颈椎间盘置换与融合治疗退变性颈椎间盘疾病的Meta分析
2016-05-10石青鹏朱永林滨州医学院烟台附属医院骨科山东烟台264110
石青鹏,朱永林(滨州医学院烟台附属医院骨科,山东烟台 264110)
颈椎间盘置换与融合治疗退变性颈椎间盘疾病的Meta分析
石青鹏,朱永林
(滨州医学院烟台附属医院骨科,山东烟台264110)
摘要:目的系统性评价颈椎间盘置换与颈椎间盘摘除和融合治疗单节段退变性颈椎间盘疾病的效果。方法计算机检索PubMed、Cochrane Library、Ovid、SpringerLink、中国生物医学文献数据库、万方、维普等数据库,手工检索相关杂志及纳入研究的参考文献,制定纳入和排除标准,用RevMan 5.1软件对效应量进行Meta分析。结果共纳入8篇文献,Meta分析结果显示:两组在SF-36评分(MD=0.98,95%CI:-0.33~-2.29,Z=1.46,P=0.14)、并发症(OR =0.60,95%CI:0.34~1.04,Z=0.93,P=0.07)及再次手术率(OR=0.52,95%CI:0.26~1.05,Z=1.83,P=0.07)方面差异无统计学意义;在颈椎残障功能指数(neck disability index,NDI)评分(MD=-2.74,95%CI:-4.57~-0.91,Z =2.93,P=0.003)、颈痛视觉模拟评分(visual analogue scale,VAS)(MD=-2.84,95%CI:-4.85~-0.84,Z=2.78,P=0.005)及上肢疼痛VAS(MD=-1.84,95%CI:-3.07~-0.61,Z=2.92,P=0.003)上有统计学意义。结论在治疗单节段退变性颈椎间盘疾病中,融合组在疼痛症状和颈部功能方面的疗效差于置换组,在并发症、再次手术率、SF-36方面无明显区别,此结论仍需要大样本多中心高质量的随机对照试验进一步证实。
关键词:颈椎间盘置换;融合;Meta分析
颈椎间盘退变性疾病是骨科的常见病,对于保守治疗无效的患者采取手术治疗。颈前路椎间盘摘除和融合(anterior cervical discectomy and fusion,ACDF)因为能够缓解疼痛和改善神经功能得到了广泛应用;颈椎间盘置换(cervical disc arthroplasty,CDA)因为保留了颈椎的运动功能单位,在理论上有更好的临床疗效而日益受到重视。许多研究[1-12]对两种术式在许多方面进行了比较,但结论却不甚统一,甚至相反的结论。为了获得最佳的循证医学证据,指导临床工作,本Meta分析对颈椎间盘置换与融合治疗单节段退变性颈椎间盘疾病在几个方面进行了比较。
1资料与方法
1.1纳入标准a)研究类型:多中心研究的随机对照试验(randomized controlled trials,RCT);b)研究对象:年满18岁,对保守治疗无效的单节段退变性颈椎间盘疾病患者;c)干预措施:试验组为CDA组,采用前路椎间盘摘除、减压和椎间盘置换,对照组为ACDF组,采用前路椎间盘摘除、减压、自体骨移植和内固定。其余治疗相同;d)评价指标:纳入的研究至少包括本分析评价指标中的一项,并提供全面的数据。
排除标准:a)骨折、感染、肿瘤、骨质疏松、代谢性疾病等疾病;b)随访时间小于24个月;c)颈椎前路手术史。
1.2文献检索及筛选计算机检索PubMed、Cochrane Library、Ovid、SpringerLink、中国生物医学文献数据库、万方数据库、维普数据库等国内外数据库,检索时间为建库至2013 年9月,不限制检索语言[13]。英文检索词为“degenerative cervical disc disease”、“cervical disc arthroplasty”和“anterior cervical discectomy and fusion”,中文检索词为退变性颈椎间盘疾病、颈椎间盘置换、颈椎前路减压和融合,均用布尔逻辑运算符(and和or)连接,搜索词在不同数据库之间做适当修改。手工检索《中华医学杂志》、《中华外科杂志》、《中华骨科杂志》、《中国脊柱脊髓杂志》、《中国骨与关节损伤杂志》等相关杂志,同时对纳入研究的参考文献和未发表的文献(灰色文献)、会议记录等进行查阅,如有必要与有关作者联系。由2名评价者独立阅读题目、摘要,按制定的纳入和排除标准进行筛选,任何可能纳入的文献均阅读全文,如对文献的选择和评价发生分歧,可通过讨论协商解决或第三方(通讯作者)仲裁决定。
1.3评价指标的提取由2名评价者对纳入的文献提取以下评价指标:a)颈部功能障碍指数(neck disability index,NDI);b)颈部和根性疼痛的视觉模拟评分法(visual analogue scale,VAS);c)健康调查量表(SF-36)评分;d)手术节段和邻近节段的再次手术率;e)并发症。各项评价指标均是2年随访时的结果。
1.4方法学质量评估由2名评价者参考Cochrane系统评价手册中的干预性治疗措施评估工具[14]对纳入的9篇文献进行方法学质量评价,从5个方面7个条目进行评价,对每一个条目均采用“低度偏倚风险”“偏倚风险不确定”及“高度偏倚风险”进行评价,如所有条目均为低度偏倚风险,则认为此研究的方法学质量高(A级);任何一个或多个条目为偏倚风险不确定,则认为此研究质量中等(B级);任何一个或多个条目为高度偏倚风险,则认为此研究质量低(C级)。
1.5统计学方法使用Cochrane协作网提供的Revman 5.1软件对提取的评价指标做Meta分析。采用χ2检验评价结果的异质性,参考Cochrane系统评价手册,当I2>40%,通过敏感性分析能够排除异质性时,选用固定效应模型,反之,则选用随机效应模型;当I2≤40%,选用固定效应模型进行分析[15]。定性资料的效应量采用优势比(odds ratio,OR)及95%置信区间(confidence interval,CI);定量资料的效应量采用均数差(mean difference,MD)及其95%CI。
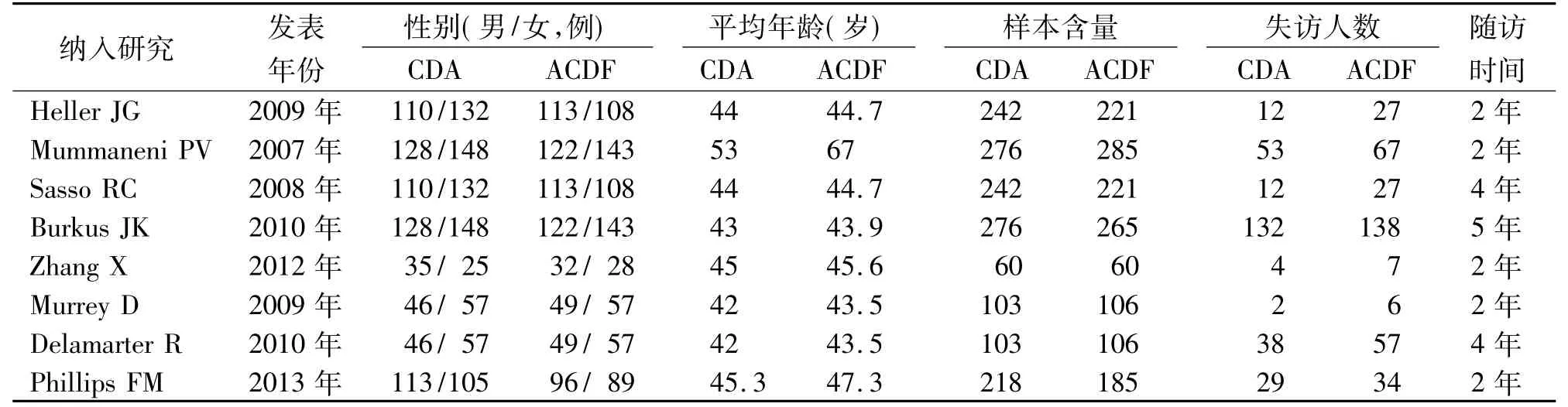
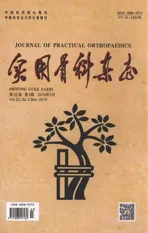
表1 纳入研究的基本特征
2结 果
2.1检索结果及质量评价结果共检索出652篇文献,通过剔除重复文献、阅读题目、摘要及全文,最终纳入8篇文献[2-9]。纳入研究的基本特征见表1,方法学的质量评价见表2。
2.2 Meta分析结果
2.2.1颈部功能障碍指数(NDI)有5篇研究[2,3,6,7,9]报告了术后2年的NDI,对纳入的研究进行异质性检验,结果显示明显异质性(I2=87%),进行敏感性分析,将1篇文献[9]排除后,异质性消失(I2=0),采用固定效应模型进行Meta分析(见图1)。结果显示:(MD=-2.74,95%CI:-4.57~-0.91,Z=2.93,P=0.003),两组在NDI方面差异有统计学意义(P<0.05),CDA组优于ACDF组。
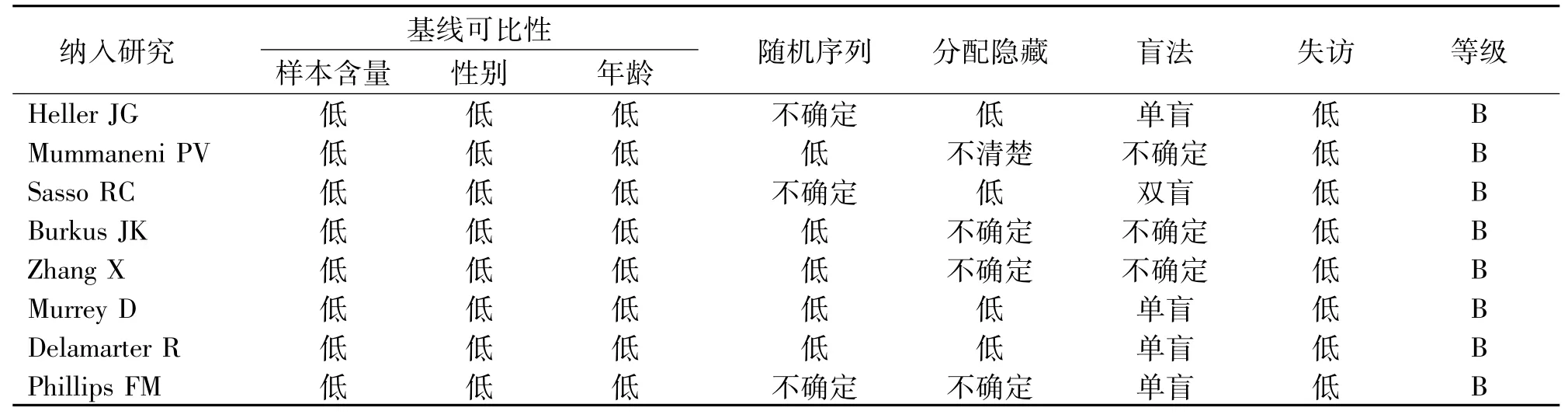
表2 纳入研究的方法学评估
图1 CDA组和ACDF组的颈部功能障碍指数比较
2.2.2颈痛VAS有2篇研究[6,9]报告了术后2年的颈痛VAS,对纳入的研究进行异质性检验,结果显示明显异质性(I2=64%),未发现异质性来源,采用随机效应模式进行Meta分析(见图2)。结果显示:(MD=-2.84,95%CI:-4.85~-0.84,Z=2.78,P=0.005),两组在颈痛VAS方面差异有统计学意义(P<0.05),CDA组优于ACDF组。

图2 CDA组和ACDF组的颈痛VAS比较
2.2.3上肢痛VAS有2篇研究[6,9]报告了术后2年的上肢痛VAS,对纳入的研究进行异质性检验,结果显示明显异质性(I2=41%),未发现异质性来源,采用随机效应模式进行Meta分析(见图3)。结果显示:(MD=-1.84,95%CI: -3.07~-0.61,Z=2.92,P=0.003),两组在上肢痛VAS方面差异有统计学意义(P<0.05),CDA组优于ACDF组。
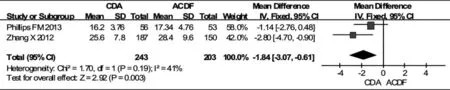
图3 CDA组和ACDF组的上肢痛VAS比较
2.2.4SF-36评分有3篇研究[2,3,9]报告了术后2年的SF-36评分,对纳入的研究进行异质性检验,结果显示无异质性(I2=0),采用固定效应模式进行Meta分析(见图4)。结果显示:(MD=0.98,95%CI:-0.33~-2.29,Z=1.46,P= 0.14),两组在SF-36评分方面差异无统计学意义(P>0.05)。

图4 CDA组和ACDF组的SF-36比较
2.2.5并发症有4篇研究[2,3,7,9]报告了并发症,对纳入的研究进行异质性检验,结果显示明显异质性(I2=29%),进行敏感性分析,将1篇文献[6]排除后,异质性消失(I2= 0),采用固定效应模型进行Meta分析(见图5)。两组在并发症方面差异无统计学意义(OR=0.60,95%CI:0.34~1.04,Z=0.93,P=0.07)。
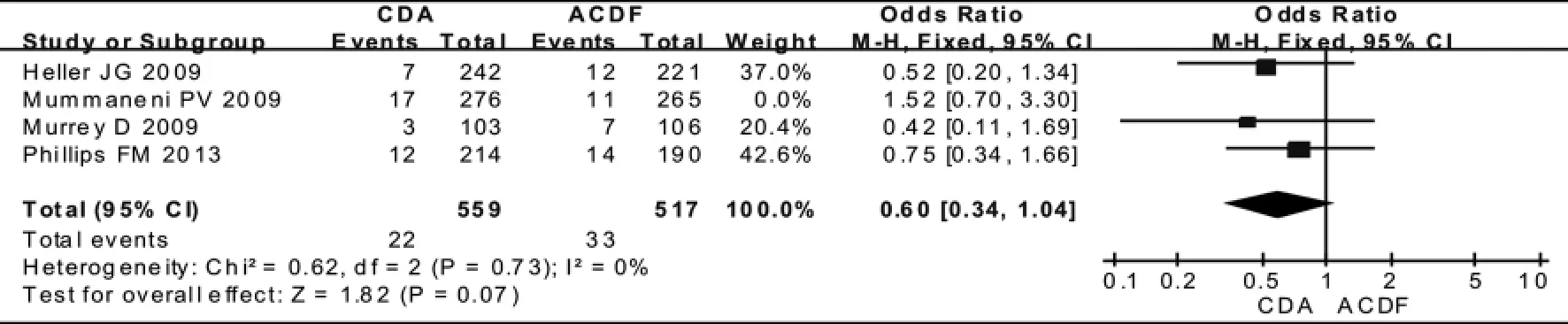
图5 CDA组和ACDF组的并发症比较
2.2.6再次手术率有4篇研究[4,5,8,9]报告了再次手术率,对纳入的研究进行异质性检验,结果显示明显异质性(I2=68%),通过敏感性分析未发现异质性来源,采用随机效应模型进行Meta分析(见图6)。两组在再次手术率方面的差异无统计学意义(OR=0.52,95%CI:0.26~1.05,Z=1.83,P =0.07)。
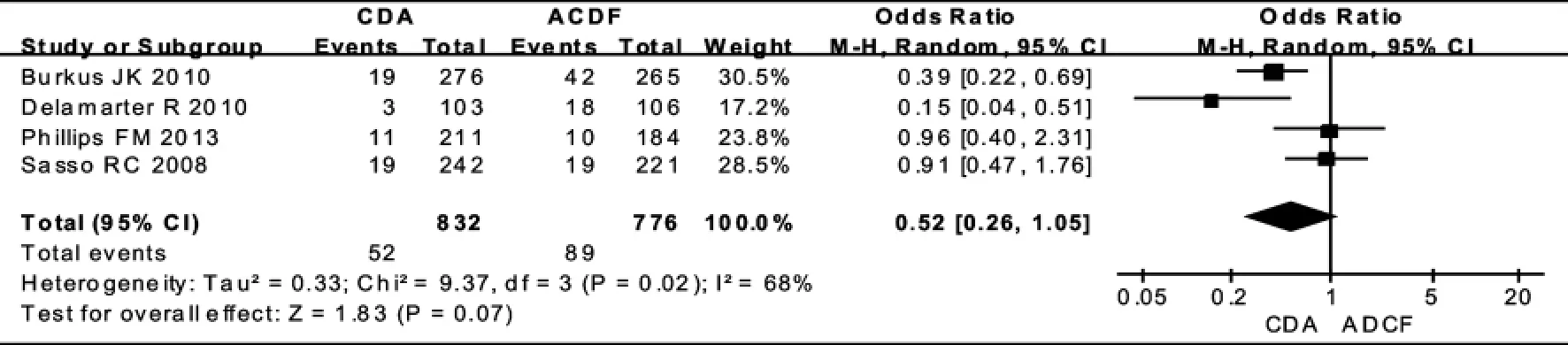
图6 CDA组和ACDF组的再次手术率比较
3讨 论
颈前路椎间盘摘除和融合(anterior cervical discectomy and fusion,ACDF)因为能够明显缓解疼痛和改善神经功能[10,16],已经成为治疗退变性颈椎间盘疾病的标准手术方式,但此术式因为融合了致病节段可能引起了邻近节段的加速退变和生物力学的失稳[17,18],最终导致疼痛症状和神经功能障碍,同时因为骨不连、植骨塌陷造成的翻修率也较高[19]。颈椎间盘置换(cervical disc arthroplasty,CDA)保留了致病节段的运动功能单位,但同时也存在生物兼容性[20]、假体的移位和塌陷[21]、异位骨化的高发生率[22]等问题。有研究[2,8,11]认为CDA有更好的症状和神经功能的改善以及延缓了邻近节段的退变,有些研究则认为两者没有区别[12,23]。两种术式的优劣仍存在很大的分歧。故本文对CDA和ACDF治疗单节段退变性颈椎间盘疾病的疗效进行比较,借以明确哪种术式更具有优势,结果显示两组在SF-36评分(P=0.14)、并发症(P=0.07)及再次手术率(P=0.07)方面差异无统计学意义;在NDI评分(P=0.003)、颈部疼痛VAS(P=0.005)及上肢疼痛VAS(P=0.003)上差异有统计学意义。
与CDA相比较,在2年随访时行ACDF的患者NDI和VAS评分明显较低,ACDF在疼痛症状和颈部功能障碍方面具有明显优势,但有研究[4,24]报道了CDA在疼痛症状和颈部功能障碍方面有优势。两组在并发症方面没有统计学意义,CDA和ACDF的并发症发生率分别为3.93%(22/559) 和6.8%(33/517),CDA的并发症主要是异位骨化、假体的移位和磨损、节段性后凸、吞咽障碍等,ACDF的并发症主要是假关节的形成、供骨区的疼痛、吞咽障碍等;有学者[25]对其中的吞咽障碍并发症进行了单独研究,结果显示ACDF有较高的吞咽障碍并发症,可能与前路内固定的使用和软组织的解剖有关。在理论上,CDA恢复了致病节段的椎间隙高度、保留了颈椎的运动功能单位及降低了邻近椎间盘的压力负荷,防止或延缓了邻近节段的退变,那么邻近节段和手术节段的再次手术率应该低于ACDF,但本Meta分析的结果显示两者并没有明显区别,可能与随访时间较短有关。此外,SF-36评分也没有明显差异,说明在患者的日常活动和健康自我评价中,两种术式疗效无明显区别。
随机对照试验被视为评价干预措施效果的最佳证据来源[26],所以本Meta仅纳入了多中心研究的RCT类文献;本文也存在某些不足:首先,各个研究在随机序列的产生、分配隐藏、盲法及失访的意向性分析等科研设计方面存在相应的缺陷,纳入的研究在方法学上均为中等质量,因此可能存在各类偏倚[27]。第二,大多数纳入的研究是由医疗器械商提供赞助完成的,尽管有严格的监督,可能是一个偏倚的潜在来源。第三,纳入的研究使用了不同的颈椎间盘假体类型,受纳入文献的限制,未进行亚组分析。最后,本文仅对2年随访时的中期部分疗效进行了评价,未对所有疗效和长期随访评价,可能得出甚至相反的结论。
综上所述,在治疗单节段颈椎间盘退变性疾病的2年随访疗效比较中,CDA在颈部和根性疼痛VAS、NDI方面优于ACDF,在并发症、再次手术率、SF-36评分方面无明显区别,但此结论仍需要大样本多中心高质量的RCT进一步证实。
参考文献:
[1]Zigler JE,Delamarter R,Murrey D,et al.ProDisc-C and anterior cervical discectomy and fusion as surgical treatment for single-level cervical symptomatic degenerative disc disease:five-year results of a Food and Drug Administration study[J].SpineSpine(Phila Pa 1976),2013,38(3):203-209.
[2]Heller JG,Sasso RC,Papadopoulos SM,et al.Comparison of Bryan cervical disc arthroplastywith anterior cervical decompression and fusion:clinical and radiographic results of a randomized,controlled,clinical trial[J].Spine,2009,34(2):101-107.
[3]Mummaneni PV,Burkus JK,Haid RW,et al.Clinical and radiographic analysis of cervical disc arthroplasty compared with allograft fusion:a randomized controlled clinical trial[J].JNeurosurg Spine,2007,6(3):198-209.
[4]Sasso RC,Best NM,Metcalf NH,et al.Motion analysis of bryan cervical disc arthroplasty versus anterior discectomy and fusion:results from a prospective,randomized,multicenter,clinical trial[J].J Spinal Disord Tech,2008,21(6):393-399.
[5]Burkus JK,Haid RW,Traynelis VC,et al.Long-term clinical and radiographic outcomes of cervical disc replacementwith the Prestige disc:results from a prospective randomized controlled clinical trial[J].JNeurosurg Spine,2010,13(3):308-318.
[6]Zhang X,Zhang X,Chen C,et al.Randomized controlled,multicenter,clinical trial comparing BRYAN cervical disc arthroplasty with anterior cervical decompression and fusion in China[J].Spine(Phila Pa 1976),2012,37(6):433-438.
[7]Murrey D,Janssen M,Delamarter R,et al.Results of the prospective,randomized,controlledmulticenter Food and Drug Administration investigational device exemption study of the ProDisc-C total disc replacement versus anterior discectomy and fusion for the treatment of 1-level symptomatic cervical disc disease[J].Spine J,2009,9(4):275-286.
[8]Delamarter R,Murrey DB,Janssen ME,et al.Results at 24 months from the prospective,randomized,multicenter Investigational Device Exemption Trial of ProDisc-C versus anterior cervical discectomy and fusion with 4-year follow-up and continued access patients[J].SAS Journal,2010,4(4):122-128.
[9]Phillips FM,Lee JY,Geisler FH.A prospective,randomized,controlled clinical investigation comparing PCM cervical disc arthroplasty with anterior cervical discectomy and fusion.2-year results from the US FDA IDE clinical trial[J].Spine(Phila Pa 1976),2013,38 (15):907-918.
[10]Chagas H,Domingues F,Aversa A,et al.Cervical spondylotic myelopathy:10 years of prospective outcome analysis of anterior decompression and fusion[J].Surg Neurol,2005,64(suppl 1):30-35.
[11]Cheng L,Nie L,Li M,et al.Superiority of the Bryan disc prosthesis for cervical myelopathy:a randomized study with 3-year follow-up[J].Clin Orthop Relat Res,2011(469):3408-3414.
[12]Nabhan A,Ishak B,Steudel WI,et al.Assessment of adjacent-segment mobility after cervical disc replacement versus fusion:RCT with 1 year's results[J].Eur Spine J,2011,20(6):934-941.
[13]Furlan AD,Pennick V,Bombardier C,et al.2009 updated method guidelines for systematic reviews in the Cochrane Back Review Group[J].Spine(Phila Pa 1976),2009,34(18):1929-1941.
[14]Higgins JP,Altman DG,Gotzsche PC,et al.The Cochrane Collaboration's tool for assessing risk of bias in randomised trials[J].BMJ,2011(343):5928.
[15]Castroflorio T,Bargellini A,Rossini G,et al.Risk factors related to sleep bruxism in children:A systematic literature review[J]Archives of oral biology,2015,60 (11):1618-1624.
[16]Landers MR,Addis KA,Longhurst JK,et al.Anterior cervical deco mpression and fusion on neck range of motion,pain,and function:a prospective analysis[J].Spine J,2013,13(6):S1529-1535.[Epub ahead of print].
[17]Hilibrand AS,Robbins M.Adjacent segment degeneration and adjacent segment disease:the consequences of spinal fusion[J].Spine J,2004,4(6 suppl):190-194.
[18]Kolstad F,Nygaard ØP,Leivseth G.Segmental motion adjacent to anterior cervical arthrodesis:a prospective study[J].Spine(Phila Pa 1976),2007,32(5):512-517.
[19]Singh K,Phillips FM,Park DK,et al.Factors affecting reoperations after anterior cervical discectomy and fusion within and outside of a Federal Drug Administration investigational device exemption cervical disc replacement trial[J].Spine J,2012,12(5):372-378.
[20]Mith HE,Wimberley DW,Vaccaro AR.Cervical arthroplasty:material properties[J].Neurosurg Focus,2004,17(3):E3.
[21]Pickett GE,Sekhon LH,SearsWR,et al.Complications with cervical arthroplasty[J].JNeurosurg Spine,2006,4(2):98-105.
[22]Chen J,Wang X,BaiW,et al.Prevalence of heterotopic ossification after cervical total disc arthroplasty:ametaanalysis[J].Eur Spine J,2012,21(4):674-680.
[23]Jawahar A,Cavanaugh DA,Kerr EJ3rd,etal.Total disc arthroplasty does not affect the incidence of adjacent segment degeneration in cervical spine:results of93 patients in three prospective randomized clinical trials [J].Spine J,2010,10(4):1043-1048.
[24]Park DK,Lin EL,Phillips FM.Index and adjacent level kinematics after cervical disc replacement and anterior fusion:in vivo quantitative radiographic analysis[J].Spine(Phila Pa 1976),2011,36(9):721-730.
[25]McAfee PC,Cappuccino A,Cunningham BW,et al.Lower incidence of dysphagia with cervical arthroplasty compared with ACDF in a prospective randomized clinical trial[J].JSpinal Disord Tech,2010,23(1):1-8.
[26]Greenhalgh T.How to read a paper.The basics of evidence based medicine[M].London:BMJBooks,2001: 9-11.
[27]Egger M,Ebrahim S,Smith GD.Where now formeta-analysis[J].Int JEpidemiol,2002,31(1):1-5.
个案
A M eta-analysis of Cervical Disc Arthrop lasty Com pared to Anterior Cervical Discectom y and Fusion for Degenerative Cervical Disc Disease
ShiQingpeng,Zhu Yonglin
(Department of Orthopaedics,1st Affiliateed Hospital,AnhuiMedical Universtiy,Hefai230032,China)
Abstract:Objective To systematically compare the outcomes of cervical disc arthroplastywith anterior cervical discectomy and fusion in the treatmentof single-level degenerative cervical disc disease.Methods The references concerning cervical disc arthroplasty and anterior cervical discectomy and fusion for the singel-level degenerative cervical disc disease were retrieved through PubMed,Cochrane Library,Ovid,SpringerLink,the China Biological Medicine Database,Wafang Database and Weipu Database,aswell as bymanually searching the related journals and literature.The eligible trialswere extracted according to the inclusion and exclusion criteria.The methodological quality of the included trials were evaluated.RevMan5.1 software was used for data analysis.Results Eight randomized controlled trials were included in the final Meta-analysis.The results of Meta-analysis showed that statistically difference between these procedures in the SF-36(MD=0.98,95%CI:-0.33~-2.29,Z=1.46,P=0.14),complications(OR=0.60,95%CI:0.34~1.04,P=0.07),reoperation rate(OR=0.52,95%CI:0.26~1.05,Z=1.83,P=0.07).There were no statistically difference in the neck disability index(MD=-2.74,95%CI:-4.57~-0.91,Z=2.93,P=0.003),neck VAS(MD=-2.84,95%CI:-4.85~-0.84,Z=2.78,P=0.005) and arm pain VAS(MD=-1.84,95%CI:-3.07~-0.61,Z=2.92,P=0.003).Conclusion In treatment of single-level degenerative cervical disc disease,cervical disc arthroplasty has better outcomes in the improvementof pain symptom and neck function,but no superiority in complications,reoperation rate and SF-36 scores.
Key words:cervical disc arthroplasty;fusion;meta-analysis
作者简介:石青鹏(1980-),男,主治医师,滨州医学院烟台附属医院骨科,264110。
收稿日期:2016-02-03
文章编号:1008-5572(2016)03-0215-06
中图分类号:R681.5+5
文献标识码:B