP(<30%),medium PTP(30%-70%)and high PTP(>70%)groups;patients in the high PTP group were taken as having coronary artery disease.Taking CAG as the golden standard,we analyzed the diagnostic accuracy of UDFM and DCS in patients with suspected coronary artery disease in China,and further analyzed the accuracy differences of these two models between different genders.ResultsOf the 1 311 patients,CAG result displayed that 739(56.37%)cases were confirmed as coronary artery disease.UDFM result showed that 294(22.43%),673(51.33%)and 344(26.24%)cases were grouped into low PTP,medium PTP and high PTP respectively;DCS result demonstrated that 165(12.59%),403(30.74%)and 743(56.67%)cases fell into the groups of low PTP,medium PTP and high PTP.The two PTP distribution comparisons showed significant difference(χ2=379.00,P<0.001).Of the confirmed 739 cases,UDFM brought 125(16.91%),372(50.34%)and 242(32.75%) cases into the low PTP,medium PTP and high PTP groups,while 64(8.66%),189(25.58%)and 486(65.76%) were classified into the groups of low PTP,medium PTP and high PTP by DCS,and the PTP distribution comparison of the confirmed patients of the two showed significant difference(χ2=257.00,P<0.001).Under the CAG golden standard,the diagnostic sensitivity,specificity and the accuracy rate of UDFM in coronary artery disease were 32.8%,82.2% and 54.3% respectively,and the areas under the curve of ROC was 0.64〔95%CI(0.61,0.67)〕;the diagnostic sensitivity,specificity and the accuracy rate of DCS in coronary artery disease were 65.8%,55.1% and 61.1% respectively,and the area under the curve of ROC was 0.63〔95%CI(0.60,0.66)〕.There was no significant difference in the areas under the curve of their ROC(Z=0.33,P>0.05).The calculated PTP of UDFM for male patients with typical angina,patients with atypical angina,and patients with non-anginal chest pain were closer to the actual positive rate,while for female patients,besides the overestimation in the typical angina patients under the age of 50-59,the rest were all underestimated;DCS overestimated the male patients,for the female patients,besides the overestimated phenomenon in typical angina patients,the other were all in underestimation state.ConclusionThe diagnostic accuracy of UDFM and DCS for patients with suspected coronary artery disease in China is not high,moreover there are gender differences.The two both have the underestimation phenomenon in female patients,which is different from European and American.Therefore,a more accurate model based on different genders is needed to be established for the PTP estimation of patients with suspected coronary artery disease in China.
【Key words】Coronary artery disease;Pretest probability;Coronary angiography;Diagnosis;Sensitivity;Specificity;Updated Diamond-Forrester method;Duke clinical score
基金项目:国家“重大新药创制”科技重大专项(2012ZX09303014001);中南大学湘雅大数据;湖南省科技计划国际合作重点项目(2014W2034)
通信作者:袁洪,410013湖南省长沙市,中南大学湘雅三医院;E-mail:yuanhongxy3@163.com
【中图分类号】R 541.4
【文献标识码】A
DOI:10.3969/j.issn.1007-9572.2016.20.017
(收稿日期:2015-12-08;修回日期:2016-04-01)
·方法学研究·
