数字化音乐胃电起搏治疗顽固性功能性消化不良重叠非糜烂性反流病的疗效观察
2015-06-28冉亚梅林玲何雨芩陈强纪雷郎秀琼黄智勇杨敏
冉亚梅,林玲,何雨芩,陈强,纪雷,郎秀琼,黄智勇,杨敏
数字化音乐胃电起搏治疗顽固性功能性消化不良重叠非糜烂性反流病的疗效观察
冉亚梅,林玲,何雨芩,陈强,纪雷,郎秀琼,黄智勇,杨敏
目的 观察数字化音乐胃电起搏治疗顽固性功能性消化不良(FD)重叠非糜烂性反流病(NERD)的临床疗效,以及其对患者心理健康状况和生活质量的影响。方法 根据罗马Ⅲ标准及胃食管反流病的蒙特利尔共识意见,选取顽固性FD重叠NERD患者50例。采用数字化音乐胃电起搏进行治疗,每日治疗1次,每次45min,15d为1疗程。应用临床症状积分评估治疗前与治疗15d后的临床疗效。采用症状自评量表-SCL90评估患者心理健康状况及生活质量。结果 与治疗前比较,治疗15d后患者上腹痛、上腹胀满、早饱、嗳气、呃逆、恶心、烧心、反酸(昼)、反酸(夜)、厌食、睡眠等11大临床症状均明显缓解,差异均有统计学意义(P<0.005),其显效率(有效率)分别为59.0%(100.0%)、59.3%(96.3%)、47.0%(94.1%)、61.3%(96.8 %)、86.7%(100.0%)、80.0%(100.0%)、64.3%(92.9%)、73.7%(89.5%)、64.3%(85.7%)、90.0%(90.0%)、36.7%(93.3%),治疗后患者症状缓解的总有效率为94.4%,总显效率为65.7%。与治疗前比较,治疗15d后患者躯体化、强迫症状、抑郁、焦虑SCL90评分明显下降,其差异有统计学意义(P<0.01)。结论 数字化音乐胃电起搏治疗顽固性FD重叠NERD有显著疗效,有望成为此类疾病治疗的新选择。
消化不良;胃食管反流;胃电起搏
功能性消化不良(functional dyspepsia,FD)与非糜烂性反流病(nonerosive reflux disease,NERD)是消化系统的常见疾病,其中FD约占消化专科门诊的20%~40%[1],NERD约占胃食管反流病(gastroesophageal reflux disease,GERD)的70%[2]。NERD中有70%的患者重叠FD[3],其发病机制亦未完全阐明[4]。迄今为止,对部分顽固性FD叠加NERD患者,临床上尚无特异、有效的治疗方法。研究表明,音乐声波按摩可改善FD患者腹痛、腹胀、嗳气、早饱、纳差、恶心呕吐等症状并能改善抑郁、焦虑等心理障碍[5];胃肠起搏可纠正胃电节律、改善胃肠动力功能[6]。本研究利用音乐及胃肠起搏的治疗原理,采用数字化音乐胃电起搏,即通过在胃起搏基波上适当叠加音乐电刺激信号来治疗顽固性FD叠加NERD,旨在为此类疾病的治疗提供一种新思路。
1 资料与方法
1.1 研究对象 根据罗马Ⅲ标准及胃食管反流病的蒙特利尔共识意见标准[7],选取我院2011年1月-2014年7月门诊顽固性FD叠加NERD患者共50例,男16例,女34例,平均年龄43.9(26~65)岁。文化水平:中专及其以上者35例,初中15例。入选标准:①FD的诊断符合罗马Ⅲ诊断标准,NERD的诊断符合胃食管反流病的蒙特利尔共识意见标准[7],有上腹痛、上腹饱胀、早饱、嗳气、呃逆、恶心、烧心、反酸等症状;②经内科常规治疗无效,症状反复发作,病程>6个月;③均经胃镜检查,排除消化道溃疡、糜烂性胃炎、萎缩性胃炎等;④有FD重叠NERD症状前无精神类疾病史且未服用精神类药物。排除标准:①妊娠和哺乳期妇女;②有肝、胆、胰、脾、肾等器官的器质性疾病及腹部手术病史;③治疗前1周停用促动力剂、抑酸剂及抗焦虑药至少1周。
1.2 数字化音乐胃电起搏治疗方案
1.2.1 刺激波形及参数 以胃起搏类正弦基波叠加超低中频不同力度的混合音乐电流为刺激波形(图1)。输出参数如下。基波频率:1.1~1.2倍胃慢波节律;刺激强度:0~21V(根据患者耐受度调节),其中音乐及基波强度根据患者自身反馈进行调节。
1.2.2 刺激电极放置部位 正极置于患者胃窦体表投影处,即剑突与脐连线中点右方2~4cm处(一般瘦小体型可取2cm,普通体型3cm,高大者取4cm);负极置于患者胃体体表投影处,即剑突与脐连线中点左方3~5cm偏上1cm处(不同体型调整方法同上);穴位刺激电极片置于双侧足三里穴位处;通过皮肤导电达到治疗作用。
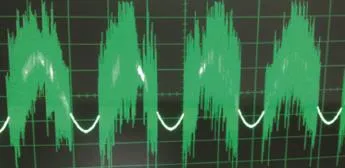
图1 音乐胃电起搏刺激波形Fig.1 Stimulation waveforms of music gastric electrical pacing
1.2.3 刺激方式 在头戴耳机聆听音乐的同时,接受电极输出的音乐胃电起搏刺激信号和原始音乐刺激信号,音乐电刺激信号适当叠加在胃起搏基波上,并激发胃肠动力相关穴位,获得胃起搏、音乐治疗、胃肠动力相关穴位刺激、神经调节等多重效果,从而达到治疗作用。
1.2.4 音乐处方及疗程 音乐处方:五行音乐,即是将中国传统医学中阴阳五行、天地人合一的理论与音乐相结合。五音即角、徵、宫、商、羽。角调为春音,属木,通于肝;徵调为夏音,属火,通于心;宫调为长夏音,属土,通于脾;商调为秋音,属金,通于肺;羽调为冬音,属水,通于肾。治疗环境安静,家属积极配合,治疗过程中观察患者有无不良反应。每日上午10:00-10:45治疗1次,每次45min,15d为1个疗程,间隔1周,可行第2疗程。
1.3 临床症状评分 按临床症状评分标准将上腹痛、上腹饱胀、早饱、嗳气、呃逆、恶心、烧心、反酸(昼)、反酸(夜)、厌食、睡眠等11项临床症状分为4级:0分为没有任何症状;1分为轻度,症状轻微,需注意才能感觉到;2分为中度,自觉症状明显,但不影响工作和生活;3分为重度,自觉症状明显,影响工作和生活。对以上症状进行评分。临床疗效评价标准如下。有效:治疗后症状较前减轻;显效:治疗后患者自觉症状完全消失或症状改善2个等级;无效:治疗后患者自觉临床症状无明显减轻或反而加重。评估显效率和有效率。显效率=显效数/总例数×100%,有效率=(有效数+显效数)/总例数×100%。对比治疗前后患者腹胀、腹痛、嗳气、反酸、早饱、厌食、烧心、恶心等临床症状的变化。
1.4 心理健康状况及生活质量评估方法 根据SCL-90症状自评量表对患者心理健康状况及生活质量进行评估。将SCL-90归纳为9个基本症状因子,各项基本症状分为1-5级。1分为自觉无该项问题;2分为自觉有该项症状,但对受试者影响轻微;3分为自觉有该项症状,对受试者有一定影响;4分为自觉有该项症状,对受试者有相当程度的影响;5分为自觉该症状的频度和强度均十分严重,严重影响受试者。对比治疗前后患者焦虑、抑郁、躯体化、强迫症状等心理状态的变化。得分高代表心理健康程度差。
1.5 统计学处理 采用SPSS 18.0软件包对数据进行处理,计量资料以±s表示,各症状组内比较采用配对t检验,P<0.05为差异有统计学意义。
2 结 果
2.1 临床症状评分及疗效比较 所有患者对数字化音乐胃电起搏治疗仪均无不良反应。患者治疗前后医生问诊症状评分及其变化情况见表1。音乐胃电起搏治疗15d后,评分均较治疗前降低,各症状明显缓解,差异均有统计学意义(P<0.005)。患者上腹痛、上腹饱胀、早饱、嗳气、呃逆、恶心、烧心、反酸(昼)、反酸(夜)、厌食、睡眠等11种症状的治疗显效率(有效率)分别为59.0%(100.0%)、59.3%(96.3%)、47.0%(94.1%)、61.3%(96.8%)、86.7%(100.0%)、80%(100%)、64.3%(92.9%)、73.7%(89.5%)、64.3%(85.7%)、90.0%(90.0%)、36.7%(93.3%),治疗后患者症状缓解的总有效率94.4 %,总显效率65.7%。
表1 数字化音乐胃电起搏治疗前后患者临床症状评分比较(±s)Tab.1 The score of clinical symptom before treatment and 15 days after treatment by using digital music gastric electrical pacing (±s)
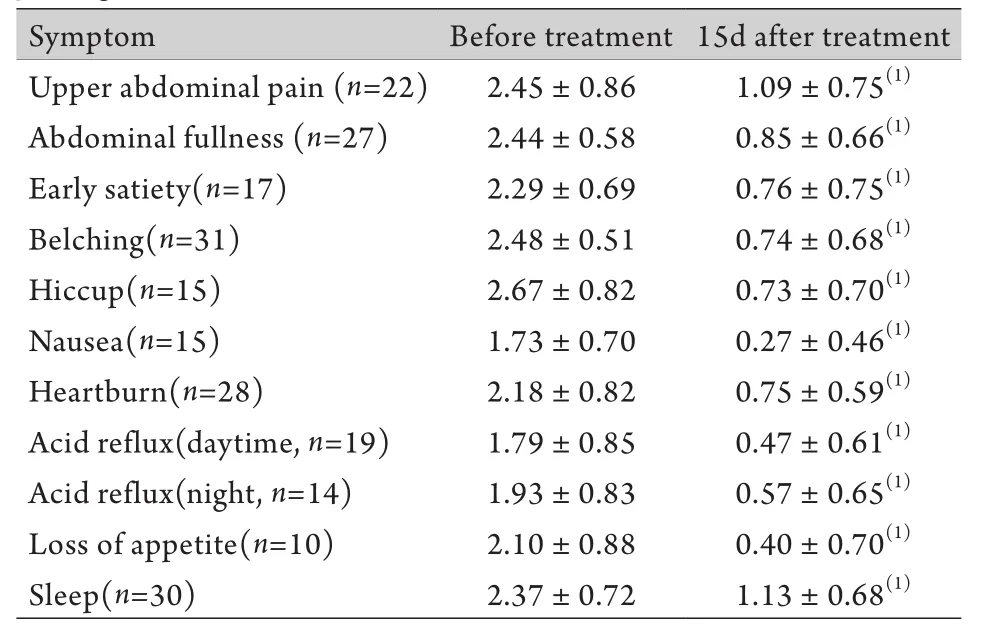
表1 数字化音乐胃电起搏治疗前后患者临床症状评分比较(±s)Tab.1 The score of clinical symptom before treatment and 15 days after treatment by using digital music gastric electrical pacing (±s)
(1)P<0.005 compared with before treatment
?
2.2 SCL-90评分比较 治疗前后患者SCL-90评分及其变化情况见表2。统计学分析结果显示,经音乐胃电起搏治疗后,患者躯体化、强迫症状、抑郁及焦虑评分明显下降,差异有统计学意义(P<0.01),而人际敏感、敌对、恐怖、偏执和精神病性评分,治疗前后差异无统计学意义(P>0.05)。
表2 数字化音乐胃电起搏治疗前后患者SCL-90评分比较(s)Tab.2 The symptom scores before and after treatment by using symptom checklist 90 (±s)
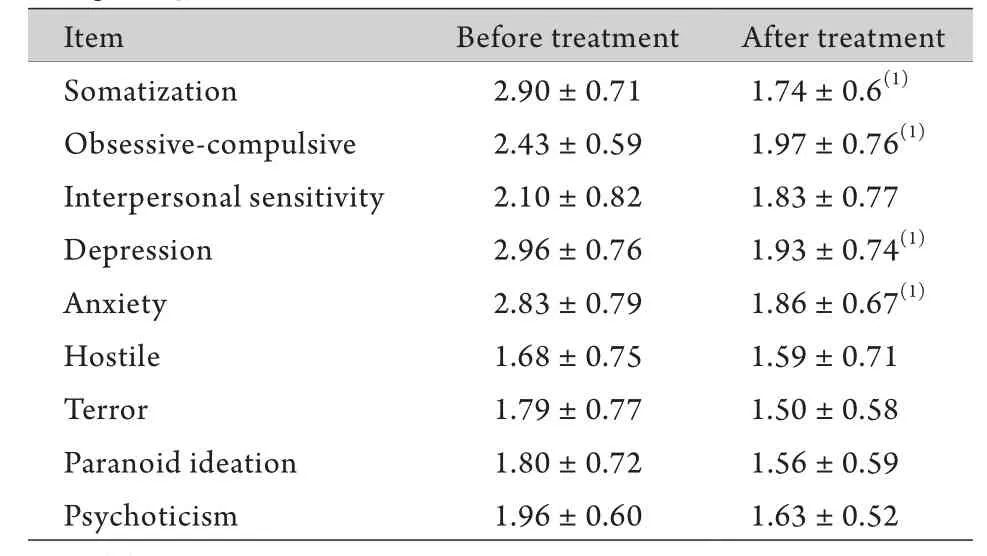
表2 数字化音乐胃电起搏治疗前后患者SCL-90评分比较(s)Tab.2 The symptom scores before and after treatment by using symptom checklist 90 (±s)
(1)P<0.01 compared with before treatment
I t e m B e f o r e t r e a t m e n t A f t e r t r e a t m e n t S o m a t i z a t i o n 2 . 9 0 ± 0 . 7 1 1 . 7 4 ± 0 . 6(1)O b s e s s i v e -c o m p u l s i v e 2 . 4 3 ± 0 . 5 9 1 . 9 7 ± 0 . 7 6(1)I n t e r p e r s o n a l s e n s i t i v i t y 2 . 1 0 ± 0 . 8 2 1 . 8 3 ± 0 . 7 7 D e p r e s s i o n 2 . 9 6 ± 0 . 7 6 1 . 9 3 ± 0 . 7 4(1)A n x i e t y 2 . 8 3 ± 0 . 7 9 1 . 8 6 ± 0 . 6 7(1)H o s t i l e 1 . 6 8 ± 0 . 7 5 1 . 5 9 ± 0 . 7 1 T e r r o r 1 . 7 9 ± 0 . 7 7 1 . 5 0 ± 0 . 5 8 P a r a n o i d i d e a t i o n 1 . 8 0 ± 0 . 7 2 1 . 5 6 ± 0 . 5 9 P s y c h o t i c i s m 1 . 9 6 ± 0 . 6 0 1 . 6 3 ± 0 . 5 2
3 讨 论
FD和NERD是消化系统的常见疾病[8],药物治疗效果不一[9-10],部分患者伴抑郁、焦虑等心理障碍,临床治疗效果较差。本研究结果表明,音乐电起搏治疗后,顽固性FD及NERD患者临床症状明显缓解,总有效率达94.4%,总显效率65.7%,且抑郁、焦虑状态也明显改善,提示音乐电起搏治疗顽固性FD及NERD疗效显著,可能会成为治疗功能性胃肠病及胃肠动力障碍性疾病的一种新方法。
数字化音乐胃电起搏以“胃肠起搏”理论为依据[11],结合音乐的特性,利用现代电子技术产生与正常人体胃肠基本电节律相似的胃肠生物电信号,使胃肠起搏点跟随正常的蠕动规律,加强胃的慢波活动,恢复正常的胃电节律和波幅[12]。数字化音乐胃电起搏可以输出音乐、合成数字化音乐胃电起搏刺激信号和原始音乐刺激信号,在头戴耳机聆听音乐的同时,接受电极输出的上述两种刺激信号,并与人体胃本身起搏节律叠加在一起,获得胃起搏、音乐治疗、胃肠动力相关穴位刺激、神经调节、免疫调节等多重效果,从而达到治疗疾病的目的。
数字化音乐胃电起搏发挥作用的机制可能与其纠正异常胃电节律、抑制异位起搏点、促使慢波偶联、加快慢波的传播速度、协调餐后的电-机械偶联和调节胃肠激素的分泌有关。Gallas等[13]研究认为FD患者经胃电刺激后,生长素释放肽增加,可明显改善患者食欲;Qin等[14]的研究显示,胃起搏可通过迷走神经的中央神经元来改善胃动力障碍,还可通过调节食管下端括约肌和Oddi括约肌压力[15-17]来纠正异常胃肠电节律,从而改善胃肠电活动参数。有研究发现,胃肠起搏的作用机制与交感神经、肠神经系统功能活动改变也有关,胃电起搏后肠神经可进行自主调节,也可能与直接或间接兴奋Cajal间质细胞,并改变其跨膜电位或作用于慢波电位有关[18-20]。Zhang等[21]则提出胆碱能神经电刺激可诱发胃部强烈收缩,且胆碱能神经释放的乙酰胆碱作用于Cajal间质细胞可影响起搏频率。
在数字化音乐胃电起搏治疗中,音乐部分改善顽固性FD重叠NERD患者症状的可能机制如下。一是音乐电流是不规则的,当其与超低频胃肠起搏信号叠加时,其节律随着音乐旋律及胃肠肌电活动,胃肠动力节律性、传导性及排空信息的变化而变化,人体不易产生适应性,可实现更好的临床疗效。二是不同的音乐可产生不同的生理、心理效应,调节内脏和躯体功能,改善神经、内分泌功能及改善情绪等,从而达到消除心理障碍、恢复或增进心身健康的目的[22-23]。Sacks等[24]和Peretz等[25]的研究表明,音乐疗法可影响与认知和情感事件相关的不同神经元及核团之间的相互作用,如通过作用于大脑边缘系统和中枢网状结构,改善患者的负面情感表达和感受。Chen等[26]指出音乐疗法也可降低肿瘤患者的焦虑、抑郁及收缩压水平。
总之,本研究表明,数字化音乐胃电起搏治疗顽固性FD重叠NERD有明显疗效,且能明显改善患者抑郁、焦虑状态。以胃肠起搏的治疗原理为基础的数字化音乐胃电起搏为此类疾病的临床治疗提供了新的视角。
[1] Ghoshal UC, Singh R, Chang FY, et al. Epidemiology of univestigated and functional dyspepsia in Asia: facts and function[J]. J Neurogatigastroenterol Motil, 2011, 17(3): 235-244.
[2] Lee SW, Lien HC, Lee TY, et al. Heartburn and regurgitation have different impacts on life quality of patients with gastroesophageal reflux disease[J]. World J Gastroenterol, 2014, 20(34): 12277-12282.
[3] Noh YW, Jung HK, Kim SE, et al. Overlap of erosive and nonerosive reflux diseases with functional gastrointestinal disorders according to Rome Ⅲ criteria[J]. Neurogastroenterol Motil, 2010, 16(2): 148-156.
[4] Li Y. Diagnosis and treatment of non-erosive reflux disease[J]. Chin J Pract Intern Med, 2010, 30(8): 697-700. [李岩. 非糜烂性反流病的诊断与治疗[J]. 中国实用内科杂志, 2010, 30(8): 697-700.]
[5] Wei YL, Ren XJ, Liu F, et al. Exploring the effect of vibroacoustic massotherapy on improving the psychosomatic symptoms in patients with functional dyspepsia[J]. Chin J Tradit Chin Med Pharm, 2008, 23(4): 350-352. [魏育林, 任晓静, 刘芳, 等. 音乐声波按摩治疗改善功能性消化不良患者心身症状的临床探讨[J]. 中华中医药杂志, 2008, 23(4): 350-352.]
[6] Yang B, Hou XH, Song GQ, et al. Effect of two-channel gastric electrical stimulation with trains of pulses on gastric motility[J]. World J Gastroenterol, 2009, 15(19): 2406-2411.
[7] Vakil N, Van Zanten SV, Kahrilas P, et al. The Montreal definition and classification of gastroesopgageal reflux disease: A Global Evidence-based consensus[J]. Am J Gastroenterol, 2006, 101(8): 1900-1920.
[8] Yan B, Cui LH, Peng LH, et al. An epidemiological research and risk factor analysis of functional gastroduodenal disorders in a Chinese naval force[J]. Med J Chin PLA, 2013, 38(6): 446-449.[闫斌, 崔立红, 彭丽华, 等. 海军某部官兵功能性胃十二指肠疾病的流行病学调查及影响因素分析[J]. 解放军医学杂志, 2013, 38(6): 446-449.]
[9] Allescher HD. Functional dyspepsia--a multicausal disease and its therapy[J]. Phytomedicine, 2006, 13(Suppl 5): 2-11.
[10] Bruley des Varannes S, Coron E, Galmiche JP. Short and longterm PPI treatment for GERD. Do we need more-potent antisecretory drugs[J]? Best Pract Res Clin Gastroenterol, 2010, 24(6): 905-921.
[11] Takayama I, Horiguchi K, Daigo Y, et al. Theinterstitial cells of Cajal and a gastroenteric pacemaker system[J]. Arch Histol Cytol, 2002, 65(1): 1-26.
[12] Wang ZS, Cheung JY, Gao SK, et al. Spatio-temporal nonlinear modeling of gastric myoelectrical activity[J]. Methods Inf Med, 2000, 39(2): 186-190.
[13] Gallas S, Fetissov SO. Ghrelin, appetite and gastric electrical stimulation[J]. Peptides, 2011, 32(11): 2283-2289.
[14] Qin C, Sun Y, Chen JD, et al. Gastric electrical stimulation modulates neuronal activity in nucleus tractus solitarii in rats[J]. Auton Neurosci, 2005, 119(1): 1-8.
[15] Kuramoto H, Kadowaki M, Yoshida N. Morphological demonstration of a vagal inhibitory pathway to the lower esophageal sphincter via nitrergic neurons in the rat esophagus[J]. Neurogastroenterol Motil, 2013, 25(7): e485-e494.
[16] Lang IM, Medda BK, Shaker R. Differential activation of medullary vagal nuclei caused by stimulation of different esophageal mechanoreceptors[J]. Brain Res, 2011, 1368: 119-133.
[17] Xing J, Felsher J, Brody F, et al. Gastric electrical stimulation significantly increases canine lower esophageal sphincter pressure[J]. Dig Dis Sci, 2005, 50(8): 1481-1487.
[18] Li C, Liu S, Guan Y, et al. Long pulse gastric electrical stimulation induces regeneration of myenteric plexus synaptic vesicles in diabetic rats[J]. Neurogastroenterol Motil, 2010, 22(4): 453-461.
[19] Sun Y, Song GQ, Yin J, et al. Effects and mechanisms of gastrointestinal electrical stimulation on slow waves: a systematic canine study[J]. Am J Physiol Regul Integr Comp Physiol, 2009, 297(5): R1392-R1399.
[20] Zhang J, Sha W, Zhu H, et al. Blunted peripheral and central responses to gastric mechanical and electrical stimulations in diet-induced obese rats[J]. J Neurogastroenterol Motil, 2013,19(4): 454-466.
[21] Zhang RX, Wang XY, Chen D, et al. Role of interstitial cells of Cajal in the generation and modulation of motor activity induced by cholinergic neurotransmission in the stomach[J]. Neurogastroenterol Motil, 2011, 23(9): 356-371.
[22] Li TJ, Shao H, You LY, et al. Clinical application of music therapeutics[J]. J Pract Diagn Ther, 2006,(5): 355-356. [李铁菊, 韶红, 游丽莹, 等. 音乐疗法的临床应用[J]. 实用诊断与治疗杂志, 2006,(5): 355-356.]
[23] Solanki MS, Zafar M, Rastogi R. Music as a therapy: Role in psychiatry[J]. Asian J Psychiatr, 2013, 6(3): 193-199.
[24] Sacks O. The power of music[J]. Brain, 2006, 129 (10): 2528-2532.
[25] Peretz I, Zatorre RJ. Brain organization for music processing[J]. Annu Rev Psychol, 2005, 56: 89-114.
[26] Chen LC, Wang TF, Shih YN, Wu LJ. Fifteen-minute music intervention reduces pre-radiotherapy anxiety in oncology patients[J]. Eur J Oncol Nurs, 2013, 17(4): 436-441.
Therapeutic efficacy of digital music gastric electrical pacing for refractory functional dyspepsia concomitant with non-erosive reflux disease
RAN Ya-mei1, LIN Ling1, HE Yu-Qin1, CHEN Qiang1, JI Lei1, LANG Xiu-qiong1, HUANG Zhi-yong2, YANG Min11Department of Gastroenterology, Institute of Field Surgery, Daping Hospital, Third Military Medical University, Chongqing 400042, China
2Communication Engineering, Chongqing University, 400030 Chongqing, China
*
, E-mail: yangmindoctor@163.com
This work was supported by the Science Achievements Transformation Fund of Third Military Medical University (2010XZH-11/2013XZH-07)
ObjectiveTo study the clinical efficacy of digital music gastric electrical pacing for refractory functional dyspepsia concomitant with non-erosive reflux disease, and its effects on mental health and life-quality of the patients.MethodsAccording to the Rome Ⅲ criteria and Montreal consensus in diagnosis of gastroesophageal reflux disease, 50 patients with concomitant refractory functional dyspepsia and non-erosive reflux disease were recruited. The clinical efficacy of digital music gastric electrical pacing were evaluated using the score of clinical symptoms before treatment and 15 days after treatment, and the mental health and life-quality of patients were assessed using symptom checklist 90.ResultsMain symptoms, including upper abdominal pain, abdominal fullness, early satiety, belching, hiccup, nausea, heartburn, acid reflux (daytime), nocturnal acid reflux, loss of appetite and sleep, were significantly improved 15 days after treatment compared with those of pre-treatment, and there were statistically significant differences (all P<0.005). The significant response rate / response rate (efficacy rate) were 59.0%/100.0%, 59.3%/96.3%, 47.0%/94.1%, 61.3%/96.8 %, 86.7%/100.0%, 80.0%/100.0%, 64.3%/92.9%, 73.7%/89.5%, 64.3%/85.7%, 90.0%/90.0%, 36.7%/93.3% respectively. After treatment for 15 days, the overall response rate of symptom relief was 94.4% in patients and the overall significant response rate was 65.7%. The symptom scores of somatization, obsessive-compulsiveness,depression, and anxiety were significantly improved, and the differences were statistically significant (all P<0.01).ConclusionThe clinical efficacy of digital music gastric electrical pacing is significant for refractory functional dyspepsia concomitant with nonerosive reflux disease, and it is expected to be a new option for the treatment of this disease complex.
dyspepsia; gastroesophageal reflux; gastric electrical pacing
R573.9
A
0577-7402(2015)03-0212-05
10.11855/j.issn.0577-7402.2015.03.08
2014-12-15;
2014-2-18)
(责任编辑:熊晓然)
第三军医大学科技成果转化基金(2010XZH-11/2013XZH-07)
冉亚梅,硕士研究生。主要从事功能性胃肠病及胃肠动力障碍性疾病的基础及临床研究
400042 重庆 第三军医大学大坪医院野战外科研究所消化内科(冉亚梅、林玲、何雨芩、陈强、纪雷、郎秀琼、杨敏);400030 重庆 重庆大学通信工程学院(黄智勇)
杨敏,E-mail: yangmindoctor @163.com
·信 息·
