Magnifying endoscopic diagnosis of digestive erosions
2011-05-16肯塔穆罕默德许树长
(肯塔·穆罕默德),(许树长)
Department of Gastroenterology,Tongji Hospital,Tongji University,School of Medicine,Shanghai 200065,China
Magnifying endoscopic diagnosis of digestive erosions
Keita Mohamed(肯塔·穆罕默德),Xu Shuchang(许树长)
Department of Gastroenterology,Tongji Hospital,Tongji University,School of Medicine,Shanghai200065,China
Magnifying endoscopy is used to visualize the microstructure and microvascular architecture of gastrointestinal surface mucosa.Microsurface structure of the mucosa includes normal structure,changed structure by inflammation and biological response.Magnifying endoscopy is starting to play an important role in diagnosis of any upper gastrointestinal diseases by assessment of magnified observation.Magnifying endoscopy holds a great deal of promise in the near future because magnifying endoscopic observation is approaching optical biopsy[1].The aim of this review is to describe recent advances in endoscopic technology and to review the available literature pertaining to the clinical application of these techniques in the diagnosis of digestive erosions diseases.
magnifying endoscopy;erosions;microstructure;microvascular architecture
Identification of pathology by standard electronic video endoscopes depends on the presence of various mucosal lesions such as erosions,plaques,nodules,or ulcers.Certain conditions can be missed on standard endoscopy because they may have very subtle mucosal changes.In recent years,further improvements in the quality and diagnostic ability of the endoscopic image have been the subject of many technological developments.Recent technological advances in miniaturization have allowed for a confocal scanning microscope to be integrated into trans-endoscopic probes enabling endoscopists to see and collect in vivo virtual biopsies of the gastrointestinal mucosa during endoscopy.
1 Term and Concept
Erosions are frequent pathological manifestation of the gastro-duodenal tract.They are often found in histology specimens specially in gastro-intestinal diseases(esophagus,stomach and duodenum).They occur in various pathologic conditions as well for no apparent reason.Frequently they are epiphenomena,accompanying other lesions.Many histological types of erosion are minute and cannot be identified with standard white-light endoscopy,only with magnification or vital staining.With endoscopy,the frequency of detection is even higher according to Kawai et al[2].The term erosion has been a major problem of endoscopic terminology,similar to the term“gastritis”.Endoscopically this term is acceptable only if the endoscopic criteria are sufficient for identifying the lesions with reasonable certainly.Erosion is essentially an acute lesion that elicits a prompt reaction and quick regeneration of the injured epithelium in a few hours or days without trace.It is an acute flat defect of the mucosa,which don’t penetrate beyond the muscularis mucosa.This is in contrast to an ulcer which heals with a scar[3].
Endoscopic criteria of mucosal erosions
The defect as such cannot be visualized because it is too shallow.The characteristic feature enabling diagnosis is the presence of exudates covering the defect.It consists of blood components and fibrin.According to the proportion of both constituents,it appears as a fleck on the mucosa,either red(hemorrhage)or yellow(fibrin).After a few hours the blood is clotted or hemolyzed or forms as hematin crust.Fibrin also shrinks into a yellowish lining sticking on the defect.If bleeding prevails,the erosion is designated as hemorrhagic.Later on the remnants of blood may get under the regenerated superficial epithelium and form a petechia or a pigment spot.If fibrin prevails,the erosion is designated as aphthous.As to the shape,erosion are linear or round,and their diameter usually does not exceed a few millimeters.More exten-sive sub epithelial hemorrhages are called ecchymosed or suffusions.In contrast to an ulcer,which is characterized by a distinct base and border,an erosion appears as a fleck with a rather indistinct margin.The difference between the two lesions includes the possibility of drawing an erosion with surrounding mucosa into the lumen with a forceps,in contrast to the ulcer,which firmly adheres to the wall.It has been said that an erosion is essentially an acute lesion.In the present literature the term chronic erosion has been used for a conical elevation 2 to 8 mm in diameter,which has a hemorrhage or aphthous erosion on the top or simply an umbilicated depression.Such a lesion has also been referred to as a raised,elevated,complete or varioliform erosion.This designation is based on the assumption that the erosion is the primary lesion,which results in elevation of the surrounding mucosa.However,the elevation is the primary phenomenon due to accumulation of material within the mucosa which protrudes into the lumen and bursts.The hole through which it empties appears as an erosion,but it is a secondary epiphenomenon.The defect seals with a hematin or fibrin plug,and after reepithelization appears as an umbilicated depression.According to this concept,the erosion is a transient phenomenon in the active stage of the lesion whereas the conical umbilicated elevation is a lasting sequella.With regard to the ensuing confusion,Chronic erosion has been avoided to an adequate descriptive term“papule,”which points to the characteristic endoscopic feature of the lesion.Further attributes specify the lesion as a hemorrhagic papule with a hemorrhagic erosion on the top,an aphthous papule with an aphthous erosion on the top,and an umbilicated papule with an umbilicated depression[4,5].
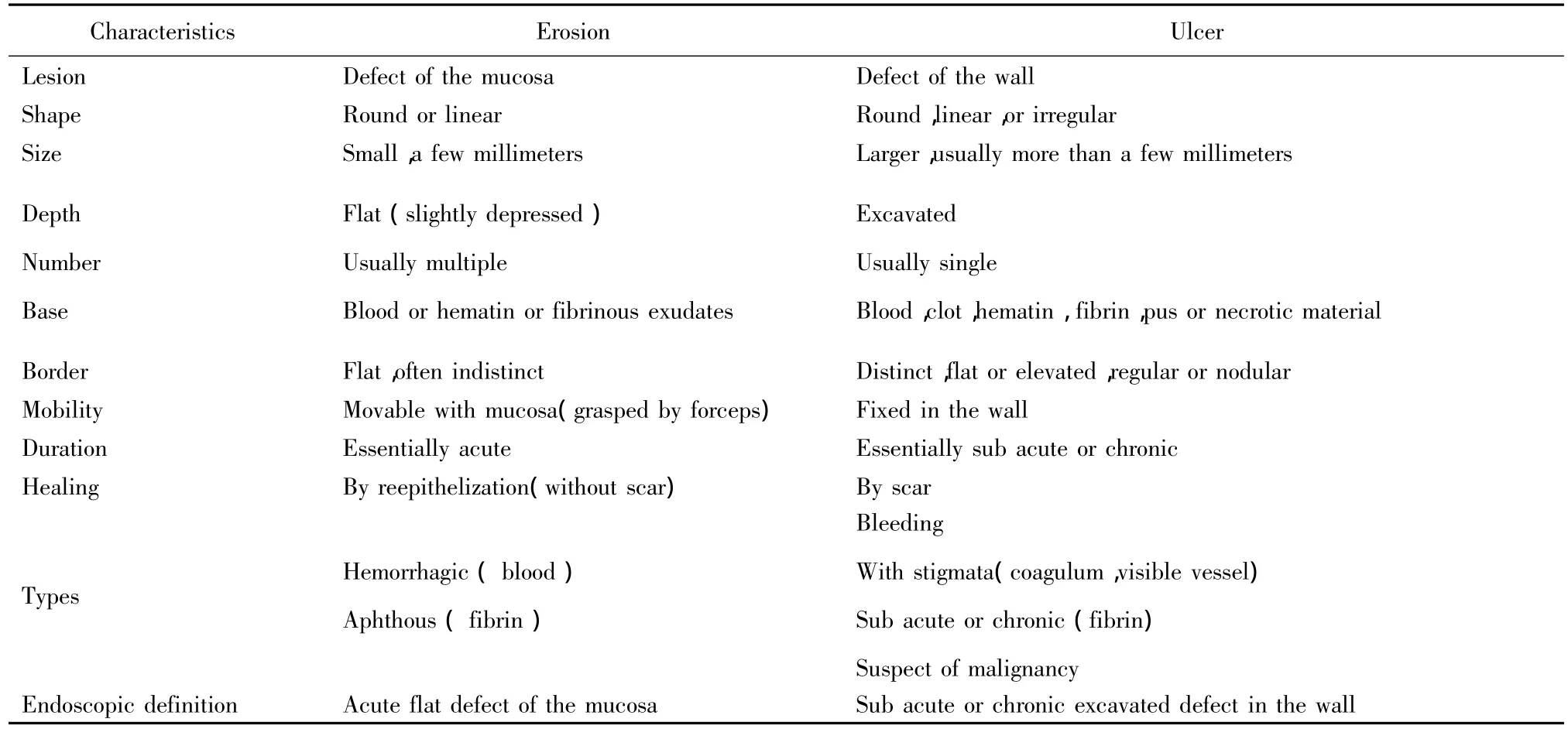
Table 1 Endoscopic characteristics of erosion and ulcer
2 The diagnosis methods of erosions lesions
The gastrointestinal diseases cited above in clinical expression are due to primary or secondary erosive lesions of the gastric mucosa.The most diagnostic methods of investigation are through direct biopsies(esophagus,antrum or the body)by the magnifying endoscopy,highlighting the loss of substances from the mucosa.
2.1 In the pharynx and esophagus
Using standard white-light endoscopy,certain conditions such as erosions,nodules,plaques or ulcers can be missed.In addition,the diagnosis of the pathology might not be always accurate[9].Recently,magnifying endoscope has been used clinically for its developments in amplifying power with the intention of improving the overall accuracy of endoscopy and biopsy.With this technique,good endoscopic visualization of the mucosa is ob-tained but adequate endoscopic biopsies are more difficult to obtain and often too superficial to make a diagnosis in this areas[6-8].
2.2 In the stomach and colon
The endoscopic appearances of the stomach and colon are poorly known by using standard white light endoscopy.It’s still controversial whether certain macroscopic endoscopic features can be used to diagnose Helicobacter pylori(HP)related gastritis.There is a great deal of ignorance about the normal macroscopic appearance of the gastric mucosal lining.In all probability many of the appearance which endoscopists interpret as“Normal”are presumably not normal.Endoscopic findings such as erythema are frequently labeled as gastritis despite a long recognized lack of evidence supporting a correlation between endoscopic features and histologic gastritis..Gastric mucosal atrophy could be identified by routine endoscopy usually when it was at more severe grade.Under magnifying endoscopy,disordered structures,deficiency and even disappearance of gastric pits are in high detection and accuracy for atrophic gastritis.As to mild and moderated grades of atrophy,the diagnosis by magnifying endoscopy may be higher than that by routine endoscopy[9-11].

Table 2 Diagnosis by magnifying endoscopy in upper GI tract
2.3 In the small intestine
Endoscopic examination of the small intestine with standard endoscopy for detection of erosive lesions is very difficult.The upper and pan endoscopy ileocolonoscopy do consider the very small portion of proximal small intestine,distal respectively.In m,ost clinics instead,a colonoscope may be used as a partial enteroscopy with probes and special endoscopic techniques.Endoscopic images obstenues of intestinal erosions were reliable and well interpreted with a good preparation[12,13].
3 Clinical application of confocal scanning endoscope
Confocal laser scanning is a cutting-edge endoscopic procedure that enables the surface of the gastrointestinal mucosa to be microscopically examined during the endoscopy.With Confocal scanning,the physician is able to make a real-time diagnosis of different GI diseases[14-16].
New model of electronic magnifying endoscope GIF Q-240Z(Olympus Optical Co.,Ltd.,Tokyo,Japan)the Pentax EG-3870CIK(upper endoscope)and EC-3870CILK(colonoscope(Pentax,Tokyo,Japan)was used.It could be used to perform routine endoscopy(observation at standard magnification)as well as to magnify the image 80 times[17-19].
Confocal laser endoscopy is a novel topic in the field of digestive endoscopy to diagnose minute erosions lesions in gastric mucosa by magnifying endoscopy with a high degree of accuracy and can facilitate rapid diagnosis during routine endoscopy.
3.1 In the esophagus and pharynx
Endoscopy is a widely used diagnostic tool for several different inflammatory and neoplastic pathologies of the mucosa of the esophagus.Unfortunately,it is quite difficult to detect these lesions under the standard white light endoscopy especially in patients with minimal change esophageal reflux disease(MERD),but also particularly by inexperienced endoscopists(kappa value for interobserver agreement by inexperienced endoscopist for minimal change was reported to be low and ranged be-tween 0.19 and 0.36).In the oropharyngeal area so far the tongue is the only region that can be see by this new technique.
Over a few years,endoscopic technologies have evolved tremendously including high resolution and magnification digital chromoendoscopy.These technologies are practically useful for detecting various subtle lesions along the gastrointestinal(GI)tract starting from esophagus to colon.Other than the detection of subtle change reflux esophagitis,Standard,simple and precise endoscopic reading criteria for the identification of MERD are also required,these have proven to be beneficial for Barrett’s epithelium detection,targeted biopsy of the suspicious area in gastric intestinal metaplasia and detecting early gastric and colon cancers.
Confocal Laser Scanning is an important tool with a high potential for GERD diagnosis particularly for MERD since it provides the endoscopist with a simple,safe and rapid method for a better detection of subtle esophageal lesions.This technology is suitable for epithelial evaluation of the anterior parts(buccal area,tongue,and door of the mouth).
In our speculation,over the next few years it may become a standard tool for GERD and MERD diagnosis in clinical practice[20-23].
3.2 In the stomach and colon
The fine detail of the structure of the gastrointestinal mucosa is not delineated during conventional white light endoscopy.Recent advances in endoscopy have facilitated the detection of the diseases.
In gastrointestinal endoscopy,magnifying endoscope have primarily been utilized to enhance the detection of diseased areas,to guide endoscopics biopsies,and to obtain better visual diagnosis or characterization of small abnormalities.The distal border of the normal fundic type of mucosa in the stomach can be recognized easily because of the differences in mucosal characteristics and the pattern of the gastric area.A small erosion which produces a very shallow depression without elevation of the surrounding mucosa is very difficult to detect endoscopically.With this new technique,it is effective to recognize such lesions and to define their size,shape,number and distribution in the detection of early gastric cancer,especially of minute diagnosis and typeⅡb carcinoma(superficial flat type),and in recognizing the extent of cancer infiltration.
This new tool is useful in differentiating benign from malignant ulcers and may aid in determining whether or not an ulcer is recurrent by direct in vivo identification of Helicobacter pylori infection.
In patients with suspected celiac disease,confocal endomicroscopy can demonstrate villous atrophy and an increased number of intraepithelial lymphocytes,enabling immediate in vivo diagnosis of celiac disease.The presence of neoplastic changes in a colonic mucosa can be predicted with high accuracy.Confocal Laser Scanning has several potential roles in polyp management from adenomatous polyps by surface characteristics to the flat neoplasms of the colon.In patients with long-term ulcerative colitis,chromoscopy with supplemental CEM has recently been shown to further increase the yield for intraepithelial neoplasia.Magnifying endoscopy has also the capacity to differentiate normal from inflamed tissue,and thus target biopsies for the purpose of grading and mapping the extent of colitis.Confocal Scanning can also be helpful for the diagnosis of microscopic colitis in patients with chronic diarrhea.In patients with collagenous colitis,it allows direct in vivo visualization of collagenous bands under the epithelial layer of the colon,and in patients with lymphocytic colitis,it can demonstrate crypt distortion and an increased distance between the colonic crypt.Thus,Confocal Scanning has the potential to replace or direct a large number of random biopsies in patients with chronic diarrhea,where the confocal image is normal[24-26].
4 Conclusion
The elaboration of a precise and clear diagnosis of gastrointestinal erosive disease has often been a major problem.It has become a source of confusion and incomprehension in the area of endoscopy because many histological erosions are minute and therefore cannot be identified using standard white-light endoscopy.In the region pharyngeal-esophagus as in the stomach and colon establishment adequate and clear diagnosis has always been a difficult problem and in correlation with histological biopsy.With the recent progress of science in the medical imaging,precision and overall good Interpretation of endoscopic images confocal laser endoscopy is used with precision and overall good interpretation of endoscopic images.
Confocal scanning is a rapidly emerging field of gastroenterology that bridges the interface between endoscopy and histology by magnifying endoscopy with a high degree of accuracy and can facilitate rapid diagnosis during routine endoscopy.It further expands our ability to image living tissue in real time and to provide therapy in the same setting.The main advantages of the advanced endoscopic imaging techniques in the management of gastrointestinal lesions are to identify abnormal mucosal and vascular patterns,to obtain targeted biopsy samples from high-yield areas,and perhaps to avoid biopsy samples from non dysplastic areas.
It is a novel topic in the field of digestive endoscopy to diagnose minute lesions in gastric mucosa by magnifying endoscopy.High resolution magnifying is superior to standard endoscopy for the diagnosis of H.pylori gastritis,and identification of specific histopathology features such as atrophy and intestinal metaplasia seems possible[27-32].Magnifying endoscopy therefore holds a great deal of promise in the near future since observation is now approaching optical biopsy.
Abbreviation
GERD:gastro esophageal reflux disease
MERD:Multiple esophageal reflux disease
CEM:confocal endomicroscopy
LPRD:Laryngopharyngeal reflux disease
IM:intestinal metaplasia
SCC:Squamous cell carcinoma
[1] Mototsugu Kato,Yuichi Shimizu,Souichi Nakagawa,et al.Usefulness of magnifying endoscopy in upper gastrointestinal tract:history and recent studies.Japan J.Endosc,2007,05.15;1443 -1661.
[2] Kawai K,Shimamoto K,Misaki F,et al.Erosion of gastric mucosa - pathogenesis,incidence and classification of the erosive gastritis.Endoscop,2008,3:165 -174.
[3] Zdenek Mafatka,MD,Endoscopic:Definition,diagnostic criteria and terminology of mucosal lesions,World organization of digestive endoscopy,hepatogastroenterology,2007,AB 42 -65.
[4] Curvers WL,Singh R,Song LM,et al.Endoscopic trimodal imaging for detection of early neoplasia in Barrett’s oesophagus:a multi-centre feasibility study using high-resolution endoscopy,auto fluorescence imaging and narrow band imaging incorporated in one endoscopy system.Gut,2008,57:167 -72.
[5] Bevacizumab MD.Painful cervical esophageal erosion in a patient with advanced colorectal cancer treated with Bevacizumab.Endoscop,2008,76:345 -639.
[6] Curvers WL,Singh R,Song LM,et al.Endoscopic trimodal imaging for detection of early neoplasia in Barrett’s oesophagus:a multi-centre feasibility study using high-resolution endoscopy,autofluorescence imaging and narrow band imaging incorporated in one endoscopy system.Gut,2008,57:167 -72.
[7] Giovanni D De Palma.The endoscope-based confocal laser endomicroscopy(CLE),imaging system:the distal tip.World J Gastroenterol,2009,14,15,46,1007 -9327
[8] Savio C,Reddymasu MD,Prateek Sharma MD Advances in Endoscopic Imaging of the Esophagus Gastroenterol Clin N Am,2008,37:763 -774
[9] Giovanni D De Palma.Confocal laser endomicroscopy in the“in vivo”histological diagnosis of the gastrointestinal tract,World J Gastroenterol,2009,14,15,46,1007-9327.
[10] Gonen Can,Simsek Ilkay,Sarioglu,et al.Comparison of High Resolution Magnifying Endoscopy and Standard Videoendoscopy for the Diagnosis of Helicobacter pylori Gastritis in Routine Clinical Practice:A Prospective Study Helicobacter.Gastroenterol,2009,14(1):12 -21.
[11] Jian-Min Yang,Lei Chen,Yu-Lin Fan,et al.Endoscopic patterns of gastric mucosa and its clinicopathological significance.World J Gastroenterol,2007,9(11):2552-2556.
[12] Khan MQ,Alhomsi Z,Al-Momen S,et al.Endoscopic features of Helicobacter pylori induced gastritis.Saudi J Gastroenterol,2010,22(5):9 -14.
[13] Moriyama T,Matsumoto T,Hirakawa K,et al.Helicobacter pylori status and esophagogastroduodenal mucosal lesions in patients with stage renal failure on maintenance hemodialysis.J Gastroenterol,2010,45(5):515-22.
[14] Tadataka Yamada,David H Alpers,Anthony N Kalloo,et al.Atlas of Gastroenterology.4thedit,2009,ISB:978-1-405-16909-7
[15] Faisel D O,Kochman M L.Gastrointest.Endoscopy and cancer management;Endoscopic oncology Humana.Press,2007,1 -58829532 - X.
[16] Kaise M,Kato M,Urashima M,et al.Magnifying endoscopy combined with narrow-band imaging for differential diagnosis of superficial depressed gastric lesions.Endoscopy,2009,41:310 -315.
[17] Dunbar K,Canto M.Confocal endomicroscopy.Curr Opin Gastroenterol,2008,24:631 -637.
[18] Kiesslich R,Goetz M,Neurath MF.Confocal E Laser and Virtual histology Best Pract Res Clin Gastroenterol,2008,22:88 -3897.
[19] Nguyen NQ,Leong RW.Current application of confocal endomicroscopy in gastrointestinal disorders.J Gastroenterol Hepatol,2008,23:1483 -1491.
[20] Becker V,von Delius S,Bajbouj M,et al.Intravenous application of fluorescein for confocal laser scanning microscopy:evaluation of contrast dynamics and image quality with increasing injection-to imaging time.Gastrointest Endosc,2008,68:319 -323.
[21] Goetz M,Kiesslich R,Dienes H,et al In vivo confocal laser endomicroscopy of the human liver:a novel method to assess liver micro architecture in real time.Endoscopy,2008,40(7):554 -562.
[22] Chaiteerakij R,Rerknimitr R,Kullavanijaya P.Role of digital chromoendoscopy in detecting minimal change esophageal reflux disease.World J Gastrointest Endosc,2010,2(4):121 -129.
[23] Kawahara Y,Okada H,Kawano S,Inoue M,Tsuzuki T,Tanioka D,Hori K,Yamamoto K.New digital imaging technology I-Scan for upper GI endoscopy:a pilot study.Gastrointest Endosc,2009,69:AB377.
[24] Hoffman A,Basting N,Goetz M,Tresch A,Mudter J,Biesterfeld S,Galle PR,Neurath MF,Kiesslich R.High definition endoscopy with i-Scan and Lugol’s solution for more precise detection of mucosal breaks in patients with reflux symptoms.Endoscopy,2009,41:107 -112.
[25]Simon Pierre Veilleux:Gastroesophagal reflux and its complications.J Endosc,2008,10 AB 235.
[26] Kiesslich R,Goetz M,Neurath MF.Confocal laser endomicroscopy for gastrointestinal diseases Gastrointest Endosc Clin N Am,2008,18:451 -466.
[27] Dunbar K,canto M Confocal endomicroscopy、Curr Opin Gastroenterology,2008,24(5):631 -637.
[28] Polglase AL,McLaren WJ,Delaney PM.Pentax confocal endomicroscope:a novel imaging device for in vivo histology of the upper and lower gastrointestinal tract.Expert Rev Med Devices,2007,3:549 -556.
[29] Trovato C,Sonzogni A,Rvizza D,et al.Confocal laser endomicroscopy diagnosis of gastric adenocarcinoma in a patient treated for gastric diffuse large B cell lymphoma Digestive and liver Disease,2009,41(6):447 -449,Clin Gastroenterol Hepatol,2008,6(1):89 -94.
[30] Pech O,Rabenstein T,Manner H,et al.Confocal laser endomicroscopy for in vivo diagnosis of early squamous cell carcinoma in the esophagus.J Med Sci,2007,56(5):234-237.
[31] Takeuehi Y,Uedo N,Lishi H,et al.The new diagnostic strategy for detecting gastric neoplasia using autofluorescence imaging videoscopy followed by narrow band imaging with magnifying endoscopy Gastrointest Endoscop,2007,65:AB 336.
[32] Rasmi Y,Sadreddini M,Shahsavari Z,et al.Prevalence of Helicobacter pylori and cytoxin-associated gene A in Iranien patients with non erosive and erosive reflux disease Indian J Med Sci,2009,63(9):402 -407.
