Enhancing endogenous stem cells in the newborn via delayed umbilical cord clamping
2015-12-15ChristopherLawtonSandraAcostaNateWatsonChiaraGonzalesPortilloTheoDiamandisNaokiTajiriYujiKanekoPaulSanbergCesarBorlongan
Christopher Lawton, Sandra Acosta, Nate Watson, Chiara Gonzales-Portillo, Theo Diamandis, Naoki Tajiri, Yuji Kaneko, Paul R. Sanberg, Cesar V. Borlongan
Center of Excellence for Aging and Brain Repair, Department of Neurosurgery and Brain Repair, University of South Florida College of Medicine, Tampa, FL, USA
Enhancing endogenous stem cells in the newborn via delayed umbilical cord clamping
Christopher Lawton, Sandra Acosta, Nate Watson, Chiara Gonzales-Portillo, Theo Diamandis, Naoki Tajiri, Yuji Kaneko, Paul R. Sanberg, Cesar V. Borlongan*
Center of Excellence for Aging and Brain Repair, Department of Neurosurgery and Brain Repair, University of South Florida College of Medicine, Tampa, FL, USA
There is currently no consensus among clinicians and scientists over the appropriate or optimal timing for umbilical cord clamping. However, many clinical studies have suggested that delayed cord clamping is associated with various neonatal benefi ts including increased blood volume, reduced need for blood transfusion, increased cerebral oxygenation in pre-term infants, and decreased frequency of iron defi ciency anemia in term infants. Human umbilical cord blood contains signifi cant amounts of stem and progenitor cells and is currently used in the treatment of several life-threatening diseases. We propose that delayed cord clamping be encouraged as it enhances blood fl ow from the placenta to the neonate, which is accompanied by an increase supply of valuable stem and progenitor cells, as well as may improve blood oxygenation and increase blood volume, altogether reducing the infant’s susceptibility to both neonatal and age-related diseases.
stem cells; umbilical cord blood; neonates; regenerative medicine
Funding: CVB is funded by NIH NINDS RO1 1R01NS071956-01, NIH NINDS 1R21NS089851-01, Department of Defense TATRC W811XWH-11-1-0634, Veterans Aff airs BX001407-01A2, James and Esther King Biomedical Research Program 09KB-01-23123, and 1KG01-33966.
Lawton C, Acosta S, Watson N, Gonzales-Portillo C, Diamandis T, Tajiri N, Kaneko Y, Sanberg PR, Borlongan CV (2015) Enhancing endogenous stem cells in the newborn via delayed umbilical cord clamping. Neural Regen Res 10(9):1359-1362.
Therapeutic Manipulation of Umbilical Cord Clamping
The timing of umbilical cord clamping, which separates the newborn from the placenta, has been the subject of much debate for decades (Mercer et al., 2001). ‘Early’ or ‘immediate’umbilical cord clamping (ICC) remains the most commonly employed method and is performed in the third stage of labor, during the period extending from complete delivery of the infant to complete delivery of the placenta (Afl aifel et al., 2012; Sheldon et al., 2013). In a recent Cochrane review (McDonald et al., 2014), early cord clamping was defined as covering a wide range from immediately following birth to less than 1 minute post-birth, whereas delayed cord clamping occurs one or more minutes after birth or when cord pulsation ceases. The benefi ts of delayed umbilical cord clamping (DCC) have been well documented and include lower risks of intraventricular hemorrhage (all grades), lower risk for necrotizing enterocolitis, increased early hemoglobin concentration, increased iron stores, and increased cerebral oxygenation in preterm infants (Baenziger et al., 2007; Rabe et al., 2012; McDonald et al., 2013). This raises the question of why early or immediate cord clamping still predominates. While some contend that the prevalence of ICC is simply because of custom, other reasons include reduced risk of post-partum hemorrhage, easier identifi cation of placental detachment, minimized risk of rhesus iso-immunization, and time constraints faced by physicians in the busy environment of the delivery room (Hutchon, 2010; Downey and Bewley, 2012). However, it is worth noting that recent studies have found no signifi cant diff erences between early versus late cord clamping groups for the primary outcome of severe postpartum hemorrhage (McDonald et al., 2014).
The benefi ts of DCC are primarily attributed to an increase in neonatal blood volume, secondary to placenta-fetal transfusion (Niermeyer and Velaphi, 2013). This transfusion has been suggested to follow an exponential decay curve with 25% being transferred within the fi rst 15 seconds, 50% by 60 seconds, and fl ow ceasing in most infants by 2–3 minutes (Yao et al., 1968, 1969; Yao and Lind, 1974). However, venous and arterial umbilical fl ow may occur for longer than previously described and placental transfusion appears to be complex and dependent on several factors (Boere et al., 2014). The transfer of umbilical cord blood is of particular interest in this review because of the various valuable stem cells contained such as hematopoietic stem cells, endothelial cell precursors, mesenchymal progenitors and multipotent/pluripotent lineage stem cells.
Stem Cells in Umbilical Cord Blood
Human umbilical cord blood (hUCB) plays a significant roleas a reservoir of stem and progenitor cells (Chen et al., 2005; Watson et al., 2015). These stem cells, which have infi nite medical potential, are currently used in the treatment of several life-threatening diseases and are viewed by many as the stem cells source of choice for clinical and non-clinical research applications (Chakraborty et al., 2014). The hematopoietic progenitor cells (HPC) of umbilical cord blood have an extensive proliferative capacity that exceeds that of bone marrow HPC (Broxmeyer et al., 1989; Ballen et al., 2013), and even a single hUCB sample can provide enough hematopoietic stem cells for both short- and long-term engraftment (Sirchia and Rebulla, 1999). While the fi rst umbilical cord blood transplant occurred 26 years ago in France in a child with Fanconi Anemia (Gluckman et al., 1989; Ballen et al., 2013), one might argue that nature’s fi rst stem cell transplant occurs at birth as the placenta and umbilical cord contract and pump blood toward the newborn (Sanberg et al., 2010; Tolosa et al., 2010). Once the blood equilibrates in both compartments, the cord becomes pulseless and blood fl ow ceases. This is the natural course in most placental mammals, yet in humans this cord blood transfusion is curtailed by early clamping of the umbilical cord, thus depriving infants of additional stem cells.
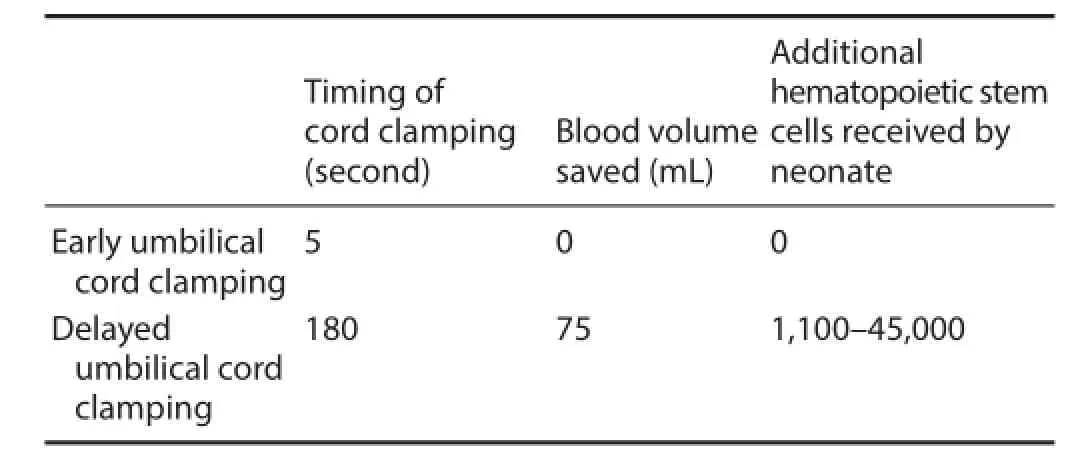
Table 1 Early versus delayed cord clamping
The existence of stem cells in fetal circulation indicates that a delay in cord clamping should increase stem cell supply to newborns. Alternatively, the artifi cial loss of stem cells at birth could potentially impact later development. The eff ects of DCC on diseases such as neonatal and adult diseases, is unknown but warrants further investigation. Of note, transplantation of exogenous hUCB has been shown to be therapeutic in animal models of cerebral palsy (Yasuhara et al., 2010), autoimmune diseases (Liu et al., 2013), acute injuries like traumatic brain injury (Acosta et al., 2014; Dela Pena et al., 2014a,b) and myocardial infarction (Acosta et al., 2013), and adult-onset disorders, such as stroke (Borlongan et al., 2004; Yu et al., 2009, 2010; Ou et al., 2010), altogether implicating that prophylactic stem cell transplantation, as may be achieved with DCC, can aff ord benefi ts against diseases in neonates and adults.
The postnatal transfer of hUCB may be particularly important in preterm infants born between 24 to 31 weeks gestation because of the higher concentration of primitive HPC and longterm culture-initiating cells when compared with cord blood of infants born closer to term (Haneline et al., 1996). Consequently, the timing of umbilical cord clamping may be especially important in preterm neonates. DCC may prove to be a safe and inexpensive practice that could potentially decrease morbidity and mortality associated with many newborn conditions, especially when there is no plan to harvest such important cells through cord blood banking.
Ideal Timing for Delayed Cord Clamping
In 2010, the International Liaison Committee on Resuscitation (ILCOR) recommended that cord clamping be delayed for at least 1 minute in healthy term infants, but stated that evidence was insuffi cient to recommend a time for clamping in those who require resuscitation (Perlman et al., 2010). Ironically, it could be argued that these infants stand to receive the greatest benefi t from DCC.
Several systematic reviews have suggested that DCC decreased incidence of intracranial hemorrhage in preterm infants (Committee on Obstetric Practice, 2012). Delaying cord clamping (for at least 30–60 seconds), with the infant maintained at or below the level of the placenta was associated with increased blood volume, reduced need for transfusion, and decreased frequency of iron defi ciency anemia in term infants (Committee on Obstetric Practice, 2012). The existence of stem cells in fetal circulation suggests that a delay in cord clamping should increase stem cell supply to the neonate, providing immediate benefi ts if neonatal disease is indicated (Table 1). In fact, if cord clamping was delayed by 180 seconds, the newborn may receive an additional 75 mL of blood volume (Yao et al., 1969; Diaz-Rossello, 2006) that could contain approximately 1,100-45,000 hematopoietic stem cells.
Some studies have even suggested that physicians delay cord clamping until ventilation (Bhatt et al., 2013), relying on the infant’s physiology rather than proceeding in a simple time-dependent fashion. Umbilical cord milking or stripping has also been put forth as a viable means of placental transfusion and been suggested to have benefi cial eff ects for newborns (Hosono et al., 2008; Rabe et al., 2011; Erickson et al., 2012; Upadhyay et al., 2013). Such milking likely increases stem cell supply to the neonate. In forming a consensus on the optimal timing for cord clamping, further investigation of the eff ects of DCC on concentrations of stem and/or progenitor cells in the newborn is essential. While DCC is likely to increase the supply of these valuable cells to the infant, it is unknown for what period of time cord clamping should be delayed for optimal benefi t to the infant.
Alternative Non-Stem Cell Mechanisms
Alternative non-stem cell mechanisms may account for some of the therapeutic eff ects of DCC. Of note, DCC has a signifi cant impact on newborn hemodynamics, mainly because of increased blood volume and improved blood oxygenation (Yigit et al., 2015). These two mechanisms may contribute to the therapeutic benefi ts rendered by DCC. For example, germinal matrix hemorrhage is known to occur with hypoxia, and DCC may protect against this hemorrhage by way of enhanced blood oxygenation and larger blood volume delivered to the baby. As previously stated, DCC is associated with less necrotizing enterocolitis and reduced incidence of intraventricular hemorrhage (Mercer et al., 2006; Aziz et al., 2012), which may be due to the increase of stem cells transferred to the baby (Sanberg et al., 2010; Tolosa et al., 2010). Likewise, DCC may improve cerebral oxygenation (Baenziger et al., 2007) and may increase blood volume (Yigit et
al., 2015), altogether reducing the incidence of intraventricular hemorrhage and necrotizing enterocolitis.
Neuroprotective Eff ects of Delayed Cord Clamping
Clinical and research-based evidence suggests that DCC may benefi t neurodevelopment and ameliorate early neurological disorders, especially in preterm neonates (McAdams, 2014). DCC’s reduction of intraventricular hemorrhage incidence (Rabe et al., 2012) is an implicated method of therapy. Abnormal neurodevelopment often spurs infant iron-defi cient anemia (Yager and Hartfi eld, 2002), and DCC is a seemingly eff ective intervention. With iron defi ciency aff ecting a substantial portion of the world’s population and approximately 25% of global births (de Benoist et al., 2008), DCC could prove a very low-cost and easy to implement treatment.
Current research also suggests that DCC provides therapeutic relief beyond the neonatal period (McDonald, 2008). Andersson et al. (2013) produced a multi-year study investigating the neurodevelopmental benefi ts of DCC at various age increments. Beginning two days after birth, infants were seen to have signifi cantly higher hemoglobin levels as well as a decrease in neonatal anemia (Andersson et al., 2015). In conjunction, data suggested more long-term relief. DCC neonates were seen to have increased scores on a series of fi ve diff erent fi ne-motor tests at 4 years of age. Such a long-term relief suggests that DCC may have a substantial impact in development. However, on the time intervals prior to the four-year mark, the data was not as promising (Andersson et al., 2015). Interestingly enough at the 12-month checkup, DCC did not have large eff ect on the iron levels or neurodevelopment in the infant population. While these sporadic improvements have been documented, more research needs to be done to demonstrate the biological cause of this phenomenon (Andersson et al., 2014).
Another anemia therapy, immediate blood transfusion, has been shown to also produce neuroprotective effects. These transfusions signifi cantly reduce early brain injury in preterm infants by altering the oxygen extraction demand within the body (Osborn, 2007). An elevated cerebral fractional tissue oxygen extraction (cFTOE) typically precedes intraventricular haemorrhage in very preterm infants (Verhagen, 2010; Balegar, 2014; Noori, 2014). The transfusion of red blood cells (RBC) balances the low blood fl ow and the high oxygen demand, eliminating the risk of hypoxia-ischaemia (Altman, 1993). Additionally, research also suggests an improvement in cardiac output and cerebral tissue in late anaemia prematurity (Andersen et al., 2015).
Conclusion
In summary, DCC can increase in neonatal blood volume, secondary to placenta-fetal transfusion. A larger blood volume may result in a higher stem cell supply to the neonate, which likely accompanies this hUCB-transfusion. Human umbilical cord blood is known to possess valuable stem and progenitor cells, which the newborn likely stands to benefi t from. Human umbilical cord blood is currently being evaluated for its effi cacy in mitigating the eff ects of various diseases and the artifi cial loss of stem cells imposed by early or immediate clamping of the umbilical cord may negatively aff ect a child’s endogenous ability to combat various diseases. In conjunction with improved oxygenation and increased blood volume, the additional stem cells delivered to the baby following DCC may aff ord therapeutic eff ects against neonatal- and adult-onset diseases.
Author contributions: CL, SA, NW, CGP, TD, NT, YK, PRS, CVB contributed to the conception of the study, review of the literature, interpretation of the studies, wrote the manuscript and provided critical revision of the manuscript for intellectual content. PRS and CVB obtained funding, and provided administrative, technical, and material support, and led the supervision of the study. All authors approved the fi nal version of this paper.
Conflicts of interest: PRS and CVB are consultants and hold patents to a number of stem cell-based biotech companies.
Acosta SA, Tajiri N, Shinozuka K, Ishikawa H, Sanberg PR, Sanchez-Ramos J, Song S, Kaneko Y, Borlongan CV (2014) Combination therapy of human umbilical cord blood cells and granulocyte colony stimulating factor reduces histopathological and motor impairments in an experimental model of chronic traumatic brain injury. PLoS One 9:e90953.
Acosta SA, Franzese N, Staples M, Weinbren NL, Babilonia M, Patel J, Merchant N, Simancas AJ, Slakter A, Caputo M, Patel M, Franyuti G, Franzblau MH, Suarez L, Gonzales-Portillo C, Diamandis T, Shinozuka K, Tajiri N, Sanberg PR, Kaneko Y, Miller LW, Borlongan CV (2013) Human umbilical cord blood for transplantation therapy in myocardial infarction. J Stem Cell Res Ther (Suppl 4) pii:S4-005.
Afl aifel N, Weeks AD (2012) Active management of the third stage of labour. BMJ 345:e45-46.
Altman DI, Perlman JM, Volpe JJ, Powers WJ (1993) Cerebral oxygen metabolism in newborns. Pediatrics 92:99-104.
Andersen CC, Karayil SM, Hodyl NA, Stark MJ (2015) Early red cell transfusion favourably alters cerebral oxygen extraction in very preterm newborns. Arch Dis Child Fetal Neonatal Ed doi:10.1136/archdischild-2014-307565.
Andersson O, Domellöf M, Andersson D, Hellström-Westas L (2013) Eff ects of delayed cord clamping on neurodevelopment and infection at four months of age: a randomised trial. Acta Paediatrica 102:525-531.
Andersson O, Domellöf M, Anderson D, Hellström-Westas D (2014) Eff ect of delayed vs early umbilical cord clamping on iron status and neurodevelopment at age 12 months: a randomized clinical trial. JAMA Pediatr 168:547-554.
Andersson O, Hellström-Westas L, Andersson D, Clausen J, Domellöf M (2013) Eff ects of delayed compared with early umbilical cord clamping on maternal postpartum hemorrhage and cord blood gas sampling: a randomized trial. Acta Obstet Gynecol Scand 92:567-574.
Andersson O, Lindquist B, Lindgren M, Stjernqvist K, Domellöf M, Hellström-Westas L (2015) Eff ect of Delayed Cord Clamping on Neurodevelopment at 4 Years of Age: A Randomized Clinical Trial. JAMA Pediatr 169:631-638.
Aziz K, Chinnery H, Lacaze-Masmonteil T (2012) A single-center experience of implementing delayed cord clamping in babies born at less than 33 weeks’ gestational age. Adv Neonatal Care 12:371-376.
Baenziger O, Stolkin F, Keel M, von Siebenthal K, Fauchere JC, Das Kundu S, Dietz V, Bucher HU, Wolf M (2007) The infl uence of the timing of cord clamping on postnatal cerebral oxygenation in preterm neonates: a randomized, controlled trial. Pediatrics 119:455-459.
Balegar KK, Stark MJ, Briggs N, Andersen CC (2014) Early cerebral oxygen extraction and the risk of death or sonographic brain injury in very preterm infants. J Pediatr 164:475-480.
Ballen KK, Gluckman E, Broxmeyer HE (2013) Umbilical cord blood transplantation: the fi rst 25 years and beyond. Blood 122:491-498.
Bhatt S, Alison BJ, Wallace EM, Crossley KJ, Gill AW, Kluckow M, te Pas AB, Morley CJ, Polglase GR, Hooper SB (2013) Delaying cord clamping until ventilation onset improves cardiovascular function at birth in preterm lambs. J Physiol 591:2113-2126.
Boere I, Roest AA, Wallace E, Ten Harkel AD, Haak MC, Morley CJ, Hooper SB, Te Pas AB (2014) Umbilical blood fl ow patterns directly after birth before delayed cord clamping. Arch Dis Child Fetal Neonatal Ed 0:F1-5.
Borlongan CV, Hadman M, Sanberg CD, Sanberg PR (2004) Central nervous system entry of peripherally injected umbilical cord blood cells is not required for neuroprotection in stroke. Stroke 35:2385-2389.
Brocklebank AM, Sparrow RL (2001) Enumeration of CD34+ cells in cord blood: a variation on a single-platform fl ow cytometric method based on the ISHAGE gating strategy. Cytometry 46:254-261.
Broxmeyer HE, Douglas GW, Hangoc G, Cooper S, Bard J, English D, Arny M, Thomas L, Boyse EA (1989) Human umbilical cord blood as a potential source of transplantable hematopoietic stem/progenitor cells. Proc Natl Acad Sci U S A 86:3828-3832.
Chakraborty SK, Banu LA, Rahman MF, Paul S (2014) Cord blood stem cells – a dream for future medicine. Mymensingh Med J 23:614-620.
Chen N, Hudson JE, Walczak P, Misiuta I, Garbuzova-Davis S, Jiang L, Sanchez-Ramos J, Sanberg PR, Zigova T, Willing AE (2005) Human umbilical cord blood progenitors: the potential of these hematopoitic cells to become neural. Stem Cells 23:1560-1570.
Committee on Obstetric Practice, American College of Obstetricians and Gynecologists (2012) Committee Opinion No.543: Timing of umbilical cord clamping after birth. Obstet Gynecol 120:1522-1526.
de Benoist B, McLean E, Egli I, Cogswell M (2008) Worldwide prevalence of anaemia 1993–2005: WHO Global Database on Anaemia. Geneva (Switzerland): World Health Organization.
De la Peña I, Sanberg PR, Acosta S, Lin SZ, Borlongan CV (2014). Umbilical cord blood cell and granulocyte-colony stimulating factor: combination therapy for traumatic brain injury. Regen Med 9:409-412.
Dela Peña I, Sanberg PR, Acosta S, Tajiri N, Lin SZ, Borlongan CV (2014) Stem cells and G-CSF for treating neuroinfl ammation in traumatic brain injury: aging as a comorbidity factor. J Neurosurg Sci 58:145-149.
Diaz-Rossello JL (2006) Cord clamping for stem cell donation: medical facts and ethics. NeoReviews 7:e557-e563.
Downey CL, Bewley S (2012) Historical perspectives on umbilical cord clamping and neonatal transition. J R Soc Med 105:325-329.
Erickson-Owens DA, Mercer JS, Oh W (2012) Umbilical cord milking in term infants delivered by cesarean section: a randomized controlled trial. J Perinatol 32:580-584.
Gluckman E, Broxmeyer HA, Auerbach AD, Friedman HS, Douglas GW, Devergie A, Esperou H, Thierry D, Socie G, Lehn P, Cooper S, English D, Kertzberg J, Bard J, Boyse E (1989) Hematopoietic reconstitution in a patient with Fanconi’s anemia by means of umbilical-cord blood from and HLA-identical sibling. N Engl J Med 321:1174-1178.
Haneline LS, Marshall KP, Clapp DW (1996) The highest concentration of primitive hematopoietic progenitor cells in cord blood is found in extremely premature infants. Pediatr Res 39:820-825.
Hosono S, Mugishima H, Fujita H, Hosono A, Minato M, Okada T, Takahashi S, Harada K (2008) Umbilical cord milking reduces the need for red cell transfusions and improves neonatal adaptation in infants born at less than 29 weeks’ gestation: a randomised controlled trial. Arch Dis Child Fetal Neonatal Ed 93:F14-F19.
Hutchon DJ (2010) Why do obstetricians and midwives still rush to clamp the cord? BMJ 341:c5447.
Liu R, Zhang Z, Lu Z, Borlongan C, Pan J, Chen J, Qian L, Liu Z, Zhu L, Zhang J, Xu Y (2013) Human umbilical cord stem cells ameliorate experimental autoimmune encephalomyelitis by regulating immunoinfl ammation and remyelination. Stem Cells Dev 22:1053-1062.
3.模型的设定。本文借鉴李越冬等(2014)研究内控重大缺陷与审计定价之间相关性的研究模型,并加入固定资产与应收类账户占总资产比例对其进行修正,构建如下模型进行研究。
McAdams RM (2014) Time to implement delayed cord clamping. Obstet Gynecol 123:549-552.
McDonald SJ, Middleton P, Dowswell T, Morris PS (2014) Eff ect of timing of umbilical cord clamping of term infants on maternal and neonatal outcomes. Evid Based Child Health 9:303-397.
McDonald SJ, Middleton P, Dowswell T, Morris PS (2013) Eff ect of timing of umbilical cord clamping of term infants on maternal and neonatal outcomes. Cochrane Database Syst Rev 7:CD004074.
Mercer JS (2001) Current best evidence: a review of the literature on umbilical cord clamping. J Midwifery Womens Health 46:402-414.
Mercer JS, Vohr BR, McGrath MM, Padbury JF, Wallach M, Oh W (2006) Delayed cord clamping in very preterm infants reduces the incidence of intraventricular hemorrhage and late-onset sepsis: a randomized, controlled trial. Pediatrics 117:1235-1242.
Niermeyer S, Velaphi S (2013) Promoting physiologic transition at birth: re-examining resuscitation and the timing of cord clamping. Semin Fetal Neonatal Med 18:385-392.
Noori S, McCoy M, Anderson MP, Ramji F, Seri I (2014) Changes in cardiac function and cerebral blood fl ow in relation to peri/intraventricular hemorrhage in extremely preterm infants. J Pediatr 164:264-270.e1-3.
Osborn DA, Evans N, Kluckow M, Bowen JR, Rieger I (2007) Low superior vena cava fl ow and eff ect of inotropes on neurodevelopment to 3 years in preterm infants. Pediatrics 120:372-380.
Perlman JM, Wyllie J, Kattwinkel DL, Atkins DL, Chameides JP, Goldsmith JP, Guinsburg R, Hazinski MF, Morley C, Richmond S, Simon WM, Singhal N, Szyld E, Tamura M, Velaphi S (2010) Part 11: Neonatal resuscitation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 122:S516-S538.
Rabe H, Diaz-Rossello JL, Duley L, Dowswell T (2012) Effect of timing of umbilical cord clamping and other strategies to infl uence placental transfusion at preterm birth on maternal and infant outcomes. Cochrane Database Syst Rev 8:CD003248.
Rabe H, Jewison A, Alvarez RF, Crook D, Stilton D, Bradley R, Holden D (2011) Milking compared with delayed cord clamping to increase placental transfusion in preterm neonates: a randomized controlled trial. Obstet Gynecol 117:205-211.
Sanberg PR, Park DH, Borlongan CV (2010) Stem cell transplants at childbirth. Stem Cell Rev 6:27-30.
Sheldon WR, Durocher J, Winikoff B, Blum J, Trussell J (2013) How eff ective are the components of active management of the third stage of labor? BMC Pregnancy Childbirth 13:46.
Sirchia G, Rebulla P (1999) Placental/umbilical cord blood transplantation. Haematologica 84:738-747.
Tolosa JN, Park DH, Eve DJ, Klasko SK, Borlongan CV, Sanberg PR (2010) Mankind’s fi rst natural stem cell transplant. J Cell Mol Med 14:488-495. Upadhyay A, Gothwal S, Parihar R, Garg A, Gupta A, Chawla D, Gulati IK (2013) Eff ect of umbilical cord milking in term and near term infants: randomized control trial. Am J Obstet Gynecol 208:120.e1-e6.
Verhagen EA, Ter Horst HJ, Keating P, Martijn A, Van Braeckel KN, Bos AF (2010) Cerebral oxygenation in preterm infants with germinal matrix-intraventricular hemorrhages. Stroke 41:2901-2907.
Watson N, Divers R, Kedar R, Mehindru A, Mehindru A, Borlongan MC, Borlongan CV (2015) Discarded Wharton jelly of the human umbilical cord: a viable source for mesenchymal stromal cells. Cytotherapy 17:18-24.
Yager JY, Hartfi eld DS (2002) Neurologic manifestations of iron defi ciency in childhood. Pediatr Neurol 27:85-92.
Yasuhara T, Hara K, Maki M, Xu L, Yu G, Ali MM, Masuda T, Yu SJ, Bae EK, Hayashi T, Matsukawa N, Kaneko Y, Kuzmin-Nichols N, Ellovitch S, Cruz EL, Klasko SK, Sanberg CD, Sanberg PR, Borlongan CV (2010) Mannitol facilitates neurotrophic factor up-regulation and behavioural recovery in neonatal hypoxic-ischaemic rats with human umbilical cord blood grafts. J Cell Mol Med 14:914-921.
Yao AC, Lind J (1974) Blood fl ow in the umbilical vessels during the third stage of labor. Biol Neonate 25:186-193.
Yao AC, Lind J (1974) Placental transfusion. Am J Dis Child 127:128-141.
Yao AC, Hirvensalo M, Lind J (1968) Placental transfusion-rate and uterine contraction. Lancet 1:380-383.
Yao AC, Moinian M, Lind J (1969) Distribution of blood between infant and placenta after birth. Lancet 2:871-873.
Yigit MB, Kowalski WJ, Hutchon DJ, Pekkan K (2015) Transition from fetal to neonatal circulation: Modeling the eff ect of umbilical cord clamping. J Biomech S0021-9290:00130-X.
Yu G, Borlongan CV, Ou Y, Stahl CE, Yu S, Bae E, Kaneko Y, Yang T, Yuan C, Fang L (2010) In vitro non-viral lipofectamine delivery of the gene for glial cell line-derived neurotrophic factor to human umbilical cord blood CD34+ cells. Brain Res 1325:147-154.
Yu G, Borlongan CV, Stahl CE, Hess DC, Ou Y, Kaneko Y, Yu SJ, Yang T, Fang L, Xie X (2009) Systemic delivery of umbilical cord blood cells for stroke therapy: a review. Restor Neurol Neurosci 27:41-54.
*Correspondence to:
Cesar V. Borlongan, Ph.D.,
cborlong@health.usf.edu.
orcid:
0000-0002-2966-9782
(Cesar V. Borlongan)
10.4103/1673-5374.165218
http://www.nrronline.org/
Accepted: 2015-06-02
猜你喜欢
杂志排行

中国神经再生研究(英文版)的其它文章
- The choline pathway as a strategy to promote central nervous system (CNS) remyelination
- Neurochemical plasticity of Müller cells after retinal injury: overexpression of GAT-3 may potentiate excitotoxicity
- Non-steroidal anti-infl ammatory drugs (NSAIDs) and neuroprotection in the elderly: a view from the mitochondria
- PTEN inhibition and axon regeneration and neural repair
- Elastic modulus aff ects the growth and diff erentiation of neural stem cells
- Neural correlates of the Heidelberg Music Therapy: indicators for the regeneration of auditory cortex in tinnitus patients?